Page 3 of 15
PA13.2 | Approach to Anemia: Classification & Diagnostic Workup — SDL Guide (Part 3)
The 5-Step Diagnostic Workup Algorithm
This is the framework you will use every time anemia is confirmed on a CBC. Learn it as a sequence, not a checklist.
STEP 1 — Confirm anemia and grade severity
- Hb below WHO threshold? → Yes = anemia confirmed
- Grade: mild (Hb 10–12), moderate (8–10), severe (< 8), life-threatening (< 6.5 g/dL)
- Urgency: severe/life-threatening → stabilize first, investigate simultaneously
STEP 2 — MCV → Morphological class
- < 80 fL → microcytic (→ iron studies, Hb electrophoresis)
- 80–100 fL → normocytic (→ retic count, LFT, RFT, TSH, direct Coombs)
- > 100 fL → macrocytic (→ B12, folate, LFT, TSH, reticulocyte count)
- Check RDW: elevated RDW with any MCV → suspect mixed deficiency or early deficiency
STEP 3 — Reticulocyte count → Marrow response
- Calculate RPI
- RPI < 2 → hypoproliferative → step into production-failure workup
- RPI > 2 → hyperproliferative → step into hemolysis/blood loss workup
STEP 4 — Peripheral blood smear
- Mandatory in ALL cases of anemia — never skip this
- What to look for: cell size (confirms MCV), shape (target cells, spherocytes, elliptocytes, schistocytes, sickle cells), WBC morphology (hypersegmented neutrophils → megaloblastic; blasts → leukemia), platelet count (thrombocytopenia + anemia → aplastic, TTP, megaloblastic)
- Smear findings that change management immediately: schistocytes (microangiopathic → TTP/HUS emergency), blasts (leukemia → hematology referral), sickle cells (SCD → crisis management)
STEP 5 — Targeted investigations based on Steps 2–4
| Suspected diagnosis | Key investigations |
|---|---|
| IDA | Serum ferritin (most sensitive), serum iron + TIBC (saturation < 16%), FEP, Hb electrophoresis to exclude thalassemia trait |
| B12 deficiency | Serum B12, MMA, homocysteine; intrinsic factor antibodies if autoimmune gastritis suspected |
| Folate deficiency | Serum folate (or RBC folate for tissue stores), homocysteine |
| Hemolytic anemia | Direct Coombs test (AIHA), LDH (elevated), indirect bilirubin (elevated), haptoglobin (decreased), peripheral smear (spherocytes/schistocytes/sickle cells), G6PD assay, Hb electrophoresis |
| Aplastic anemia | Bone marrow biopsy (hypocellular marrow), cytogenetics |
| Anemia of CKD | Serum creatinine, eGFR, EPO level (low) |
| Anemia of chronic disease | ESR, CRP, ferritin (elevated), iron studies (low serum iron, normal/low TIBC) |
Indian clinical context additions:
- Stool for ova and parasites (hookworm) — especially in rural, barefoot-walking adults with IDA
- Malaria RDT or smear — in febrile hemolytic anemia in endemic zones
- G6PD assay — before prescribing antimalarials (primaquine) or nitrofurantoin
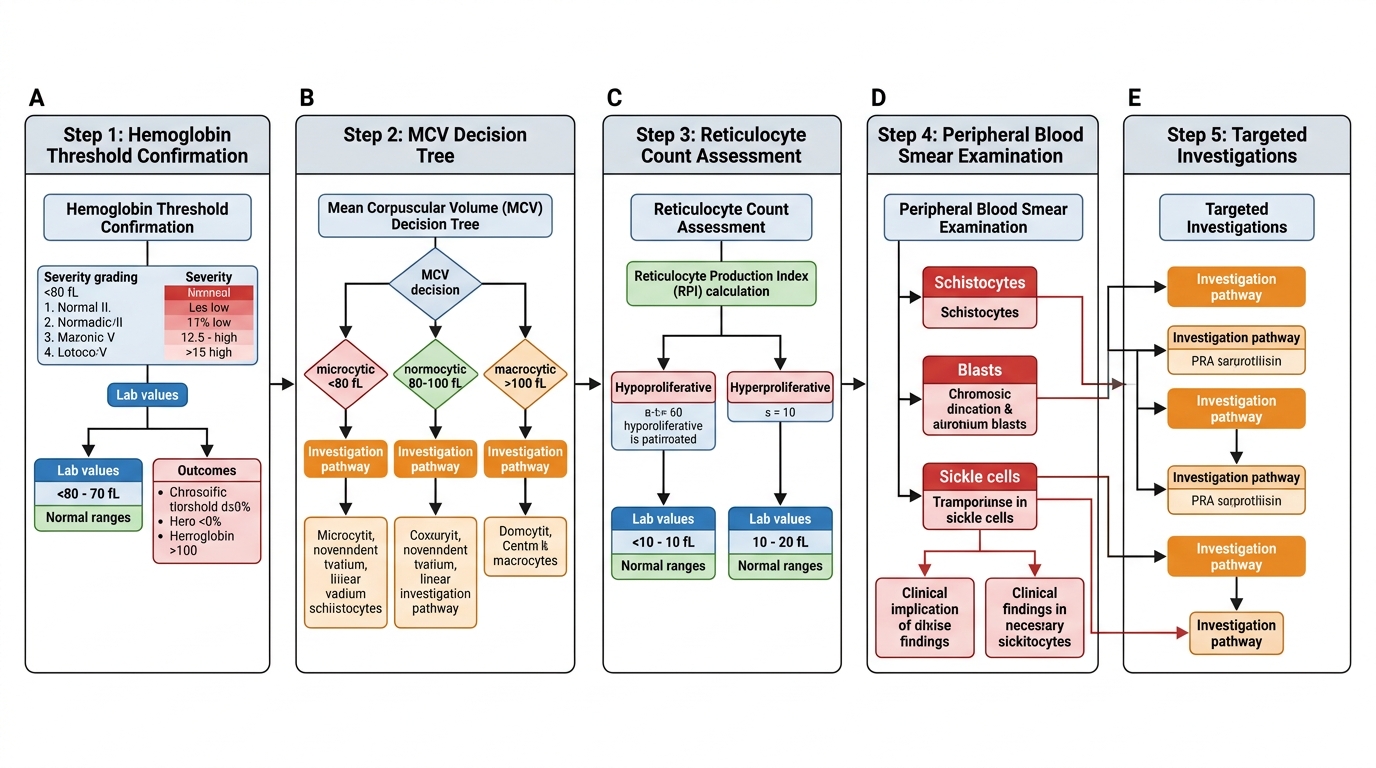
The 5-Step Diagnostic Workup Algorithm for Anemia
SELF-CHECK
A 55-year-old woman presents with 3 months of fatigue and pallor. Investigations: Hb 7.2 g/dL, MCV 68 fL, RDW 18% (elevated), reticulocyte count 0.4%, serum ferritin 6 µg/L (low), TIBC elevated, peripheral smear: hypochromic microcytic cells with pencil cells. What is the MOST LIKELY diagnosis AND the next MOST important investigation to determine the cause?
A. A. Thalassemia trait — Hb electrophoresis
B. B. Iron deficiency anemia — stool examination for occult blood and helminths
C. C. Anemia of chronic disease — CRP and ESR
D. D. Sideroblastic anemia — bone marrow biopsy with Prussian blue stain
Reveal Answer
Answer: B. B. Iron deficiency anemia — stool examination for occult blood and helminths
The low MCV (68 fL), elevated RDW, low ferritin, elevated TIBC, and hypochromic microcytic smear with pencil cells are diagnostic of iron deficiency anemia (IDA). In a 55-year-old woman who is post-menopausal (no menstrual loss), IDA must be explained by pathological blood loss until proven otherwise. The most important next step is stool examination for occult blood (GI malignancy, peptic ulcer, hookworm) — GI workup (colonoscopy) is mandatory. Thalassemia trait has normal or low-normal ferritin, normal RDW, and would show a higher RBC count relative to the Hb ('decoupling'). Anemia of chronic disease has normal-to-elevated ferritin and low TIBC. Sideroblastic anemia has elevated ferritin and ring sideroblasts on bone marrow.
Worked Example: Applying the 5-Step Framework
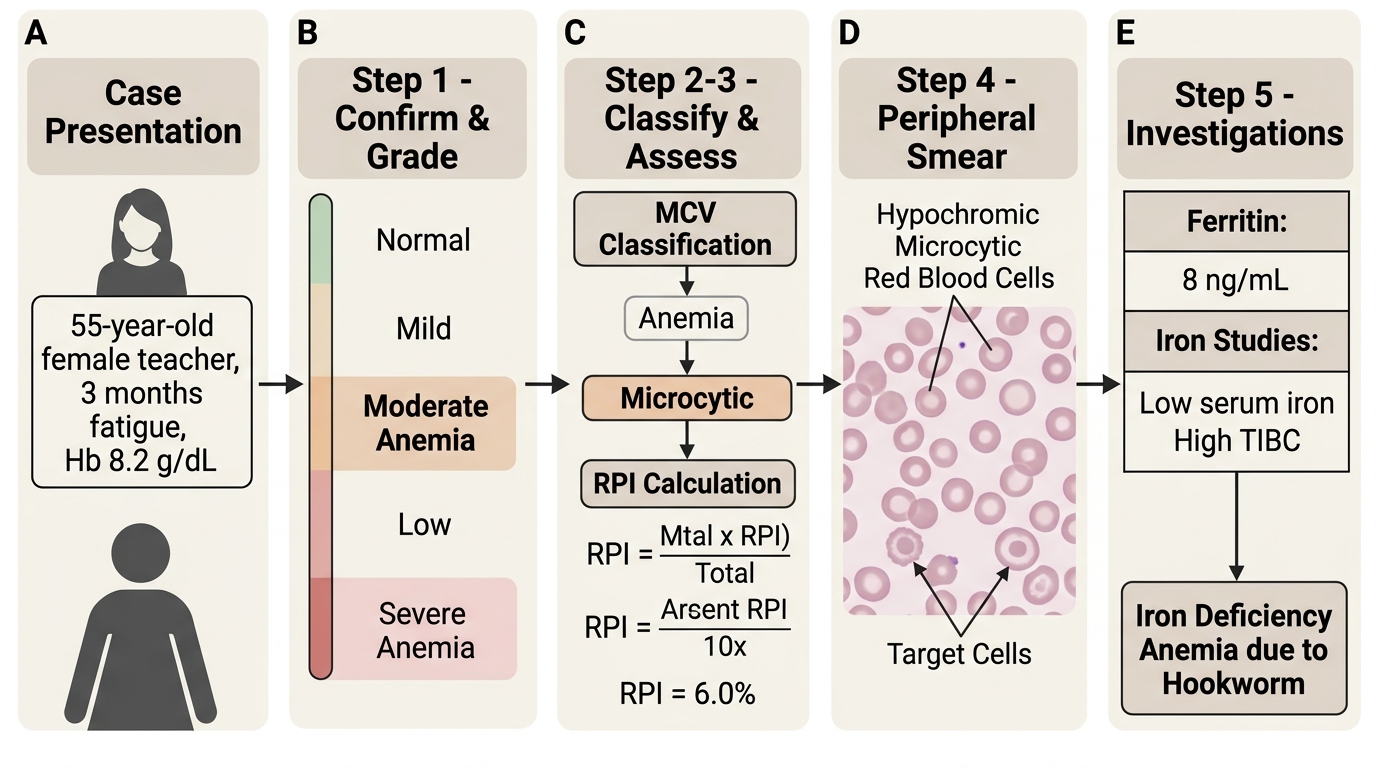
5-Step Anemia Framework: Iron Deficiency Anemia Case Example
Case: 55-year-old female teacher (de-identified), 3 months of fatigue, Hb 8.2 g/dL, MCV 70 fL, reticulocyte count 0.5%, peripheral smear: hypochromic microcytic cells, occasional target cells, no spherocytes, no blasts.
Step 1 — Confirm and grade: Hb 8.2 g/dL is below 12.0 g/dL (non-pregnant adult woman). Severity: moderate (8.0–10.9 g/dL). Not immediately life-threatening, but warrants prompt workup.
Step 2 — MCV 70 fL: Microcytic. Differential: IDA, thalassemia, ACD (unlikely if truly microcytic), sideroblastic anemia. High RDW noted (not given here but typically elevated in IDA).
Step 3 — Reticulocyte 0.5%: Calculate RPI. Hct ≈ 25% → maturation factor 2.0. Normal Hb for women = 13 g/dL. CRC = 0.5 × (8.2/13) = 0.32%. RPI = 0.32/2.0 = 0.16. RPI << 2 → hypoproliferative. The marrow is NOT compensating. This is a production problem, NOT hemolysis.
Step 4 — Peripheral smear: Hypochromic microcytic cells + target cells. No spherocytes (rules against autoimmune hemolysis). No blasts. Target cells suggest either IDA or thalassemia.
Step 5 — Targeted investigations:
- Serum ferritin: 5 µg/L (severely depleted — confirms IDA)
- Serum iron: 30 µg/dL (low); TIBC: 450 µg/dL (elevated); Saturation: 6.7% (< 16%, confirms IDA)
- Hb electrophoresis: HbA2 3.2% (normal, ≤ 3.5%) → rules out beta-thalassemia trait
- Stool for occult blood and ova/parasites: Ancylostoma eggs ++ (hookworm!)
Conclusion: Iron deficiency anemia, moderate severity, secondary to hookworm infestation. Management: single-dose albendazole 400 mg for hookworm + oral ferrous sulfate 200 mg TID for 3 months + dietary counseling. Recheck Hb at 4 weeks; if suboptimal response, investigate for celiac disease or H. pylori.
Teaching point: In this 55-year-old woman (post-menopausal, no GI symptoms), it would be tempting to stop at 'IDA + hookworm' and not investigate further. However, any new IDA in a post-menopausal woman or adult male requires exclusion of GI malignancy — colonoscopy is indicated even after hookworm is found, because two causes can coexist.