Page 13 of 20
PE17.1 | National Health Mission Programs — SDL Guide (Part 2)
RMNCH+A: The Strategic Framework
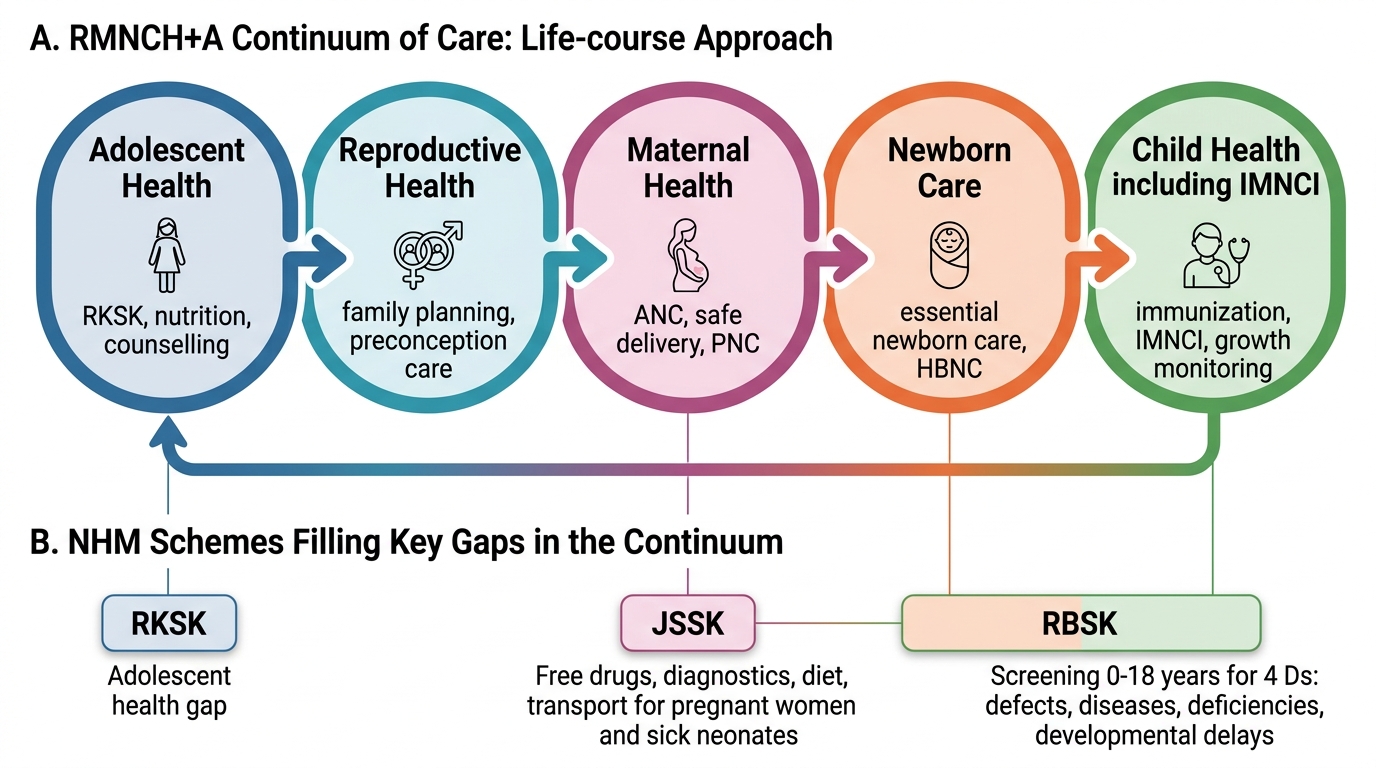
RMNCH+A — Reproductive, Maternal, Newborn, Child and Adolescent Health — is the overarching strategic framework through which NHM delivers its maternal and child health interventions. Launched in 2013 as India's adaptation of the global RMNCH Continuum of Care approach, RMNCH+A explicitly operationalises the life-course principle: health interventions are most effective when they are delivered as a continuum from adolescence through pregnancy, delivery, the neonatal period, childhood, and back to adolescence in the next generation. The central insight of RMNCH+A — borrowed from the Lancet series on neonatal survival and subsequent global analyses — is that child mortality cannot be reduced to sustainable levels by addressing only one segment of the continuum while neglecting others. A country that invests heavily in skilled birth attendance but does not provide postnatal care will see gains in intrapartum deaths plateau without further reduction in neonatal deaths. A country that immunises well but does not address maternal anaemia will continue to see low birth weight as a driver of neonatal mortality. RMNCH+A therefore mandates that all five strategic areas be addressed simultaneously, with the same community health workers and facility staff serving as the delivery mechanism across the full lifecycle.
The framework is organised around five strategic areas:
- Reproductive Health: contraception, family planning, STI/RTI management — to ensure that every pregnancy is planned and healthy.
- Maternal Health: antenatal care (minimum 4 ANC contacts per MoHFW guideline, now 8 per WHO 2016 but India at 4+), institutional delivery promotion, skilled birth attendance, emergency obstetric care, postnatal care. JSSK is the financial entitlement that makes maternal health services free.
- Newborn Care: HBNC visits (days 1, 3, 7, 14, 28 by ASHA), facility-based newborn care corners in all delivery facilities (warmth, resuscitation equipment, early exclusive breastfeeding promotion), SNCU (Special Newborn Care Units) at district hospitals for sick neonates.
- Child Health: IMNCI as the clinical case-management tool; RBSK for screening and early intervention; immunisation (NIS + Mission Indradhanush); nutrition (ICDS + NRC for SAM); ORS/zinc cornerstone.
- Adolescent Health: RKSK programme — see below.
The defining feature of RMNCH+A is the continuum-of-care principle: each of the five strategic areas feeds into the next — a healthy, well-nourished adolescent is more likely to have a healthy pregnancy; a well-managed delivery reduces neonatal sepsis risk; a newborn receiving HBNC will be more likely to survive to childhood; and so on. Interrupting the continuum at any point — for example, poor neonatal care despite good antenatal care — results in preventable deaths.
RMNCH+A Continuum of Care and Supporting NHM Schemes
RBSK, RKSK and JSSK: Programme Details
Three major NHM child health schemes complement RMNCH+A's overarching framework: RBSK for early identification of birth defects and developmental problems, RKSK for adolescent health, and JSSK for financial protection of mothers and sick neonates. Each addresses a specific gap in the MCH continuum that the RMNCH+A framework alone — operating through the ANC/delivery/HBNC pathway — was insufficient to fill. RBSK fills the gap of silent, undetected disability in the first 18 years of life: a child with congenital heart disease or developmental delay would go undetected in a passive, symptom-driven health system unless actively screened. RKSK fills the gap of adolescent health — a population largely invisible in India's earlier MCH architecture that focused on under-5s and pregnant women. JSSK fills the financial barrier gap: even when a woman wanted to deliver in a government facility, user charges for drugs, diagnostics, and transport were a substantive deterrent in low-income households. Removing these charges through an entitlement-based scheme was the lever that shifted India's institutional delivery rate from 40% to nearly 80% in 15 years.
Provided image
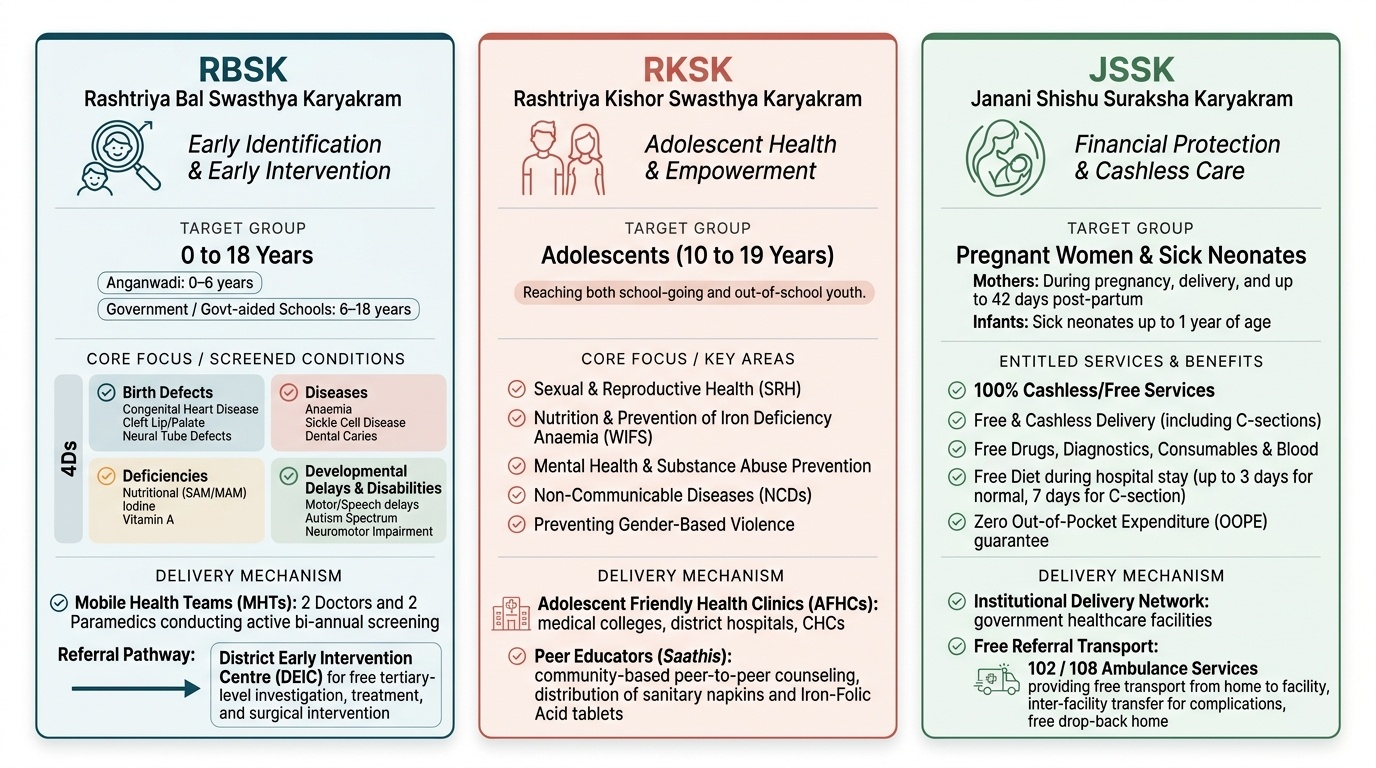
RBSK — Rashtriya Bal Swasthya Karyakram (National Child Health Screening and Early Intervention Programme):
Launched in 2013, RBSK aims to provide free health screening and early intervention for all children from birth to 18 years. The target conditions are grouped as the 4Ds:
• Birth Defects — congenital heart disease, cleft lip/palate, neural tube defects, hearing impairment, congenital cataract, talipes
• Diseases — anaemia, sickle cell disease, dental caries, vitamin D/A deficiency, rheumatic heart disease
• Deficiencies — nutritional (SAM/MAM), iodine, vitamin A, iron
• Developmental Delays and Disabilities — motor delay, speech/language delay, cognitive delay, autism spectrum, neuromotor impairment
Screening is conducted by Mobile Health Teams (MHTs) — two doctors and two paramedics per team — visiting every Anganwadi (0–6 years) and government school (6–18 years) twice a year. Children identified with conditions requiring further care are referred to the District Early Intervention Centre (DEIC) — a hub facility at the district hospital that coordinates free investigation, treatment, and follow-up.
RKSK — Rashtriya Kishor Swasthya Karyakram:
Launched in 2014, RKSK addresses the health needs of adolescents aged 10–19 years — approximately 253 million Indians. Key components: (1) Adolescent Friendly Health Clinics (AFHCs) at PHC/CHC level offering confidential, non-judgmental counselling on nutrition, menstrual health, sexual and reproductive health, mental health, and substance use; (2) ASHA Facilitators — dedicated ASHAs trained for adolescent outreach; (3) Peer Educator Programme — trained adolescent peers who disseminate health information in schools; (4) Weekly Iron and Folic Acid Supplementation (WIFS) for adolescent girls (60 mg elemental iron + 500 µg folic acid weekly) and albendazole 400 mg every 6 months (deworming) to reduce anaemia before pregnancy.
JSSK — Janani Shishu Suraksha Karyakram:
Launched in 2011, JSSK entitles every pregnant woman delivering in a government facility to: free normal delivery, free caesarean section, free essential drugs and consumables, free diagnostics, free blood transfusion if needed, free diet (3 days for normal delivery, 7 days for C-section), free referral transport (within and between facilities), and exemption from all user charges. Every sick neonate is also entitled to: free treatment, free drugs, free diagnostics, free blood transfusion, free diet for the mother, and free referral transport up to 30 days after birth.
| Programme | Target group | Key feature | Referral hub |
|---|---|---|---|
| RBSK | Birth to 18 years | 4Ds screening by MHTs | DEIC at district hospital |
| RKSK | 10–19 years (adolescents) | AFHCs + WIFS + peer educators | PHC/CHC AFHC |
| JSSK | Pregnant women + sick neonates to 30 days | Free delivery, drugs, transport, diagnostics | Government facility (PHC to tertiary) |
CLINICAL PEARL
The RBSK 4Ds mnemonic is high-yield for NMC examinations. 'RBSK screens for 4Ds: Birth Defects, Diseases, Deficiencies, and Developmental Delays/Disabilities.' A critical point often missed: RBSK is a universal screening programme — it is NOT targeted only at symptomatic children. Every child attending a government Anganwadi or school is screened twice a year by an MHT, regardless of apparent health status. This proactive, population-level approach is what makes RBSK structurally different from the passive facility-based detection of conditions it replaced. When you are a PHC medical officer, you are responsible for supporting the MHT visits in your catchment area and ensuring detected children reach the DEIC — this is a routine administrative duty under NHM, not a specialist referral.
Mission Indradhanush and ICDS
Two NHM programmes specifically target immunisation coverage and child nutrition — the two most powerful preventive health interventions for under-5 mortality.
Provided image
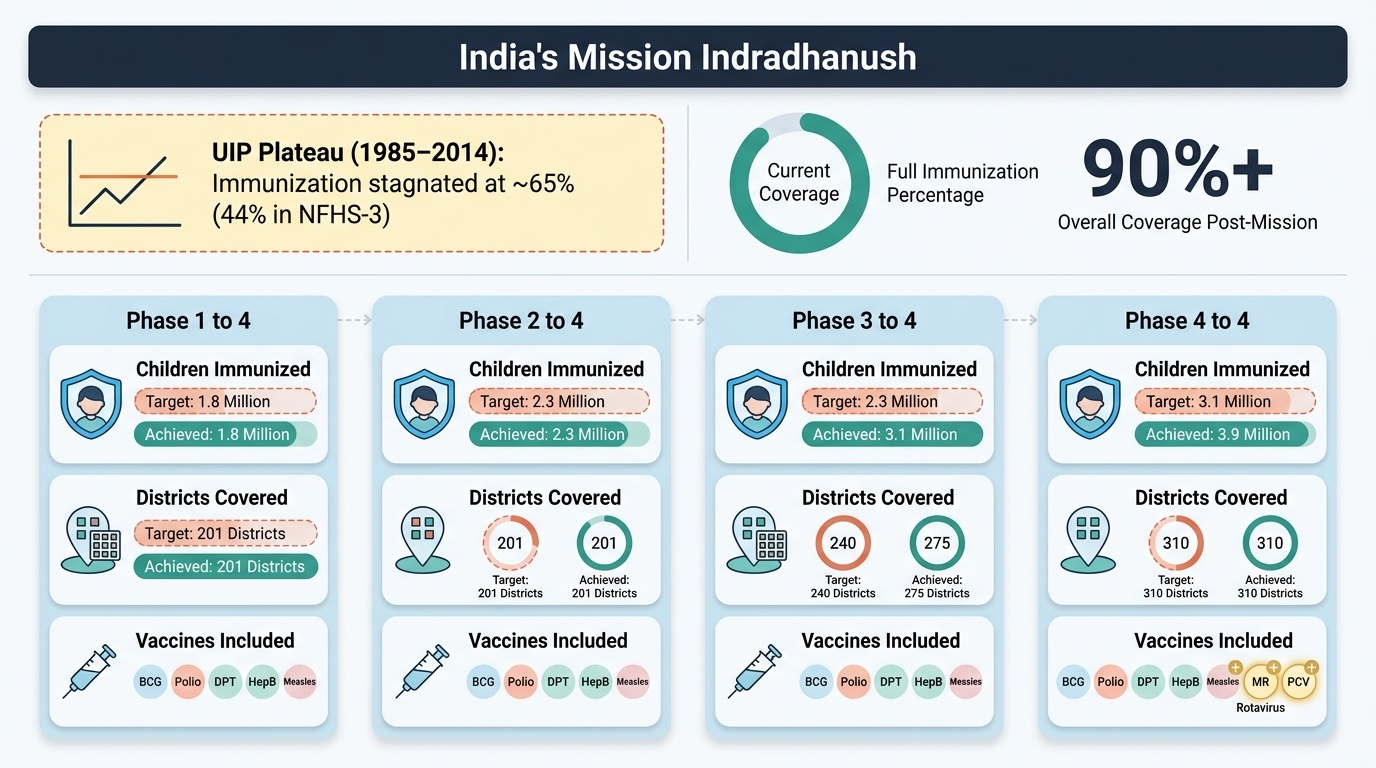
Mission Indradhanush:
Launched in December 2014, Mission Indradhanush was India's response to a persistent immunisation plateau: despite the Universal Immunisation Programme (UIP) operating since 1985, full immunisation coverage in India stagnated at approximately 65% by the mid-2000s and reached only 44% in NFHS-3 (2005-06). Millions of children were either unimmunised or partially immunised — particularly in the 201 high-focus districts where coverage was lowest.
Mission Indradhanush was designed as an intensive catch-up immunisation campaign: health workers actively identified and vaccinated all children under 2 years and pregnant women who had missed or incomplete vaccinations. The programme operates in defined phases — Phase 1 (2015, 201 districts), Phase 2 (2015-16, 352 districts), Phase 3 (2017, 558 districts), and Phase 4 (Intensified Mission Indradhanush 2.0 and beyond, with continued expansion). The mission targeted ≥90% full immunisation coverage as its endpoint — a threshold believed sufficient to establish herd immunity against vaccine-preventable diseases in the routine programme's gaps.
The vaccines included in Mission Indradhanush have expanded progressively to now include all UIP vaccines plus newer additions: Rotavirus vaccine, Pneumococcal Conjugate Vaccine (PCV), IPV (injectable polio), MR (Measles-Rubella), JE (Japanese Encephalitis in endemic districts), and Vitamin A supplementation as part of the catchup.
ICDS — Integrated Child Development Services:
Launched in 1975, ICDS is India's oldest and largest nutrition and early childhood development programme — predating NHM but now fully integrated under it. The programme delivers a package of six services through the Anganwadi Centre (AWC): supplementary nutrition, immunisation, health check-up, referral services, pre-school non-formal education, and nutrition and health education for mothers.
The ICDS target population is children 0–6 years, pregnant and lactating women, and adolescent girls. The Anganwadi Worker (AWW) is the primary implementer — a village-level community worker who provides daily supplementary nutrition (hot cooked meal or take-home ration), weighs children monthly (growth monitoring), conducts early stimulation activities for 3–6 year olds, and maintains the 'Village Health and Nutrition Register' tracking growth, immunisation, and nutrition status.
| Programme | Year | Target | Core intervention | Current status |
|---|---|---|---|---|
| Mission Indradhanush | 2014 | Children <2 yr + PW with missed vaccines | Catch-up intensive immunisation | Ongoing, Phase 4+ |
| ICDS | 1975 | 0-6 yr + PW/LW + adolescent girls | Supplementary nutrition + early education + health | Universal, 14 lakh+ AWCs |
SELF-CHECK
A 4-year-old boy in an Anganwadi is found by the RBSK Mobile Health Team to have suspected congenital hearing loss. Which of the following MOST accurately describes the correct RBSK pathway for this child?
A. Refer to the nearest ENT surgeon at the medical college — RBSK does not have a district-level referral mechanism
B. Document the finding and advise parents to seek private care — government facilities cannot manage hearing impairment
C. Refer to the District Early Intervention Centre (DEIC) at the district hospital, where free audiological assessment, hearing aids, and follow-up are coordinated
D. Re-screen at the next 6-monthly visit — a single visit finding is insufficient for referral
Reveal Answer
Answer: C. Refer to the District Early Intervention Centre (DEIC) at the district hospital, where free audiological assessment, hearing aids, and follow-up are coordinated
Under RBSK, a child found with a suspected condition from the 4Ds is referred to the District Early Intervention Centre (DEIC) — the designated hub at the district hospital that coordinates free assessment, treatment, and long-term follow-up for all conditions detected by RBSK screening. Hearing impairment falls under 'Birth Defects' in the RBSK 4Ds framework. DEIC provides audiological evaluation, fitting of hearing aids (free under RBSK), speech therapy, and parental counselling. Referral to the private sector or medical college bypassing DEIC is not the RBSK pathway. A single clear-cut finding of suspected hearing loss is sufficient to trigger DEIC referral — re-screening without action is inappropriate.