Page 3 of 27
PA21.1 | ABO & Rh Blood Group Systems — SDL Guide (Part 3)
Haemolytic Disease of the Newborn (HDN)
Rh Haemolytic Disease of the Newborn
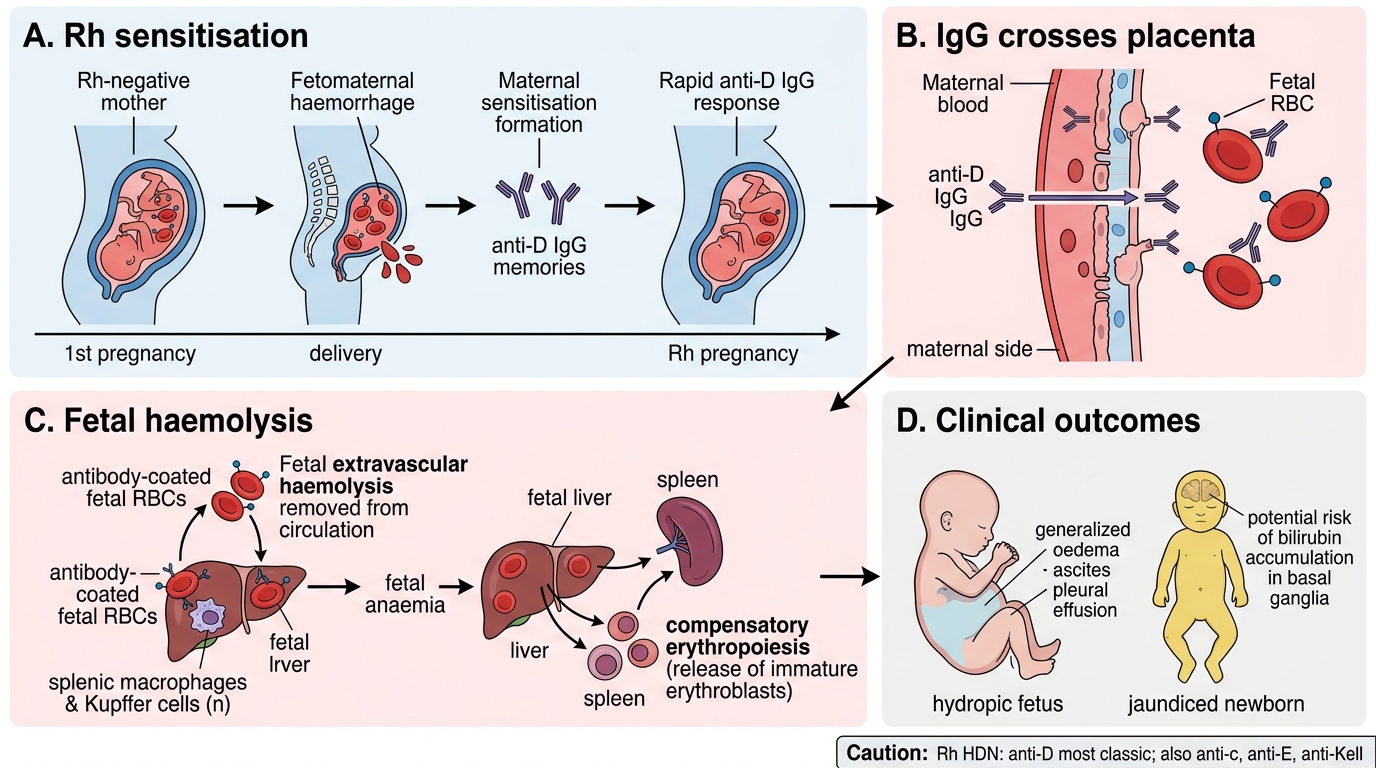
HDN (also called erythroblastosis fetalis) is the paradigm disease illustrating the clinical consequences of Rh incompatibility.
Classic scenario:
• Rh-negative (Rh−) mother × Rh-positive (Rh+) father → Rh+ fetus (inherits D antigen from father)
• During delivery (or earlier — amniocentesis, antepartum haemorrhage), fetal RBCs enter maternal circulation: fetomaternal haemorrhage
• Maternal immune system recognises D antigen as foreign → produces anti-D (IgG) — sensitisation
• First pregnancy is usually safe (sensitisation occurs late in gestation; anti-D titre is low and rises slowly)
• In a subsequent Rh+ pregnancy, maternal anti-D memory B cells respond rapidly → high-titre IgG anti-D
• IgG crosses the placenta → binds fetal RBCs → extravascular haemolysis (Kupffer cells and splenic macrophages) → fetal anaemia
• Fetal liver/spleen produce immature RBCs (erythroblasts) to compensate → erythroblastosis fetalis
• Severe cases: massive haemolysis, high-output cardiac failure, generalised oedema, ascites, pleural effusions → hydrops fetalis (the fatal end-stage)
• After delivery: ongoing haemolysis + neonatal liver immaturity → neonatal jaundice, hyperbilirubinaemia, risk of kernicterus (bilirubin deposits in basal ganglia)
IMPORTANT: Rh HDN can also be caused by anti-c, anti-E, and anti-Kell antibodies — not just anti-D.

Hemolytic Disease of the Newborn: Two-Pregnancy Mechanism
CLINICAL PEARL
Anti-D prophylaxis (Rho(D) immune globulin / RhoGAM): Given to all Rh-negative pregnant women at 28 weeks and within 72 hours of delivery of an Rh+ baby. The injected anti-D rapidly clears any fetal D+ RBCs from the maternal circulation before the maternal immune system can mount its own response — preventing sensitisation. Key teaching point: this is passive immunisation that prevents active immune sensitisation. It does NOT help once sensitisation has already occurred. It must be given after every potentially sensitising event (miscarriage, ectopic pregnancy, amniocentesis, antepartum haemorrhage).
SELF-CHECK
A primigravida Rh-negative woman delivers a healthy Rh-positive baby. Anti-D prophylaxis is NOT given. In her second pregnancy with an Rh-positive fetus, what is the expected immunological finding and consequence?
A. High-titre IgM anti-D in maternal plasma; immediate intravascular haemolysis of fetal RBCs
B. High-titre IgG anti-D in maternal plasma; crosses placenta, causes extravascular haemolysis of fetal RBCs
C. No anti-D (natural antibodies are absent in Rh-negative individuals); no fetal harm
D. Low-titre IgA anti-D in maternal plasma; binds fetal RBCs but does not activate complement
Reveal Answer
Answer: B. High-titre IgG anti-D in maternal plasma; crosses placenta, causes extravascular haemolysis of fetal RBCs
After sensitisation in the first pregnancy, memory B cells produce high-titre IgG anti-D on re-exposure in the second pregnancy. IgG (unlike IgM) readily crosses the placenta, binds fetal Rh+ RBCs, and causes extravascular haemolysis via macrophages in fetal spleen and liver — the mechanism of HDN. IgM does NOT cross the placenta. Natural anti-D does not exist. IgA plays no role here.
Other Clinically Important Blood Group Systems

Clinically Important Blood Group Systems Beyond ABO and Rh
Beyond ABO and Rh, several other systems cause clinically significant alloimmunisation:
| System | Key antigen | Antibody class | Clinical significance |
|---|---|---|---|
| Kell | K (Kell) | IgG | Highly immunogenic; second only to D. Causes severe HDN. Anti-K suppresses fetal erythropoiesis directly. |
| Duffy | Fy(a), Fy(b) | IgG | Duffy-null (Fy(a−)Fy(b−)) common in West Africans; Duffy antigen is the receptor for Plasmodium vivax — Duffy-null individuals are resistant to P. vivax malaria |
| Kidd | Jk(a), Jk(b) | IgG | Anti-Jk(a) notorious for delayed haemolytic transfusion reactions (antibody titre falls below detectable levels between transfusions, then rises rapidly on re-exposure) |
These systems are tested in pre-transfusion compatibility (crossmatch) and must be considered in patients who are chronically transfused (e.g., sickle cell disease, thalassaemia).
Agglutination: The Unifying Principle of Blood Grouping

Agglutination in ABO Blood Grouping
All blood group typing relies on agglutination — the clumping of RBCs when antibody bridges antigens on adjacent cells.
Mechanism:
1. Antibody (typically IgM for direct agglutination — its pentameric structure spans the ~25 nm gap between RBCs easily) binds antigen on the RBC surface.
2. Each antibody molecule cross-links two RBCs.
3. Aggregates form a visible clump (positive reaction).
4. Absence of antigen → no binding → RBCs remain dispersed (negative reaction).
In the direct agglutination test (tube or tile method):
• Add anti-A serum to test RBCs → agglutination = A antigen present
• Add anti-B serum → agglutination = B antigen present
• Confirm with reverse grouping: test plasma against known A and B cells
IgG antibodies (Rh, Kell, Kidd, Duffy) do NOT cause direct agglutination because of their smaller size and the repulsion between RBCs (zeta potential). They require the indirect antiglobulin test (Coombs test) — covered in SDL 5.

ABO Blood Group Agglutination Reaction Schematic
SELF-CHECK
Why does ABO incompatibility typically cause immediate intravascular haemolysis, while Rh incompatibility (anti-D) causes delayed extravascular haemolysis?
A. ABO antibodies are IgG and activate complement to completion; anti-D is IgM and cannot cross the placenta
B. ABO antibodies are IgM and efficiently activate complement to MAC formation; anti-D is IgG, activates complement only partially, and causes macrophage-mediated extravascular destruction
C. ABO incompatibility involves more antigens on the RBC surface; Rh incompatibility involves fewer antigens so the reaction is slower
D. ABO antibodies are naturally occurring and always present in high titres; anti-D is always present in low titres because it is a natural antibody
Reveal Answer
Answer: B. ABO antibodies are IgM and efficiently activate complement to MAC formation; anti-D is IgG, activates complement only partially, and causes macrophage-mediated extravascular destruction
ABO natural isohaemagglutinins are IgM — pentameric, highly efficient at activating the classical complement pathway to completion (MAC formation) → intravascular haemolysis within minutes. Anti-D is IgG — does not activate complement to completion, coats RBCs with IgG, which are then recognised and destroyed extravascularly by splenic and hepatic macrophages (Fc receptor-mediated). The IgM/IgG distinction drives the entire clinical difference.