Page 1 of 17
PA15.1 | Vitamin B12 & Folate Metabolism — Deficiency Pathogenesis — SDL Guide
Learning Objectives
- Trace the dietary sources and absorption pathway of Vitamin B12, including the role of intrinsic factor and the terminal ileum.
- Outline folate absorption and metabolism, and explain the biochemical relationship between B12 and folate.
- Describe the major causes of B12 deficiency (pernicious anaemia, dietary, malabsorption, drugs) and their mechanisms.
- Explain how impaired DNA synthesis leads to megaloblastosis and nuclear-cytoplasmic asynchrony.
- Justify why neurological involvement (subacute combined degeneration) occurs in B12 deficiency but NOT in isolated folate deficiency.
- Contrast the clinical and biochemical differences between B12 and folate deficiency anemias.
INSTRUCTIONS
Macrocytic anaemia is one of the most nuanced haematological diagnoses in MBBS — because the same blood film can arise from two metabolically distinct deficiencies. This module unpacks the biochemistry and pathology of B12 and folate metabolism so you understand why deficiency causes megaloblastosis and why only B12 deficiency harms the spinal cord. Before you reach the lab module (H4 SDL2) or the smear module (H4 SDL3), you need the molecular foundation built here.
References
- Robbins & Kumar Basic Pathology, 10th ed., Ch 14 — Red Cell Disorders (textbook)
- Harsh Mohan Textbook of Pathology, 7th ed., Ch 12 — Nutritional & Megaloblastic Anaemias (textbook)
- Devlin Biochemistry with Clinical Correlations, 8th ed., Ch 25 — B Vitamins (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old strict vegetarian arrives with a 3-year history of progressive fatigue and mild unsteadiness of gait. Her tongue is smooth and sore. CBC shows macrocytic anaemia; her serum B12 is undetectable. Her gastroenterologist finds no Crohn's disease, no ileal resection. Yet her serum anti-intrinsic-factor antibodies return positive.
The same blood-film appearance could have been caused by a folate deficiency — but the neurological wobble would not. By the time you finish this module you will know exactly why, and you will be able to explain it to a patient in a single, clear sentence.
RECALL
Before we begin, activate what you already know from Year-1:
- DNA synthesis requires thymidine; thymidine synthesis requires the one-carbon transfer enzyme thymidylate synthase, which in turn requires a folate derivative (5,10-methylene-THF).
- Myelin is maintained by remethylation of homocysteine → methionine → SAM (S-adenosylmethionine) as the methyl donor; B12 is the cofactor for this reaction.
- Gastric parietal cells secrete both hydrochloric acid and intrinsic factor (IF). Recall the proton-pump physiology from GI block.
If these feel rusty, spend 5 minutes re-reading your Year-1 biochemistry notes on one-carbon metabolism before proceeding — the clinical story below builds directly on them.
Vitamin B12 — Sources and Absorption Pathway
Vitamin B12 Absorption Pathway: Five-Step Relay Process
Vitamin B12 (cobalamin) is synthesised exclusively by micro-organisms; all dietary B12 enters the human body through animal-derived foods — meat, fish, eggs, dairy. Strict vegans consuming no animal products have zero dietary intake.
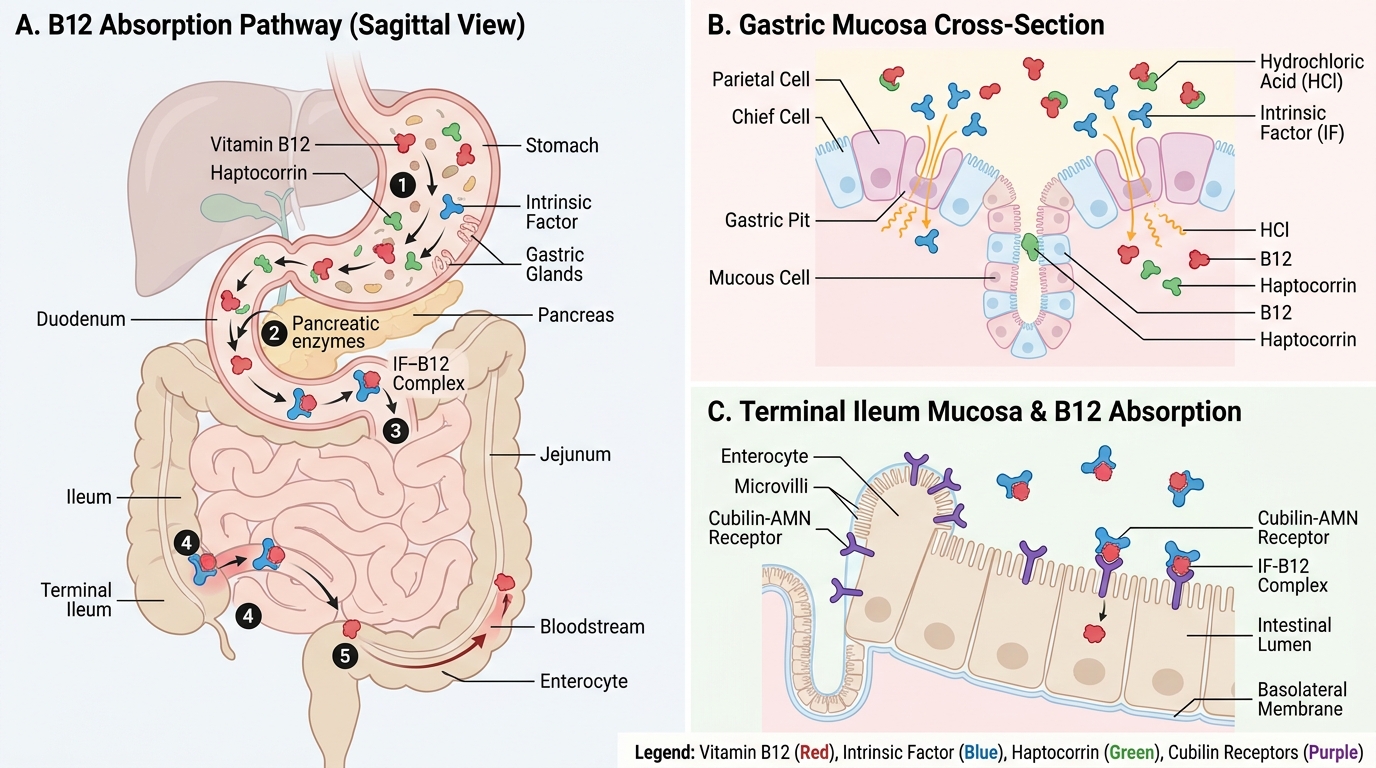
Absorption — a five-step relay:
- Gastric acid releases protein-bound B12 from food.
- Free B12 binds haptocorrin (R-protein), secreted by salivary glands and gastric mucosa, which protects it through the acid stomach.
- Pancreatic proteases degrade haptocorrin in the duodenum, releasing B12.
- Free B12 binds intrinsic factor (IF), a 44 kDa glycoprotein secreted by gastric parietal cells of the fundus/body. IF-B12 complex is resistant to digestion.
- The IF-B12 complex binds the cubilin-AMN receptor complex in the terminal ileum mucosa, is endocytosed, and enters portal blood bound to transcobalamin II (TC-II).
TC-II delivers B12 to every tissue. Hepatic stores (3–5 mg) are enough for 3–5 years — this explains the long latency of clinical deficiency after dietary omission begins.
IMPORTAN: daily requirement is only 1–2 µg; the body recycles B12 via enterohepatic circulation (bile → re-absorption in ileum), which further extends stores.
IMPORTAN: Only the terminal ~100 cm of ileum carries cubilin receptors — proximal ileal disease or resection leaves B12 unabsorbed even if IF is normal.

Vitamin B12 Absorption Pathway: From Ingestion to Portal Circulation
Folate — Sources, Absorption, and Cellular Delivery
Folate Sources, Absorption, and Cellular Delivery
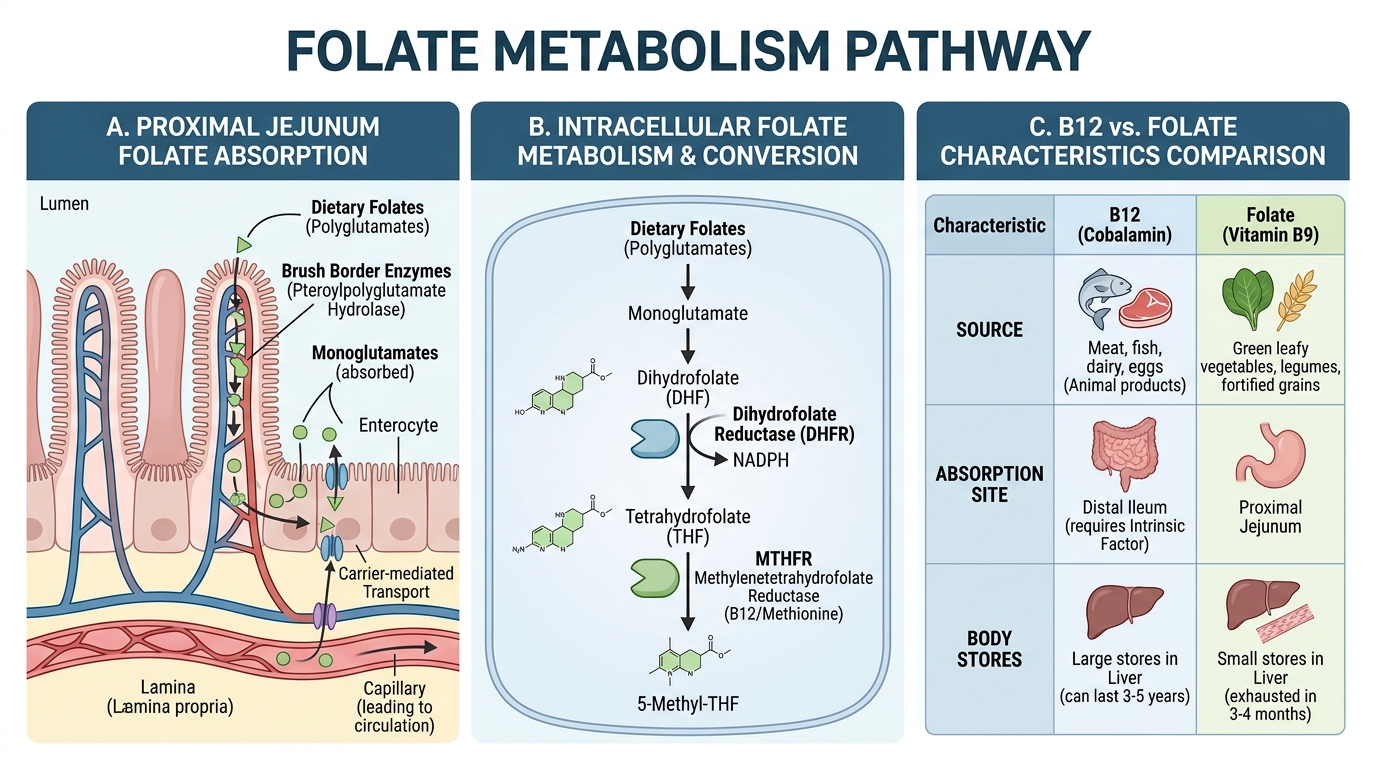
Folate (vitamin B9) is abundant in green leafy vegetables, legumes, liver, and fortified cereals. Unlike B12, body stores are modest — only 3–4 mg, sufficient for about 3–4 months. Deficiency develops far faster than B12 deficiency after dietary omission.
Absorption:
• Dietary folate arrives as polyglutamates; intestinal brush-border γ-glutamyl carboxypeptidase (folate conjugase) cleaves excess glutamate residues.
• Monoglutamate folate is absorbed throughout the proximal jejunum (contrast: B12 is terminal ileum only).
• Inside intestinal cells it is reduced to dihydrofolate (DHF), then to tetrahydrofolate (THF) by dihydrofolate reductase (DHFR).
• THF is methylated to 5-methyl-THF, the predominant plasma form, and delivered to tissues.
Storage: folate is polyglutamated inside cells (keeps it trapped intracellularly) and stored predominantly in the liver.
| Feature | Vitamin B12 | Folate |
|---|---|---|
| Source | Animal foods only | Plant + animal |
| Absorption site | Terminal ileum | Proximal jejunum |
| Body stores | 3–5 mg (3–5 years) | 3–4 mg (3–4 months) |
| Carrier protein | Transcobalamin II | Reduced folate carrier |
| Latency to deficiency | Years | Months |
SELF-CHECK
A 45-year-old patient undergoes surgical resection of the terminal 80 cm of ileum for Crohn's disease. Which nutrient will become most difficult to absorb over the following years?
A. Folate
B. Vitamin B12
C. Iron
D. Vitamin D
Reveal Answer
Answer: B. Vitamin B12
The terminal ileum is the exclusive site for cubilin-receptor–mediated absorption of the intrinsic factor–B12 complex. Folate is absorbed in the proximal jejunum (unaffected). Iron and vitamin D have multiple absorption sites unrelated to the terminal ileum. After ileal resection, B12 malabsorption is inevitable regardless of how much IF the stomach produces.
Cellular Roles of B12 — the Two Key Enzymes
Cellular Roles of Vitamin B12: The Two Key Enzymes
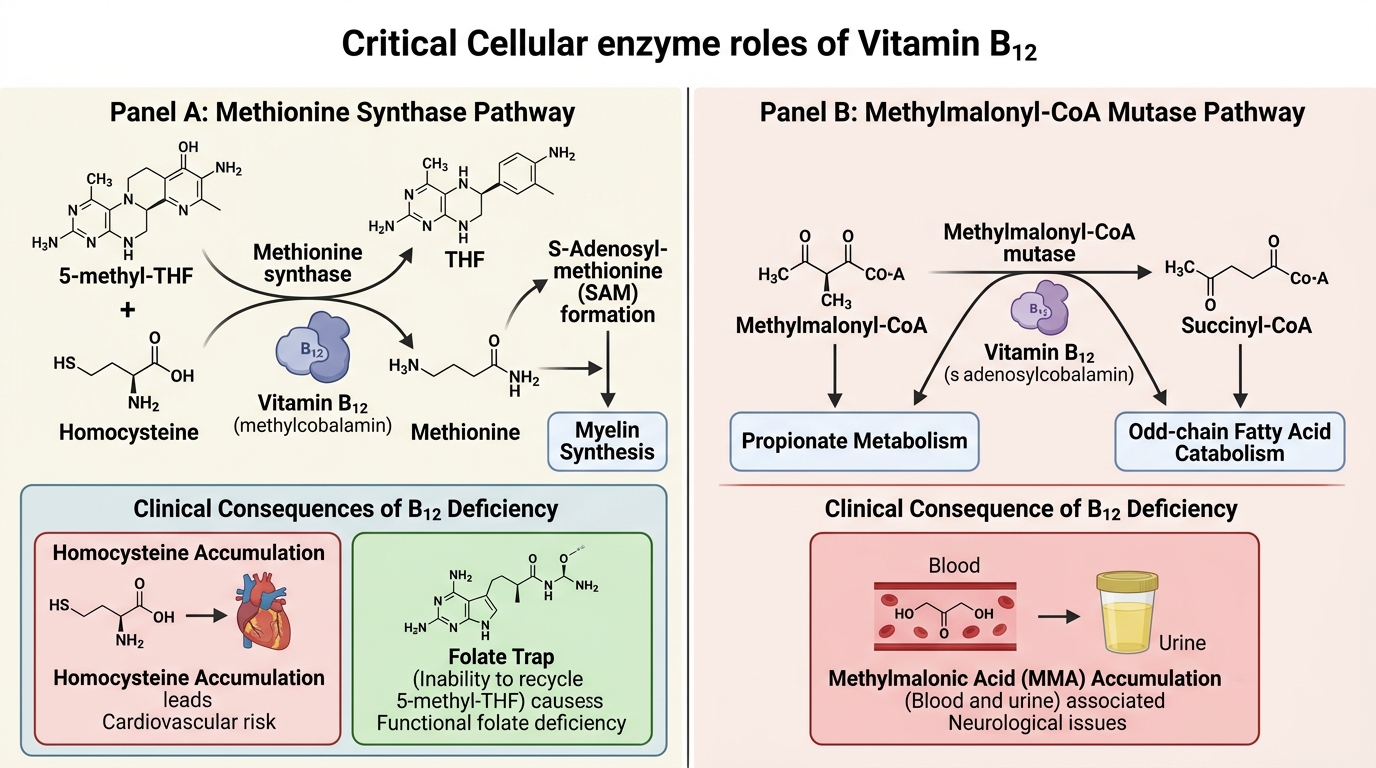
Inside cells, B12 (as methylcobalamin and adenosylcobalamin) is the cofactor for exactly two enzymes in humans — and both are clinically important:
1. Methionine synthase (MS)
• Reaction: 5-methyl-THF + homocysteine → THF + methionine (B12 as methylcobalamin is the methyl carrier)
• Why it matters: methionine → S-adenosylmethionine (SAM), the universal methyl donor for myelin synthesis and hundreds of other methylation reactions.
• Deficiency consequence A — homocysteine accumulates (toxic to endothelium, causes thrombosis).
• Deficiency consequence B — the folate trap (see below).
2. Methylmalonyl-CoA mutase (MUT)
• Reaction: methylmalonyl-CoA → succinyl-CoA (B12 as adenosylcobalamin)
• Why it matters: propionate metabolism and fatty-acid catabolism.
• Deficiency consequence — methylmalonic acid (MMA) accumulates. Elevated serum MMA is a specific marker of B12 deficiency (unlike homocysteine, which rises in both B12 and folate deficiency).
Remember: only methylmalonyl-CoA mutase requires B12. Folate deficiency does NOT raise MMA — this biochemical fact underpins the diagnostic separation.