Page 2 of 10
PA20.3 | Multiple Myeloma — Lab Findings & Diagnosis — SDL Guide (Part 2)
Laboratory Findings — The High-Yield Core

Laboratory Findings in Multiple Myeloma
The laboratory findings in myeloma are unusually specific and form the cornerstone of diagnosis.
1. Serum Protein Electrophoresis (SPEP) — M-spike
Monoclonal gammopathy appears as a tall, narrow, sharply demarcated peak (the M-spike) in the γ or β-γ region — in contrast to the broad, diffuse polyclonal hypergammaglobulinaemia seen in infection or inflammation.
• Most common: IgG (~55%), then IgA (~25%)
• Immunofixation electrophoresis (IFE) confirms the M-protein class (IgG/IgA/IgM/IgD/IgE) and light chain type (κ or λ) — it is more sensitive than SPEP for detecting small M-proteins

Diagnostic Features of Multiple Myeloma: Laboratory and Microscopic Findings
2. Bence-Jones Protein (Urine)
Free light chains (κ or λ) are small enough to be filtered by the glomerulus and appear in urine. Bence-Jones protein has the classic heat behaviour: precipitates at 40–60°C, redissolves at 100°C. Urine protein electrophoresis (UPEP) or urine IFE is needed — standard urine dipstick detects albumin, NOT light chains, so a negative dipstick does NOT exclude Bence-Jones proteinuria.
3. Blood Film — Rouleaux and High ESR
Rouleaux formation: erythrocytes stack like coins due to elevated M-protein coating their surfaces and reducing electrostatic repulsion. Blood film shows long chains of RBCs (rouleaux). This directly drives a markedly elevated ESR (often >100 mm/h).

Multiple Myeloma: Key Diagnostic Features
4. Bone Marrow Biopsy
>10% clonal plasma cells in the marrow is a key diagnostic criterion. Morphology: plasma cells with eccentric nucleus, clock-face (cartwheel) chromatin, abundant basophilic cytoplasm, perinuclear hof (Golgi zone). Abnormal forms: multinucleated, flame cells (IgA-secreting), Mott cells (Russell bodies — grape-like Ig inclusions).

Bone Marrow Histopathology: Normal vs. Myeloma Plasma Cells
5. Plain X-Ray / Skeletal Survey
Classic "punched-out" lytic lesions — round, well-defined osteolytic defects with no sclerotic rim, most striking in the skull ("pepper-pot skull"), vertebrae, and long bones.

Multiple Myeloma: Lytic Bone Lesions in Skull (Pepper-Pot Appearance)
6. Other Biochemical Findings
• Total protein elevated (due to M-protein), albumin reduced → reversed albumin-to-globulin (A:G) ratio (normal A:G ~2:1; in myeloma often <1)
• β2-microglobulin (β2M): shed by plasma cells; elevated levels correlate with tumour burden and are a key prognostic marker (high β2M = poor prognosis in the ISS staging system)
• Serum calcium: elevated (CRAB C)
• Creatinine: elevated if renal involvement
• LDH: elevated in high tumour burden
• CBC: normocytic normochromic anaemia; leukopenia and thrombocytopenia in advanced disease
CLINICAL PEARL
The urine dipstick trap — a favourite exam question: standard urine dipstick tests detect ALBUMIN only (they use a colorimetric albumin-binding dye). Bence-Jones protein (free light chains) does NOT bind this dye and therefore gives a NEGATIVE or trace result on dipstick even when urinary light chain levels are very high. Always request urine protein electrophoresis (UPEP) or urine immunofixation in suspected myeloma — do not be falsely reassured by a normal dipstick.
SELF-CHECK
Which of the following laboratory findings is MOST specific for multiple myeloma compared with a reactive plasmacytosis?
A. Elevated ESR
B. Normocytic normochromic anaemia
C. Monoclonal M-spike on serum protein electrophoresis
D. Increased total serum protein
Reveal Answer
Answer: C. Monoclonal M-spike on serum protein electrophoresis
A monoclonal M-spike on SPEP reflects clonal expansion of a single immunoglobulin-producing cell line — the hallmark of a plasma cell neoplasm. Reactive plasmacytosis (seen in infections, connective tissue disease, liver disease) produces a polyclonal hypergammaglobulinaemia — a broad diffuse rise in the gamma region, not a narrow spike. Elevated ESR, anaemia, and raised total protein can all occur in reactive states. Immunofixation then characterises the heavy and light chain class of the M-protein, which is diagnostic.
Diagnostic Criteria (Brief)
Diagnostic Criteria for Multiple Myeloma
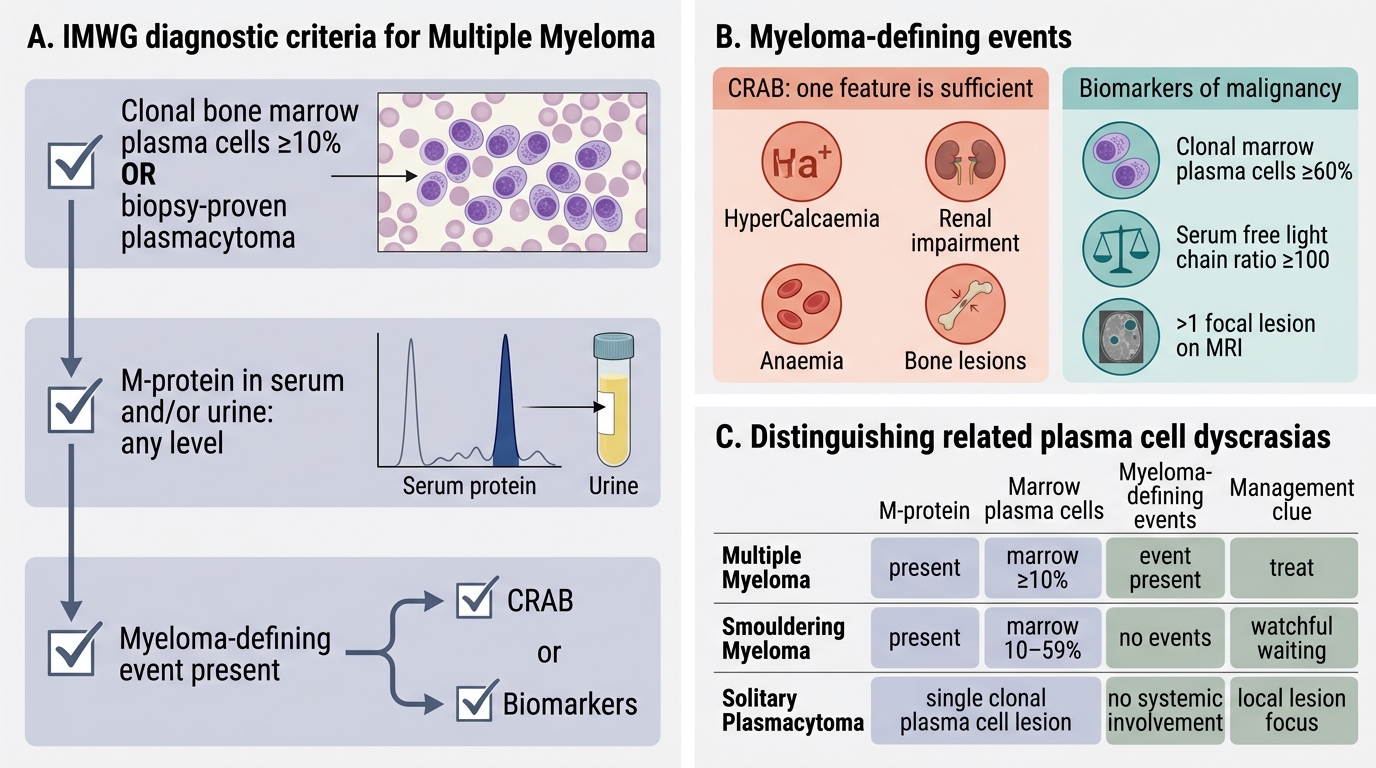
The IMWG (International Myeloma Working Group) criteria require ALL THREE:
1. Clonal bone marrow plasma cells ≥10% (or biopsy-proven plasmacytoma)
2. M-protein in serum and/or urine (any level)
3. Myeloma-defining events — either CRAB criteria (end-organ damage) OR biomarkers of malignancy:
• Clonal marrow plasma cells ≥60%
• Serum free light chain ratio ≥100
• >1 focal lesion on MRI
> Note: You do NOT need all four CRAB features — one is sufficient if the plasma cell and M-protein criteria are met.
Smouldering myeloma: M-protein present + marrow plasma cells 10–59% but NO myeloma-defining events — watchful waiting, no treatment.
Solitary plasmacytoma: single bony or extramedullary lesion of clonal plasma cells without systemic involvement.
Differential Diagnosis

Differential Diagnosis of Plasma Cell Dyscrasias
Three key entities to distinguish:
MGUS (Monoclonal Gammopathy of Undetermined Significance)
• M-protein present (usually <30 g/L) AND marrow plasma cells <10%
• No CRAB features, no end-organ damage
• Incidental finding; ~1% annual risk of progression to myeloma
• The most important DDx — do NOT treat MGUS as myeloma
Waldenström Macroglobulinaemia
• Clonal lymphoplasmacytic lymphoma secreting IgM monoclonal protein
• IgM is a large pentameric molecule → hyperviscosity syndrome is the dominant feature (vs. myeloma where bone disease dominates)
• Lytic bone lesions and CRAB features are characteristically ABSENT
• Marrow shows lymphoplasmacytic infiltrate, not sheets of plasma cells
• CXCR4/MYD88 mutations are characteristic
Reactive Plasmacytosis
• Seen in chronic infections (TB, endocarditis), autoimmune diseases, liver cirrhosis
• Plasma cells usually <10% of marrow
• Polyclonal hypergammaglobulinaemia (broad gamma rise on SPEP, NOT a sharp M-spike)
• No Bence-Jones protein, no CRAB features
| Feature | MGUS | Myeloma | Waldenström |
|---|---|---|---|
| M-protein | <30 g/L | Any level | IgM |
| Marrow PC | <10% | ≥10% | Lymphoplasmacytic |
| CRAB | Absent | Present (≥1) | Absent |
| Bone lesions | None | Lytic | None |
| Hyperviscosity | Rare | Occasional | Common |
SELF-CHECK
A 70-year-old woman is found to have an IgG M-spike of 18 g/L on SPEP during routine check-up. Bone marrow biopsy shows 7% plasma cells. She has no anaemia, normal calcium, normal creatinine, and no bone lesions on skeletal survey. The correct diagnosis and management is:
A. Multiple myeloma — start chemotherapy
B. MGUS — observe with annual monitoring
C. Smouldering myeloma — start lenalidomide
D. Waldenström macroglobulinaemia — check for hyperviscosity
Reveal Answer
Answer: B. MGUS — observe with annual monitoring
This patient fulfils the criteria for MGUS: M-protein present BUT marrow plasma cells <10% (7%) AND no CRAB features (no anaemia, no hypercalcaemia, no renal failure, no bone lesions). MGUS requires no treatment — only annual monitoring for progression to myeloma (~1% per year). Smouldering myeloma requires ≥10% plasma cells (this patient has 7%). Waldenström involves IgM paraprotein and a lymphoplasmacytic (not plasma cell) infiltrate.
Prognosis and a Note on Staging
Prognosis and ISS Staging in Multiple Myeloma
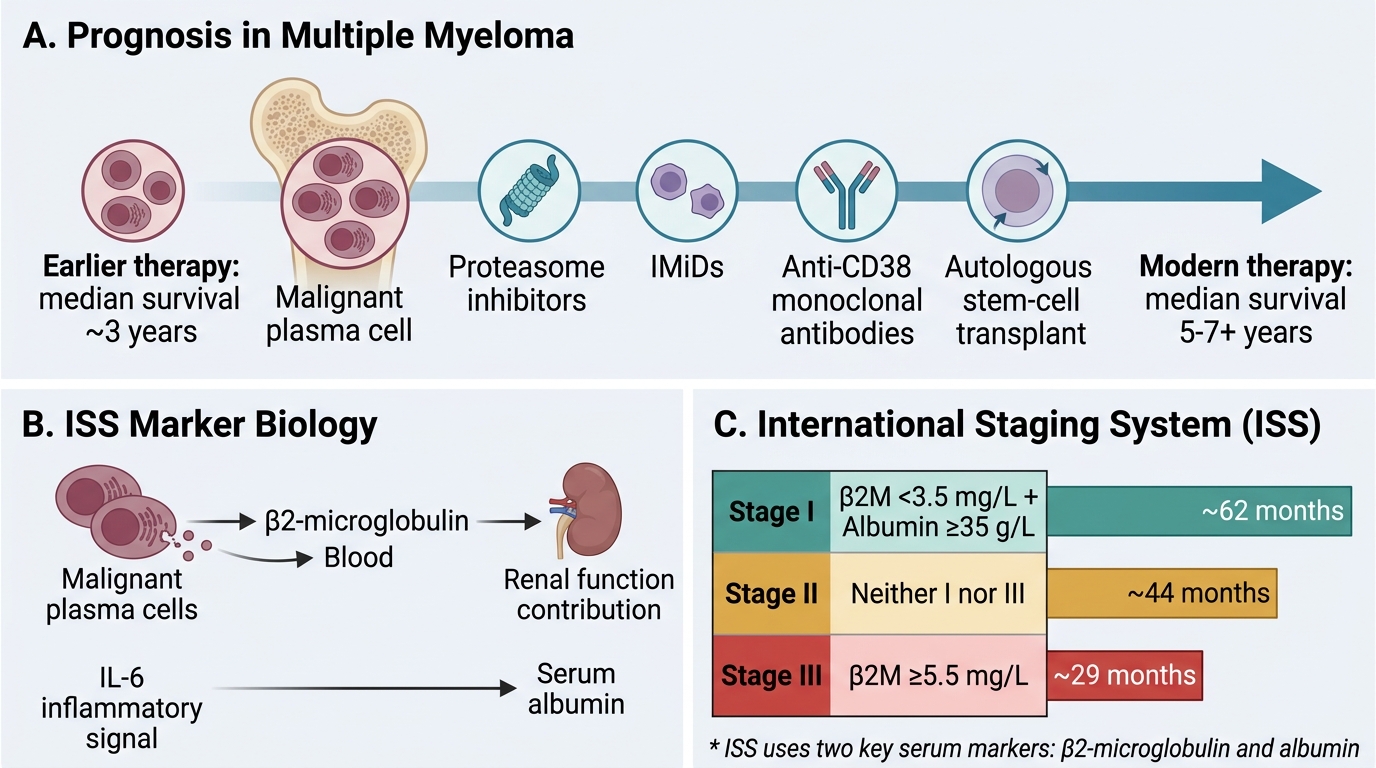
Myeloma is currently incurable in most patients but is treatable; median survival has improved from 3 years to 5–7+ years with modern therapy (proteasome inhibitors, IMiDs, anti-CD38 monoclonal antibodies, autologous stem-cell transplant).
International Staging System (ISS) — the two key markers:
• β2-microglobulin — shed by plasma cells; reflects tumour burden + renal function
• Serum albumin — inverse correlate of IL-6 activity
| ISS Stage | β2M | Albumin | Median Survival |
|---|---|---|---|
| I | <3.5 mg/L | ≥35 g/L | ~62 months |
| II | Neither I nor III | — | ~44 months |
| III | ≥5.5 mg/L | — | ~29 months |
High-risk cytogenetics (del 17p, t(4;14), t(14;16)) further stratify prognosis in the Revised ISS (R-ISS).