Page 2 of 23
PA19.1 | Approach to Lymphadenopathy — SDL Guide (Part 2)
Differentiating Features: Clinical Discriminators

Clinical Discriminators in Lymphadenopathy
When you palpate a lymph node, six clinical features create the differential framework:
1. Distribution: Localised vs Generalised
• Localised (one region) → suggests a regional cause: local infection (dental, scalp, tonsil), or metastatic disease draining from a known primary.
• Generalised (≥ 2 non-contiguous regions) → suggests systemic disease: viral infection (EBV, CMV, HIV), autoimmune (SLE, RA), disseminated malignancy (leukaemia, advanced NHL), drug reaction, or sarcoidosis.
2. Tenderness
• Tender → inflammatory/infective (rapid capsular stretch from oedema). Pyogenic lymphadenitis, early viral infections.
• Non-tender → neoplastic (slow growth, no inflammation) or granulomatous (TB, sarcoid — fibrosis suppresses pain). Painless lymphadenopathy in a young adult = lymphoma until proven otherwise.
3. Consistency
• Soft — acute inflammation, abscess formation.
• Firm — reactive hyperplasia, early lymphoma.
• Rubbery — classic for lymphoma (HL particularly). The word to remember: rubber-ball feel.
• Hard/stony — metastatic carcinoma. Desmoplastic stroma from the tumour makes the node rock-hard.
4. Mobility and Matting
• Mobile — reactive nodes (capsule intact, no extra-nodal spread).
• Fixed/matted (nodes fused together) — neoplastic infiltration (lymphoma, metastasis) or TB (periadenitis from caseation and fibrosis).
5. Site Significance
• Virchow's node (left supraclavicular) — via the thoracic duct; metastasis from GI (gastric, colon, pancreatic), lung, or pelvic primaries. Troisier's sign = palpable Virchow's node.
• Right supraclavicular — lung, oesophagus, mediastinal primaries.
• Epitrochlear — normally impalpable; when enlarged → sarcoidosis, syphilis (secondary), cat-scratch disease, lymphoma.
• Posterior cervical — EBV, toxoplasmosis, TB (posterior triangle).
• Anterior cervical — dental, tonsillar, thyroid pathology.
6. Age as Discriminator
• < 14 years: reactive/infective cause is overwhelmingly more likely (> 90%).
• 15–35 years: infectious mononucleosis + lymphoma both on the list; Hodgkin lymphoma peaks here.
• > 50 years: malignancy (NHL, metastasis, CLL) probability rises sharply.

Lymph Node Groups and Drainage Territories: Clinical Anatomy
SELF-CHECK
A 58-year-old woman has a 2 cm, non-tender, hard, fixed left supraclavicular lymph node. She reports a 4 kg weight loss over 3 months. What is the SINGLE most important step in the diagnostic workup?
A. FNAC of the lymph node
B. Excision biopsy of the lymph node
C. Search for a primary tumour (CECT chest, abdomen, pelvis)
D. Empirical anti-tuberculosis therapy
Reveal Answer
Answer: C. Search for a primary tumour (CECT chest, abdomen, pelvis)
Hard, fixed, left supraclavicular (Virchow's node) with constitutional symptoms in a 58-year-old is metastatic carcinoma until proven otherwise. The immediate priority is finding the primary — CECT chest/abdomen/pelvis will identify the source (gastric, colonic, pancreatic, lung, or pelvic origin). FNAC (option A) can confirm the node is malignant and the cell type, but is done after imaging to guide it; excision biopsy (option B) is inappropriate for suspected metastatic carcinoma (architecture is irrelevant here, unlike lymphoma). Option D is dangerous — starting ATT without histological proof in a patient with high metastasis risk delays cancer treatment.
Diagnostic Approach: FNAC vs Excision Biopsy

FNAC vs Excision Biopsy in Lymphadenopathy
Once clinical assessment raises concern, tissue diagnosis is required. Two options exist:
Fine-Needle Aspiration Cytology (FNAC)
What it does: Aspirates individual cells; cytology shows cell morphology but NOT tissue architecture.
When to use:
• Suspected metastatic carcinoma (cell type, e.g., adenocarcinoma vs squamous) — architecture irrelevant.
• Tuberculous lymphadenitis — caseous material, epithelioid granulomas identifiable on smear, ZN stain for AFB.
• Reactive lymphadenopathy — polymorphous population of lymphocytes supports benign diagnosis.
Limitations: Cannot subclassify lymphoma reliably (requires architecture, immunohistochemistry, flow cytometry on intact tissue).
Excision Biopsy (or core biopsy with IHC)
What it does: Provides the entire node with architecture intact; allows immunohistochemistry (IHC), flow cytometry, cytogenetics (FISH for translocations), and molecular studies.
When to use:
• Suspected lymphoma — ALWAYS excision biopsy. This is non-negotiable. Lymphoma subclassification (Hodgkin vs NHL, and the specific subtype of NHL) is ONLY possible with intact architecture. Reed-Sternberg cells in Hodgkin lymphoma, follicular vs diffuse pattern in NHL — all require histology.
• Persistent lymphadenopathy > 6 weeks with no obvious cause after FNAC.
• Failed FNAC (insufficient material, atypical cells).
The key principle: Architecture = lymphoma diagnosis. Cytology alone cannot classify lymphoma.
Practical sequence for a suspicious node:
1. Clinical history + examination (distribution, consistency, B symptoms, age).
2. Blood work: CBC, ESR, LDH, LFT, viral serology (EBV/CMV/HIV) if clinically indicated.
3. Imaging: CECT to characterise node and look for primary (for suspected metastasis) or mediastinal/abdominal disease (for suspected lymphoma).
4. FNAC first if rapid confirmation needed (for clinically obvious TB or metastatic carcinoma).
5. Excision biopsy if lymphoma suspected, FNAC inconclusive, or persistence > 6 weeks.
CLINICAL PEARL
Why you should NEVER do FNAC alone for suspected lymphoma:
A cytology report saying "atypical lymphoid cells" or even "consistent with lymphoma" from FNAC is insufficient to start chemotherapy. Oncologists need the WHO subtype (e.g., Diffuse Large B-cell Lymphoma vs Follicular Lymphoma vs Burkitt Lymphoma) because each has a different treatment protocol and prognosis. This classification requires Reed-Sternberg cell morphology, the follicular vs diffuse growth pattern, IHC (CD20, CD3, CD10, bcl-6, cyclin D1, etc.), and sometimes FISH for translocations — none of which are possible on aspirated cells. Send the whole node.
Putting It Together: A Framework for the Clinic
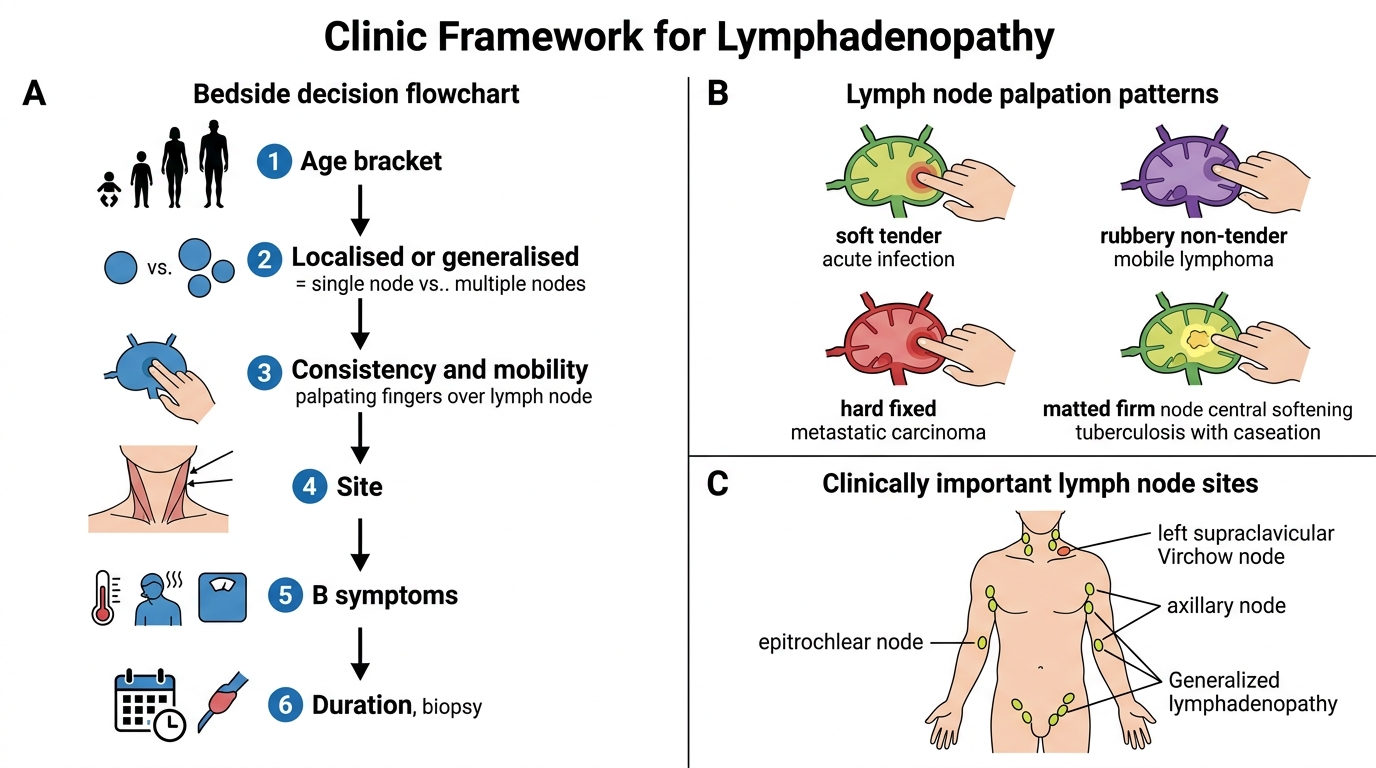
Clinic Framework for Lymphadenopathy
Use this mental checklist at the bedside:
Step 1 — Age bracket?
< 14 → reactive most likely. 15–35 → EBV, lymphoma. > 50 → malignancy prominent.
Step 2 — Localised or generalised?
Generalised → systemic cause (viral, autoimmune, haematological malignancy).
Step 3 — Consistency and mobility?
• Rubbery + non-tender + mobile → lymphoma.
• Hard + fixed → metastatic carcinoma.
• Soft + tender → acute infection.
• Matted + firm + central softening → TB (with caseation).
Step 4 — Site?
Left supraclavicular (Virchow's) → abdominal/thoracic primary. Epitrochlear → sarcoid, syphilis.
Step 5 — B symptoms?
Present → lymphoma workup mandatory.
Step 6 — Duration?
< 2 weeks + tender + localised after obvious infection → observe with antibiotics.
> 6 weeks + unexplained → biopsy.

Stepwise Diagnostic Flowchart for Lymphadenopathy
SELF-CHECK
A 17-year-old presents with 3-week history of generalised lymphadenopathy, fever, sore throat, and fatigue. Peripheral blood smear shows > 10% atypical lymphocytes. Which reactive hyperplasia pattern is MOST consistent with this clinical picture?
A. Follicular hyperplasia with polarised germinal centres
B. Paracortical hyperplasia with immunoblastic expansion
C. Sinus histiocytosis with dilated medullary sinuses
D. Granulomatous lymphadenitis with caseation
Reveal Answer
Answer: B. Paracortical hyperplasia with immunoblastic expansion
This is classic infectious mononucleosis (EBV). EBV infects B cells but the dramatic lymphadenopathy (and the circulating atypical lymphocytes = reactive CD8+ T cells) reflects intense T-cell activation → paracortical hyperplasia. The paracortex expands with immunoblasts (transformed T cells); follicles may be compressed. Atypical lymphocytes on smear are cytotoxic T cells destroying EBV-infected B cells. Follicular hyperplasia (A) would indicate B-cell stimulation (RA, autoimmune). Sinus histiocytosis (C) suggests regional carcinoma. Granulomatous (D) fits TB.
Bridge to SDL2, SDL3, and SDL4

Lymph Node Architecture as the Bridge to SDL2-4
This module has given you the framework. The next three SDLs apply it to specific diseases:
SDL2 — Tuberculous Lymphadenitis:
The commonest cause of lymphadenopathy in India. You will learn the morphological spectrum (follicular hyperplasia → epithelioid granulomas → caseation → collar-stud abscess), Langhans giant cells, ZN staining, and the paradox of lymphocyte trapping that masks positive FNAC.
SDL3 — Hodgkin Lymphoma:
The prototype rubbery, non-tender, localised lymphadenopathy of the young adult. You will learn Reed-Sternberg cells, the Ann Arbor staging, and the four histological subtypes. Paracortical destruction by the malignant process builds on the paracortical hyperplasia you learned today.
SDL4 — Non-Hodgkin Lymphoma:
The heterogeneous group — from indolent follicular lymphoma (bcl-2 you saw today) to aggressive DLBCL and Burkitt lymphoma. The concept of follicular architecture mimicking follicular hyperplasia you learned here will be the diagnostic challenge in SDL4.
The architecture of a lymph node you reviewed in the Recall block is the lens through which all four SDLs are read.