Page 6 of 13
PS1.2-3 | Psychiatric History and Mental Status Examination — SDL Guide (Part 2)
The Mental Status Examination: Structure and Sequence
The Mental Status Examination (MSE) is a structured, systematic assessment of the patient's current mental functioning at the time of the interview — analogous to the physical examination in general medicine. Unlike the history (which covers the longitudinal course of illness), the MSE is a cross-sectional snapshot of the patient's present mental state. It should be conducted alongside the history rather than after it, because many MSE domains are best assessed through observation during the interview itself.
Provided image
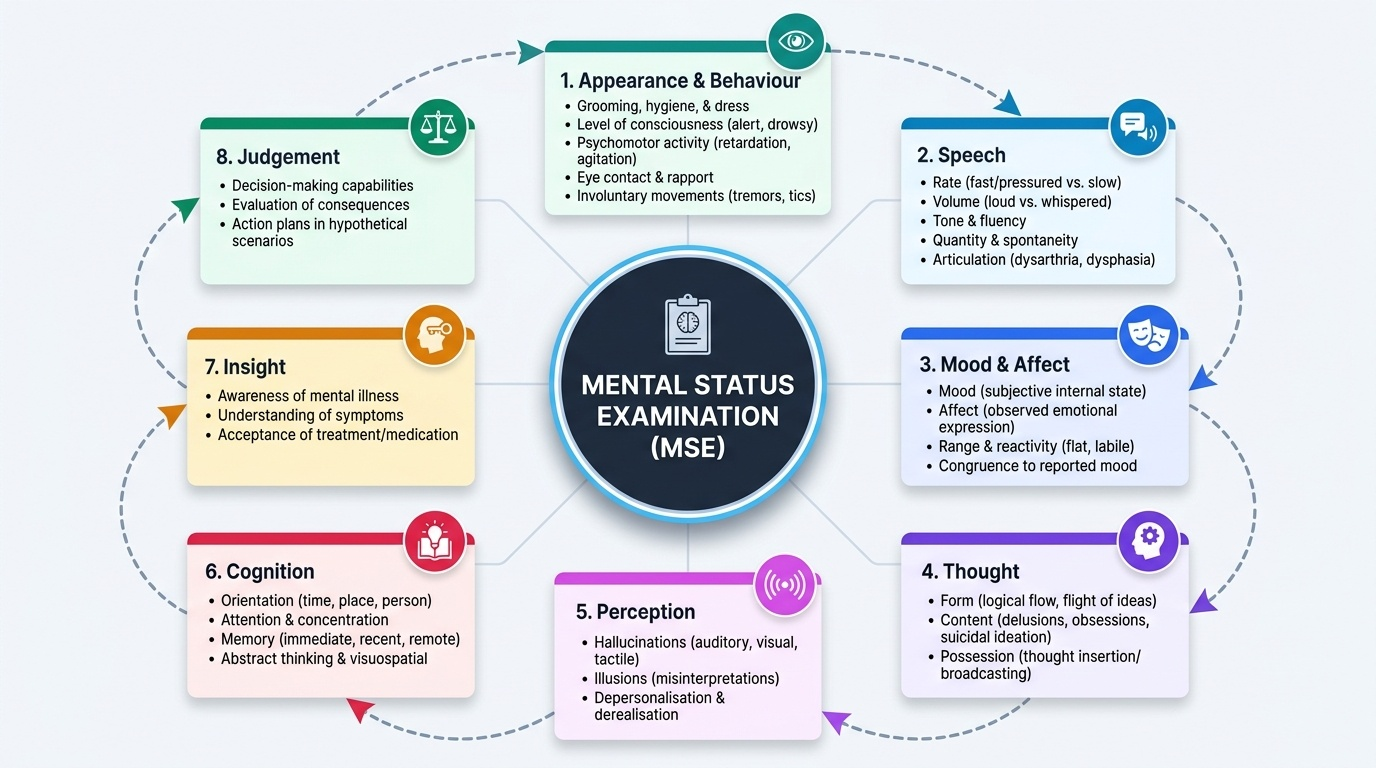
The MSE is organised across eight standard domains, which must be systematically covered and documented in every psychiatric assessment. The mnemonic ASMT-PCT or the sequential structure below can be used as an aide-memoire. Each domain is described below with its key components and clinical significance:
Domain 1: Appearance and Behaviour — Assess the patient's general appearance (personal hygiene, grooming, dress — are they dishevelled? overdressed? wearing unusual items?); level of consciousness (alert, drowsy, stuporous); psychomotor activity (retardation — slow, slumped posture, poverty of movement, long response latency; agitation — restlessness, pacing, inability to sit still; catatonic features — posturing, waxy flexibility, mutism, negativism, echopraxia); eye contact; rapport; any involuntary movements (tardive dyskinesia, tremor, akathisia).
Domain 2: Speech — Assess rate (fast in mania/anxiety, slow in depression), volume (loud in mania, whispered in depression), tone, fluency, quantity (pressure of speech = rapid, continuous, difficult to interrupt, seen in mania; poverty of speech = laconic, monosyllabic, seen in schizophrenia and depression), and spontaneity. Note any dysarthria (slurred speech suggesting intoxication or neurological cause) or dysphasia (indicating a neurological lesion).
Domain 3: Mood and Affect — Mood is the subjective, internal emotional state as reported by the patient ('How have you been feeling inside?') — described in the patient's own words (e.g. 'I feel empty,' 'I feel on top of the world'). Affect is the external, objective expression of emotion observed by the clinician — assess: quality (elated, depressed, anxious, irritable, hostile, dysphoric, euthymic); range (full range vs. restricted vs. flat/blunted vs. labile); reactivity (does the affect change appropriately with conversational content?); congruence with mood and thought content (does the patient laugh while discussing a tragedy? = incongruence, seen in schizophrenia).
Domain 4: Thought — This is the most complex and clinically important domain, assessed across three sub-dimensions:
Form of thought (the way thoughts are organised and expressed): flight of ideas (rapid succession of loosely connected thoughts, with discernible links; seen in mania); loosening of associations / formal thought disorder (ideas lack logical connection; seen in schizophrenia); thought blocking (abrupt cessation mid-sentence, patient cannot continue; may indicate thought withdrawal in schizophrenia); circumstantiality (verbose, indirect but eventually reaches the point; seen in anxiety and mania); tangentiality (goes off on tangents and never reaches the point); perseveration (repeating the same idea or phrase; seen in organic disorders); clang associations (rhyming, punning); neologisms (invented words).
Content of thought: delusions (types: persecutory — most common; reference — neutral events have special personal meaning; grandiose; nihilistic — body is rotting, world has ended; somatic; erotomanic; jealous/morbid jealousy; religious; thought insertion, thought withdrawal, thought broadcasting — specific first-rank symptoms of Schneider). Also assess: overvalued ideas (strongly held but not fixed beyond all argument; OCD, eating disorders); phobias (morbid, excessive fear of specific objects/situations); obsessions (intrusive, ego-dystonic, recurrent thoughts); suicidal and homicidal ideation — always specifically asked.
Possession of thought (Schneider's first-rank symptoms): thought insertion (thoughts placed into the mind by an external force), thought withdrawal, thought broadcasting (thoughts transmitted to others).
Domain 5: Perception — Assess for hallucinations in all modalities: auditory (second-person commanding or commenting; third-person discussing the patient — running commentary or discussing in third person are Schneider first-rank symptoms); visual; tactile (formication — insects crawling, seen in cocaine/alcohol withdrawal); olfactory; gustatory. Also assess for illusions (misinterpretation of real stimuli) and pseudohallucinations (hallucinations recognised as arising from within the mind, not external space). Depersonalisation (feeling detached from one's own mental processes or body) and derealisation (feeling that the external world is unreal).
Domain 6: Cognition — Assess: orientation (time, place, person); attention and concentration (Serial 7s — subtract 7 from 100 serially; WORLD backwards; Digit span); memory (immediate recall: repeat 3 items; short-term: recall after 5 min; long-term: recent and remote events); abstract thinking (proverb interpretation — concrete vs. abstract; similarities: in what way are an apple and a banana similar?); intelligence (general knowledge questions calibrated to educational level).
Domain 7: Insight — The degree to which the patient recognises that they are ill, understands that the illness is psychiatric in nature, and acknowledges that treatment is needed. Ahuja grades insight on a 6-point scale: Grade 0 (no awareness of illness) to Grade 6 (full awareness and voluntary seeking of help). Impaired insight is characteristic of psychotic disorders and mania; preserved insight is characteristic of neurotic disorders and early depression.
Domain 8: Judgement — The patient's capacity to make reasonable decisions about everyday situations. Assessed by asking about their plans for managing their current situation, their understanding of why they are in hospital, and their response to hypothetical situations (e.g. 'What would you do if you found a sealed, stamped, addressed envelope on the street?'). Judgement and insight are closely related but distinct — a patient may have some insight ('I know I have a mental illness') while still having impaired judgement ('but I don't need to take medication or see a doctor').
SELF-CHECK
During the MSE, a patient with acute psychosis denies having any illness and states he has come to hospital only because his family insisted. He agrees that the voices he hears are real external voices, not symptoms of illness. Which assessment of insight is most accurate?
A. Full insight — he acknowledges the voices
B. Partial insight — he recognises distress but not the psychiatric cause
C. Impaired insight — he does not recognise the experiences as illness symptoms
D. Insight cannot be assessed without formal cognitive testing
Reveal Answer
Answer: C. Impaired insight — he does not recognise the experiences as illness symptoms
Insight in psychiatry refers specifically to the patient's awareness that their experiences are symptoms of a mental illness. This patient does not recognise his voices as illness symptoms — he believes them to be real external perceptions. This constitutes impaired insight, which is characteristic of psychotic disorders. Insight does not require the ability to name the diagnosis — it requires awareness that one's mental experiences are abnormal and that one has an illness. Insight assessment does not require formal cognitive testing.
Interpreting MSE Findings: Mapping to Diagnostic Patterns
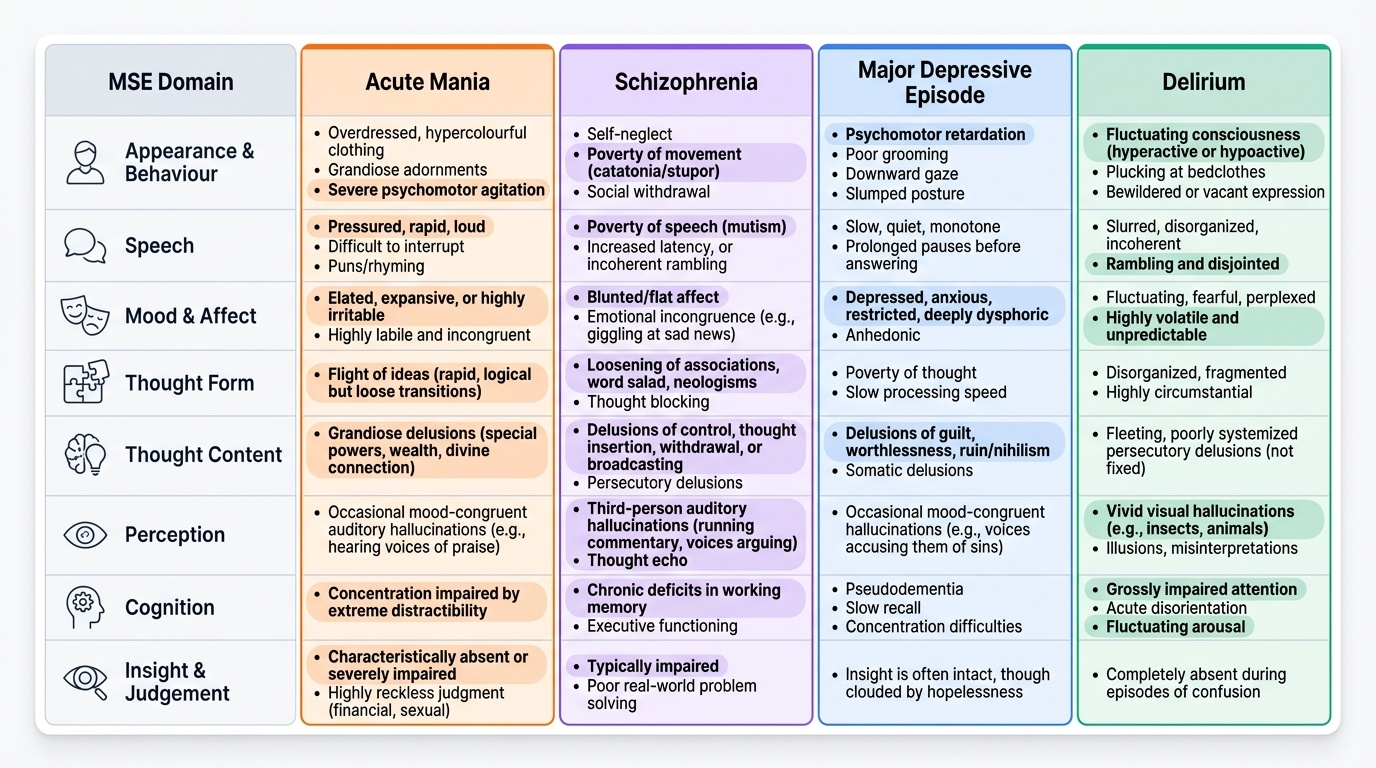
The real clinical value of the MSE lies not in documenting individual findings in isolation, but in recognising the patterns of findings that characterise specific diagnostic categories and in reasoning from abnormal findings to their likely underlying disorder. This section maps the key MSE abnormalities to their diagnostic correlates, with the caveat that no single MSE finding is pathognomonic — the diagnosis requires integrating the MSE with the full psychiatric history.
Provided image
Pattern 1: Acute mania. Appearance: overdressed, hypercolourful clothing, possibly grandiose adornments; psychomotor agitation. Speech: pressured, rapid, loud, difficult to interrupt. Mood: elated, expansive, or irritable (irritability is common when mania is resisted). Affect: labile, full, incongruent at times. Thought form: flight of ideas (connected but rapid topic changes). Thought content: grandiose delusions (inflated self-importance, special powers, special relationship with God or powerful figures); reduced need for sleep not experienced as fatigue. Perception: occasionally mood-congruent hallucinations. Cognition: attention and concentration usually impaired by distractibility. Insight: characteristically impaired — patients rarely present voluntarily. Judgement: severely impaired (financial recklessness, sexual disinhibition, risk-taking). Duration: manic episode ≥1 week (ICD-11/DSM-5) or any duration requiring hospitalisation.
Pattern 2: Schizophrenia. Appearance: self-neglect, poverty of movement, social withdrawal. Speech: poverty of speech, latency increased, or at times pressured and incoherent. Mood: blunted or flat affect, emotional incongruence (inappropriate giggling). Thought form: loosening of associations, tangentiality, blocking, neologisms. Thought content: persecutory delusions, ideas of reference, delusions of control, thought insertion/withdrawal/broadcasting (Schneider first-rank symptoms). Perception: third-person auditory hallucinations (running commentary, discussion in third person), thought echo (also Schneider FRS). Cognition: working memory and executive function impaired even in acute episodes. Insight: typically impaired. Duration of core symptoms ≥1 month (ICD-11), ≥6 months total (DSM-5).
Pattern 3: Major depressive episode. Appearance: psychomotor retardation, poor grooming, downward gaze. Speech: slow rate, decreased volume, decreased spontaneity, long response latency. Mood: subjectively depressed, empty, hopeless, worthless ('I feel like a burden to everyone'). Affect: restricted, congruent with mood. Thought form: normal but slowed. Thought content: worthlessness, guilt, hopelessness, suicidal ideation (passive — 'I wish I were dead' — or active — 'I am planning to take tablets'); somatic preoccupations; occasionally nihilistic delusions in severe depression with psychotic features. Perception: hallucinations only in psychotic depression. Cognition: poor concentration and memory (pseudodementia in severe depression — may mimic dementia in elderly). Insight: usually preserved. Duration: ≥2 weeks (ICD-11/DSM-5).
Pattern 4: Delirium (organic disorder). Appearance: restless, confused, often looking around fearfully; fluctuating level of consciousness (cardinal feature). Speech: disorganised, incoherent, fluctuating. Mood: fearful, agitated, perplexed. Thought: disorganised, fragmented. Perception: visual hallucinations are most characteristic (as opposed to auditory, which predominate in primary psychotic disorders); illusions. Cognition: impaired orientation (time first, then place, then person), impaired attention (fails Serial 7s), recent memory severely impaired. Insight: absent (patient is too confused to have insight). This pattern demands urgent medical investigation — the underlying cause (infection, metabolic derangement, drug toxicity, withdrawal) must be identified and treated.
The presence of visual hallucinations, disorientation (especially to time and place), and fluctuating consciousness strongly suggests an organic disorder (delirium or organic psychosis) rather than a primary psychiatric disorder. Primary schizophrenia almost never causes disorientation or visual hallucinations as the predominant feature — if these are present, organic causes must be urgently excluded.
SELF-CHECK
A 70-year-old retired teacher presents with 3 days of visual hallucinations (seeing small animals in the room), confusion, and agitation that worsens at night. She is oriented to her name but not to the date or place. What does this MSE pattern most strongly suggest?
A. Paranoid schizophrenia — she has hallucinations and agitation
B. Manic episode with psychotic features — she is agitated and disinhibited
C. Delirium — visual hallucinations, disorientation, and nocturnal worsening indicate an organic cause
D. Major depressive disorder with psychotic features — elderly women are at high risk
Reveal Answer
Answer: C. Delirium — visual hallucinations, disorientation, and nocturnal worsening indicate an organic cause
This MSE pattern is diagnostic of delirium: visual hallucinations (characteristically organic), disorientation (to time and place but not person — the typical sequence), nocturnal worsening ('sundowning'), and acute onset in an elderly patient. Schizophrenia does not typically cause visual hallucinations or disorientation as the predominant features in an elderly patient without prior psychiatric history. The priority is to identify the organic cause (infection, drug toxicity, metabolic derangement, intracranial pathology) and treat it.
Applied Practice: Conducting the Interview and Writing the Formulation
The practical application of psychiatric history-taking and MSE skills involves integrating the structured framework above with real-time adaptation to the patient's mental state, communication abilities, and cultural context. This section addresses the applied dimensions that distinguish a competent clinician from one who has merely memorised the checklist.
Managing the acutely disturbed patient: When a patient is agitated, threatening, or refusing to engage, the clinician's priority is safety — of the patient, the clinician, and others in the clinical area. Ensure adequate space and an open exit; speak in a calm, quiet, non-confrontational tone; avoid challenging delusions or arguing with hallucinated voices; acknowledge the patient's distress without endorsing the delusional content ('I can see you are very frightened — I want to help you'); and involve a colleague for safety if needed. The MSE can be abbreviated in the acutely disturbed state and completed more fully once the patient is settled.
Managing the mute or catatonic patient: Do not assume a mute patient is 'unresponsive' — catatonic patients may have preserved awareness despite appearing unresponsive. Observe carefully for posturing, waxy flexibility, echopraxia, and other catatonic features. Speak gently and document what you observe. Catatonia can occur in schizophrenia, mood disorders, and organic states and is a medical emergency when associated with fever, autonomic instability, or nutritional compromise (malignant catatonia).
Cultural adaptation: In India, psychiatric interviewing must be sensitive to the high rate of somatic presentation of psychological distress — depression and anxiety commonly present as headache, chest pain, fatigue, burning sensations, and musculoskeletal pain rather than as primary emotional complaints. Asking about somatic symptoms as an entry point and then exploring the affective dimension is often more productive than asking directly 'Are you depressed?' Some patients may use idioms of distress that are culturally specific (e.g. 'sinking heart' for depression in some South Asian communities). An experienced clinician builds cultural competence through supervised clinical experience across diverse patient populations.
The psychiatric formulation: After the history and MSE are completed, the findings are synthesised into a psychiatric formulation — a structured narrative that covers: (1) the descriptive formulation (diagnosis or differential diagnosis, with the MSE findings that support each); (2) the aetiological formulation (predisposing, precipitating, perpetuating, and protective factors — the 'four P's'); (3) the management plan (biological, psychological, and social components); and (4) the prognosis. The formulation, rather than a bare diagnosis, is the hallmark of skilled psychiatric thinking.
Documentation and medicolegal considerations: The MSE must be clearly documented in the case notes, with specific examples rather than vague descriptors ('patient expressed persecutory beliefs that neighbours are poisoning his food through the water supply' rather than 'patient has paranoid ideas'). Under the Mental Healthcare Act 2017, documentation of mental state is required for legal proceedings involving mental illness. Accurate, specific MSE documentation also provides a baseline against which future assessments can be compared to track treatment response.
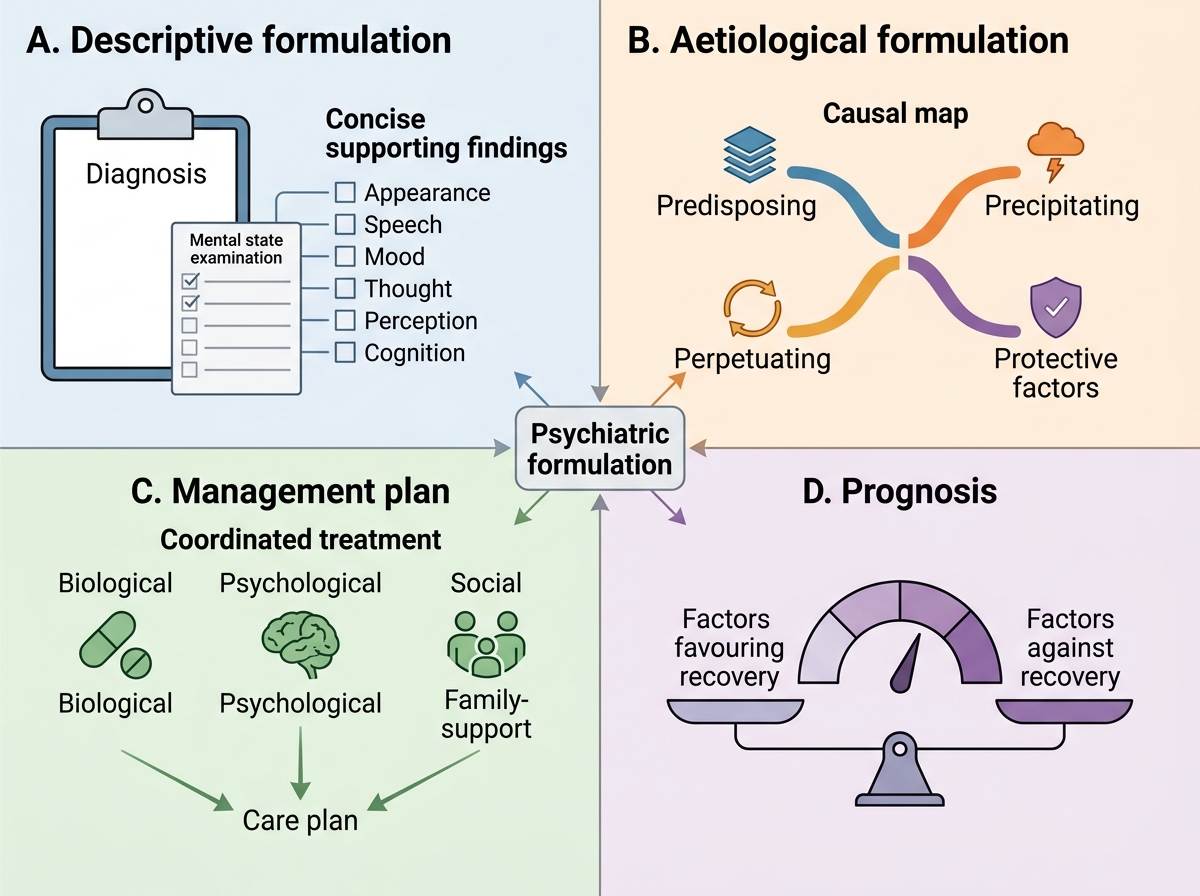
Structure of Psychiatric Formulation