Page 1 of 8
PS4.1 | Schizophrenia at Primary Care Level — SDL Guide
Learning Objectives
- Identify the clinical features of schizophrenia, including positive, negative, and cognitive symptom clusters
- Apply ICD-11 and DSM-5 diagnostic criteria with correct duration thresholds at primary care
- Conduct a focused Mental Status Examination relevant to a suspected psychotic presentation
- Initiate first-line antipsychotic treatment, monitor for adverse effects, and arrange safe referral
- Counsel families and plan community follow-up for a patient with schizophrenia at primary care level
INSTRUCTIONS
Schizophrenia is a chronic psychotic disorder that affects roughly 1% of the global population and carries immense personal, family, and societal burden. As a primary care physician you will be the first professional many patients with schizophrenia encounter — the quality of your initial assessment, the promptness of treatment initiation, and the warmth of your psychosocial support directly shape long-term outcomes. This module equips you with the clinical knowledge and practical skills to diagnose, initiate treatment, and manage schizophrenia within a primary care context, including knowing when and how to refer to a specialist.
References
- Ahuja N. A Short Textbook of Psychiatry, 8th ed. Jaypee Brothers, Ch 5 (textbook)
- Sadock BJ, Sadock VA, Ruiz P. Kaplan & Sadock's Synopsis of Psychiatry, 11th ed. Wolters Kluwer, Ch 7 (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 24-year-old engineering student is brought to your primary health centre by his worried parents. Over the past three months he has stopped attending college, locks himself in his room for hours, talks to himself, and insists that his classmates are sending coded messages through the television to spy on him. His personal hygiene has deteriorated and he appears emotionally flat during your interview. His parents are distraught and ask: "Doctor, is he losing his mind? Can we take care of him at home?" How you respond in the next 30 minutes will set the trajectory for this young man's next decade.
WHY THIS MATTERS
Schizophrenia affects approximately 1 in 100 people worldwide — in India this translates to over 10 million individuals, the vast majority of whom first present to general practitioners or primary care facilities rather than psychiatric centres. Early recognition and timely initiation of treatment are the two variables most strongly linked to long-term functional recovery. A delay of even one year in treatment significantly worsens prognosis. As a primary care physician practising under the Mental Healthcare Act 2017 (which replaced the Mental Health Act 1987 and decriminalised suicide attempt), you carry both a legal duty of care and a practical gatekeeping role: you will be the person who recognises the illness, starts first-line therapy, provides family psychoeducation, and coordinates specialist referral — skills this module builds directly.
RECALL
Before proceeding, take a moment to retrieve what you already know. From your Year-1 physiology and biochemistry studies, recall the major neurotransmitter systems: dopamine pathways (mesolimbic, mesocortical, nigrostriatal, tuberoinfundibular), serotonin (5-HT) receptor distribution, and glutamate NMDA receptors. From your basic psychiatry orientation, recall the definition of a psychosis — a state in which reality testing is lost — and the broad distinction between functional and organic causes. From clinical pharmacology, remind yourself what a D₂ receptor antagonist does. These building blocks will make the pathophysiology and pharmacology of schizophrenia easier to integrate.
Clinical Presentation of Schizophrenia
Schizophrenia presents across a broad clinical spectrum that is best understood by organising its features into three symptom clusters: positive symptoms, negative symptoms, and cognitive symptoms. This three-cluster framework is more clinically useful than the older binary of 'positive versus negative' because it guides both pharmacological targeting and functional outcome prediction.
Positive symptoms represent the addition of experiences that are absent in healthy individuals. They include delusions — fixed, false, unshakeable beliefs that are out of keeping with the patient's cultural background (e.g. persecutory delusions, delusions of reference, grandiose or nihilistic delusions); hallucinations — most commonly auditory (voices commenting on the patient's actions or giving commands, or two or more voices conversing), though visual, olfactory, and tactile hallucinations may also occur; disorganised thinking (formally termed thought disorder) manifesting as loose associations, tangentiality, or incoherence; and grossly disorganised or catatonic behaviour, which can range from unpredictable agitation to complete stupor.
Negative symptoms represent the diminution or loss of normal functions. The core negative symptoms, remembered by the mnemonic 5As, are: avolition (lack of motivation and drive), alogia (poverty of speech), anhedonia (inability to experience pleasure), affective flattening (reduced emotional expression), and asociality (social withdrawal). Negative symptoms are often more disabling than positive symptoms in the long run, are associated with worse functional outcomes, and respond less robustly to antipsychotic medication.
Cognitive symptoms include impairments in working memory, attention, processing speed, and executive function. These are present in most patients with schizophrenia, often precede the first psychotic episode by years, and are the strongest predictors of occupational and social functioning.
For teaching purposes, Kurt Schneider's First-Rank Symptoms (FRS) retain historical and mnemonic value: they include auditory hallucinations in the third person, thought insertion, thought withdrawal, thought broadcasting, and somatic passivity experiences. It is important to understand that FRS are neither diagnostic (they appear in other psychoses) nor necessary for the diagnosis — their utility today is primarily pedagogical.
The natural history typically begins with a prodromal phase of non-specific social withdrawal, declining academic or occupational performance, odd beliefs, and perceptual distortions. This is followed by one or more acute psychotic episodes, and then a residual phase in which negative and cognitive symptoms predominate between episodes. The earlier the treatment is initiated, the shorter the untreated psychosis duration, and the better the long-term prognosis.
IMPORTANT: Always perform a thorough physical examination and appropriate investigations (blood glucose, TFTs, urine drug screen, CT/MRI brain where indicated) to exclude organic causes of psychosis — substance intoxication or withdrawal, delirium, encephalitis, brain tumour, hyperthyroidism, SLE, and metabolic encephalopathies can all mimic schizophrenia and must be ruled out before a functional psychosis is diagnosed.
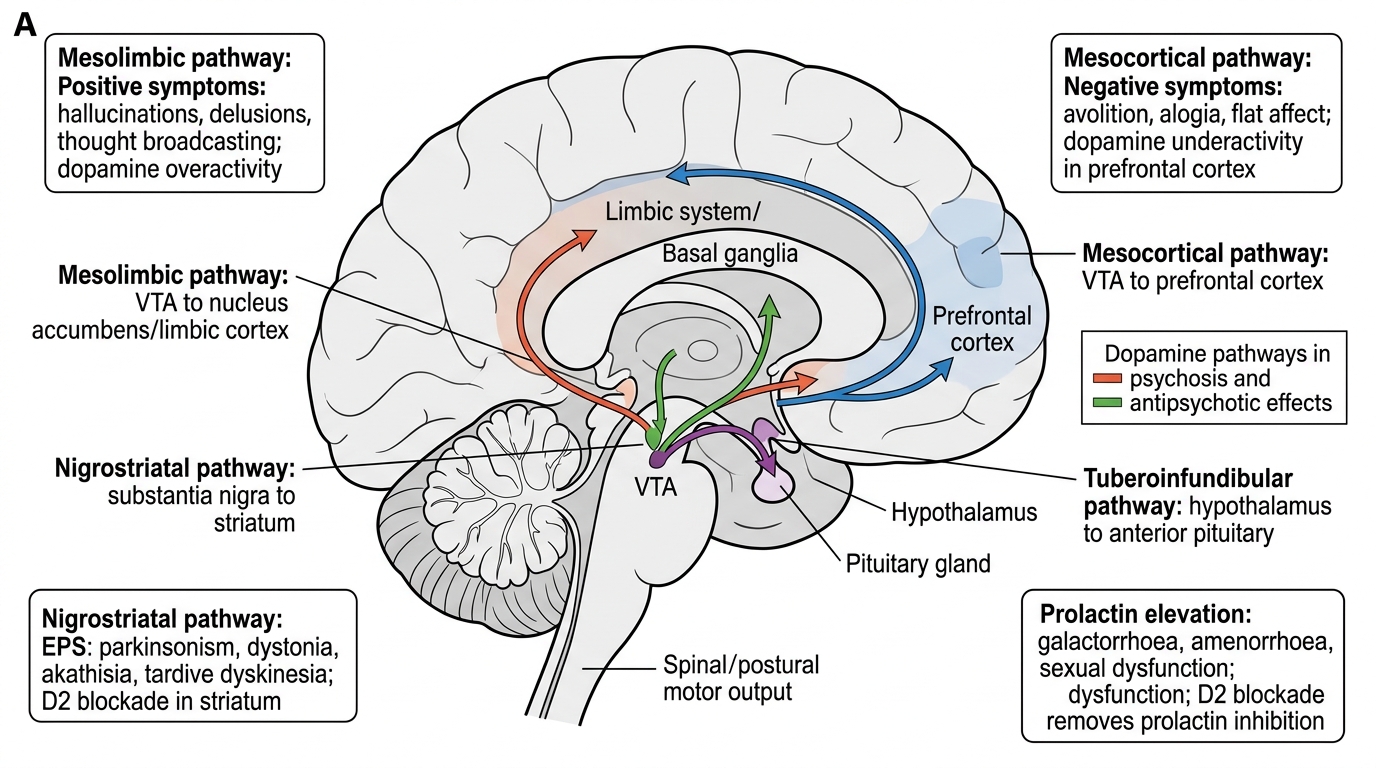
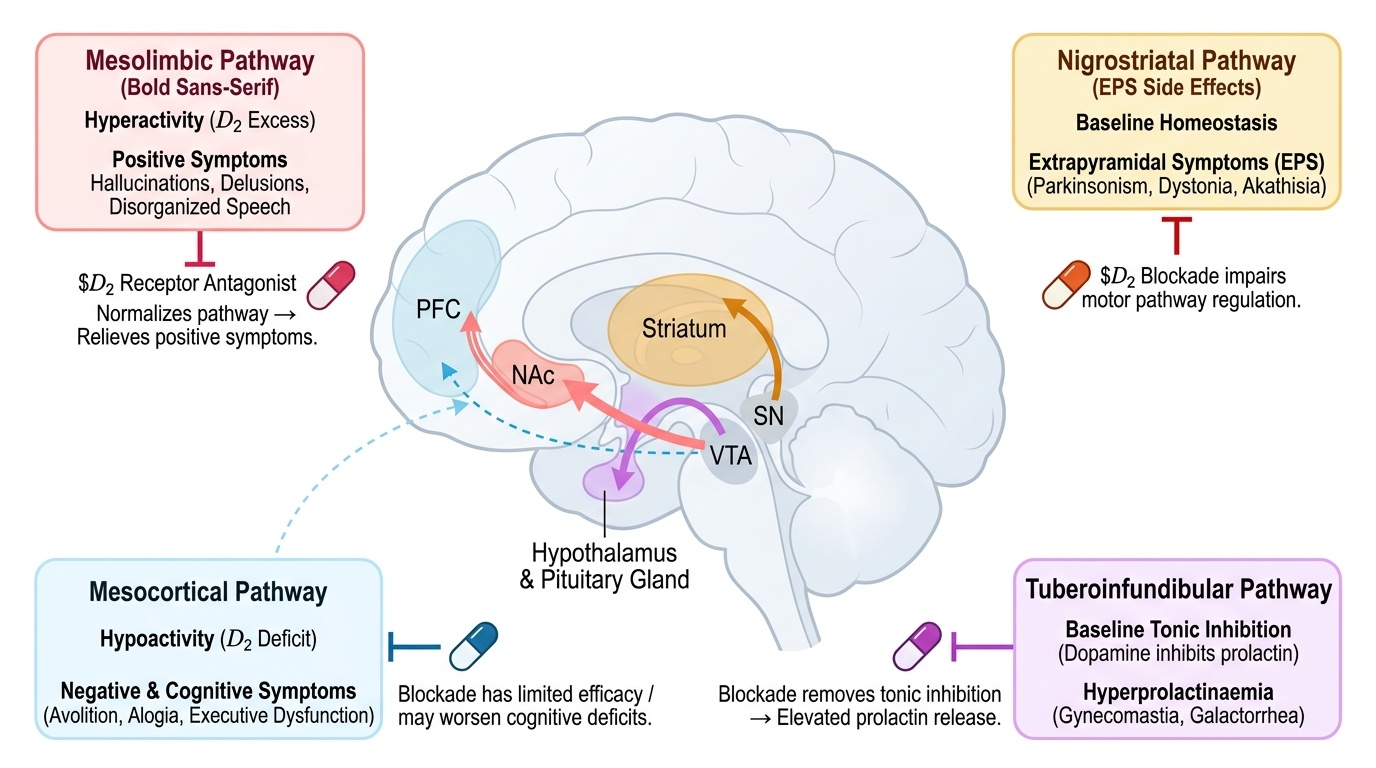
Four Dopamine Pathways in Psychotic Disorders
SELF-CHECK
A 22-year-old man reports that his thoughts are being broadcast to everyone around him and that he can hear two voices discussing his actions. Which symptom cluster do these experiences primarily represent?
A. Negative symptoms
B. Cognitive symptoms
C. Positive symptoms
D. Residual symptoms
Reveal Answer
Answer: C. Positive symptoms
Thought broadcasting and auditory hallucinations (voices commenting or conversing) are positive symptoms — they represent experiences added to normal mental life that do not exist in health. They are also examples of Schneider's First-Rank Symptoms. Negative symptoms (avolition, alogia, anhedonia, flat affect, asociality) represent diminished functions, while cognitive symptoms include working memory and executive function deficits.
Psychopathology and Aetiology
Understanding why schizophrenia occurs requires integrating neurobiological, genetic, and environmental evidence into a coherent aetiological framework. No single cause has been identified; instead, schizophrenia is best understood as a neurodevelopmental disorder with a complex multifactorial aetiology, where genetic vulnerability interacts with environmental stressors during critical periods of brain development.
Provided image
The dopamine hypothesis remains the most clinically relevant neurochemical model. In its refined form (the revised dopamine hypothesis), there is subcortical dopaminergic hyperactivity in the mesolimbic pathway, which correlates with positive symptoms, and prefrontal dopaminergic hypoactivity in the mesocortical pathway, which correlates with negative symptoms and cognitive deficits. This distinction explains why antipsychotics (which are D₂ receptor antagonists) effectively reduce positive symptoms but have limited efficacy against negative and cognitive symptoms — they address the mesolimbic excess but cannot compensate for the mesocortical deficit.
The glutamate (NMDA receptor hypofunction) hypothesis complements the dopamine model. NMDA receptor antagonists such as phencyclidine (PCP) and ketamine produce a schizophrenia-like syndrome encompassing positive, negative, and cognitive symptoms — an observation that the dopamine model alone cannot replicate. Decreased NMDA receptor activity on GABAergic interneurons leads to disinhibition of downstream dopaminergic and glutamatergic circuits, providing a mechanism that unifies both positive and negative symptoms.
From a genetic standpoint, the heritability of schizophrenia is approximately 80%. The concordance rate in monozygotic twins is around 40–50% (not 100%), confirming that genes are necessary but not sufficient. First-degree relatives have a lifetime risk of approximately 10%, compared to 1% in the general population. Multiple genes of small effect are implicated — copy number variants (CNVs), GWAS hits involving DISC1, COMT (catechol-O-methyltransferase), and neuregulin-1 — rather than any single causative gene.
Environmental risk factors that interact with genetic vulnerability include advanced paternal age, prenatal infections (influenza, rubella) particularly in the second trimester, obstetric complications (perinatal hypoxia), urban upbringing, migration stress, childhood adversity and trauma, and cannabis use (especially high-THC potency strains in adolescence). Cannabis use is a dose-dependent risk factor: the risk of psychosis is approximately doubled with regular cannabis use and further increased with daily heavy use starting in early adolescence.
Neuroanatomically, post-mortem and neuroimaging studies consistently reveal lateral ventricular enlargement, reduced volume of the hippocampus and prefrontal cortex, and reduced total grey matter — changes that predate onset and progress slowly, particularly during the first few years of illness.
Diagnosis and Mental Status Examination
Diagnosing schizophrenia at primary care requires the clinician to apply a formal diagnostic framework while simultaneously conducting a systematic Mental Status Examination (MSE). Both the ICD-11 and DSM-5 criteria must be understood because different specialist referral letters, prescribing guidelines, and research literature reference each system, and the duration thresholds differ critically between them.
Provided image
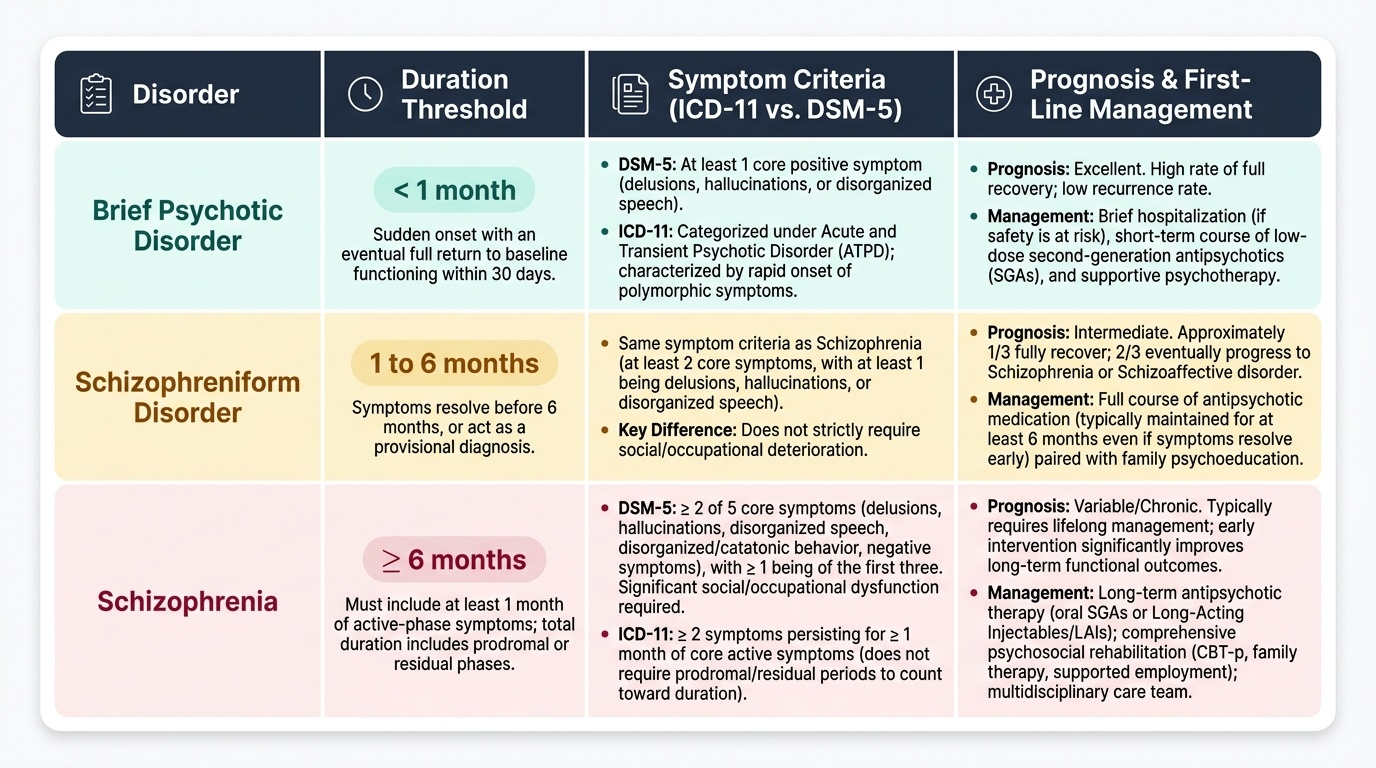
Under ICD-11, the diagnosis of schizophrenia requires the presence of characteristic psychotic symptoms (at least two from: delusions, hallucinations, disorganised thinking, disorganised behaviour, negative symptoms, or psychomotor disturbances) persisting for at least 1 month of core active symptoms. The ICD-11 does not require a prodromal or residual period to be counted in the minimum duration.
Under DSM-5, the diagnosis requires at least two of five core symptoms (delusions, hallucinations, disorganised speech, grossly disorganised or catatonic behaviour, negative symptoms — with at least one of the first three being present) that must be present for a significant portion of at least 1 month of active phase, with total duration including prodrome and residual phase of at least 6 months. This longer DSM-5 window is specifically designed to distinguish schizophrenia from briefer psychotic disorders such as brief psychotic disorder (<1 month) and schizophreniform disorder (1–6 months). When counselling families or writing referral letters, always state which classification system you are using and its specific threshold.
The Mental Status Examination (MSE) is the psychiatrist's equivalent of the physical examination and must be conducted systematically in every suspected case. Its components and their relevance to schizophrenia are:
- Appearance and behaviour: self-neglect, bizarre dress, catatonic posturing, limited eye contact, psychomotor retardation or agitation
- Speech: poverty of speech (alogia), tangential, circumstantial, derailment (loosening of associations), neologisms, word salad in severe cases
- Mood and affect: often discordant — the patient may describe a neutral mood while appearing emotionally flat or inappropriately affect
- Thought content: elicit delusions by open-ended questioning — ask about unusual experiences, fears, beliefs about persecution or special powers
- Thought form: assess logical coherence, flow and connectivity of ideas
- Perceptions: screen for hallucinations in all modalities, particularly auditory ("Do you hear voices when no one is around?")
- Cognition: brief orientation, memory, attention screening (digit span, serial subtraction)
- Insight and judgement: most patients in an acute episode have impaired insight — assessing degree of insight guides treatment planning and legal considerations under the Mental Healthcare Act 2017
The differential diagnosis at primary care includes: organic psychoses (rule out first), bipolar disorder with psychotic features (distinguish by longitudinal mood history), severe depression with psychotic features (mood-congruent delusions, prominent depressive symptoms), substance-induced psychosis (temporal relationship with use, resolves on cessation), delusional disorder (circumscribed delusions, personality and functioning largely preserved), and acute and transient psychotic disorder / brief psychotic disorder (sudden onset, duration <1 month, good premorbid functioning).
SELF-CHECK
A patient meets all symptomatic criteria for schizophrenia but has had continuous symptoms for only 10 weeks with no prodromal period. Which classification correctly describes this presentation?
A. Schizophrenia by both ICD-11 and DSM-5
B. Schizophrenia by ICD-11 only (≥1 month met); schizophreniform disorder by DSM-5 (total duration <6 months)
C. Brief psychotic disorder by both systems
D. Schizophrenia by DSM-5 only
Reveal Answer
Answer: B. Schizophrenia by ICD-11 only (≥1 month met); schizophreniform disorder by DSM-5 (total duration <6 months)
ICD-11 requires ≥1 month of core psychotic symptoms; 10 weeks satisfies this threshold, so ICD-11 would permit a diagnosis of schizophrenia. DSM-5, however, requires a total duration of ≥6 months (including prodrome and residual phases); 10 weeks falls short, placing this presentation in the DSM-5 category of schizophreniform disorder (1–6 months duration with schizophrenia-like features). Brief psychotic disorder requires duration <1 month — 10 weeks clearly exceeds this. This distinction underscores why citing the classification system is mandatory when discussing diagnosis.