Page 4 of 11
PS6.1 | Mania in Primary Care — SDL Guide
Learning Objectives
- Recognise the core clinical features of a manic episode (ICD-11/DSM-5), including the ≥1-week duration criterion and the hospitalisation exception
- Distinguish mania from hypomania based on severity, duration, and functional impact
- Conduct a mental status examination of a patient with suspected mania and document key findings systematically
- Identify the primary-care management priorities: safety, acute behavioural control, and early specialist referral
- Describe the role of lithium in bipolar disorder, including its therapeutic range (0.6–1.2 mEq/L), monitoring requirements, and signs of toxicity
- Explain why antidepressant monotherapy is contraindicated in bipolar depression and the risk of mania switching
INSTRUCTIONS
Mania is a psychiatric emergency that primary-care physicians will encounter — in district hospitals, emergency settings, and community clinics — often before a specialist is available. The untreated manic patient is at high risk of self-harm through reckless behaviour, financial ruin, sexual disinhibition, and breakdown of relationships. Crucially, mania is also commonly the first presentation of bipolar disorder, and the diagnostic and management decisions made at the primary-care interface shape the long-term trajectory of the illness. This module gives you the recognition skills, the immediate management framework, and the referral judgment needed to handle mania safely from the front line.
References
- Ahuja N. A Short Textbook of Psychiatry, 8th ed. New Delhi: Jaypee; 2022. Ch 7 (Mood Disorders) (textbook)
- Kaplan HI, Sadock BJ. Synopsis of Psychiatry, 11th ed. Philadelphia: Wolters Kluwer; 2015. Ch 8 (textbook)
- Mental Healthcare Act 2017. Government of India. Ministry of Law and Justice. (guideline)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 26-year-old man is brought to your district hospital by his family at midnight. He has not slept in four days but insists he has never felt better. He is speaking so rapidly that he is difficult to interrupt, switching from topic to topic. He tells you he has just donated his family's life savings to a stranger on the street 'because God told me to.' His wife says he has never behaved like this before and that in the past two months he spent all their money on a business venture that failed. He is agitated, pacing, and demanding discharge to 'complete his divine mission.' What is happening, and how dangerous is this situation?
WHY THIS MATTERS
Bipolar disorder — the overarching condition that encompasses both manic and depressive episodes — affects approximately 1–2% of the global population across all cultures and socioeconomic groups. In India, an estimated 10–15 million people live with bipolar disorder, yet the majority remain undiagnosed for many years after first presentation. The first presentation of the illness is frequently a manic episode, and it often occurs dramatically — a sudden change in behaviour that brings the patient to the attention of police, family members, or emergency services before any psychiatric diagnosis has been made. As a primary-care physician, you may be the first clinician to assess this patient. Your ability to recognise mania, prevent harm in the acute phase, and initiate the referral pathway for confirmed diagnosis and specialist-supervised long-term management can be life-changing — and potentially life-saving.
RECALL
Reactivate what you already know about mood neurobiology and pharmacology. In PY you studied the limbic system, the hypothalamic-pituitary-adrenal (HPA) axis, and the role of dopamine in the mesolimbic reward pathway — understanding this pathway helps explain the euphoria and reward-seeking behaviour that characterises mania. In PH you learnt the pharmacology of lithium, a mood stabiliser used for decades in bipolar disorder. You will now apply that pharmacological foundation to understand lithium's clinical use, its narrow therapeutic index, and the critical importance of monitoring serum levels. Recall also that you studied the monoamine hypothesis of mood disorders in the depression module; mania can be understood, in simplified terms, as a state of monoamine excess rather than deficiency.
Clinical Presentation of a Manic Episode
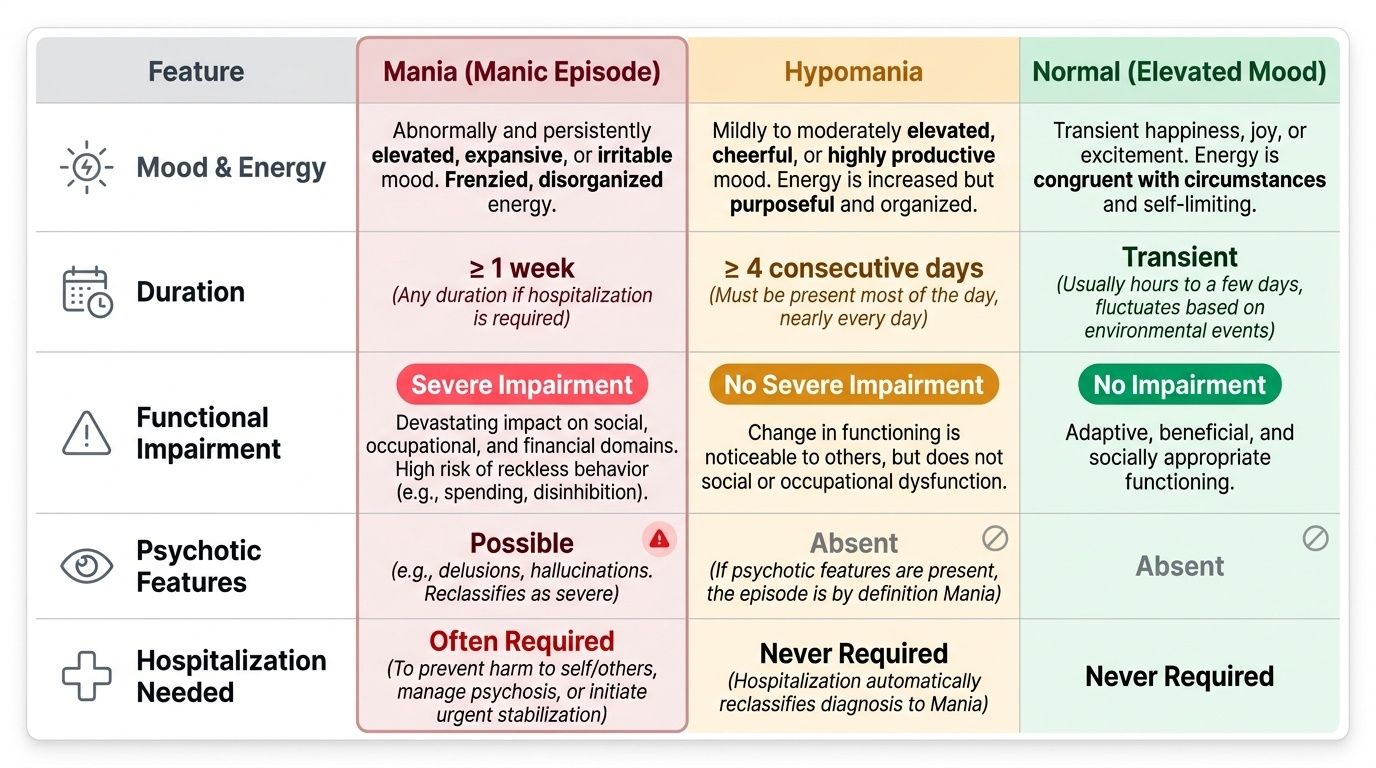
A manic episode is defined by a distinct period of abnormally and persistently elevated, expansive, or irritable mood, and abnormally and persistently increased goal-directed activity or energy. This core mood disturbance must persist for at least one week and be present for most of the day, nearly every day — or any duration if hospitalisation is required. The 'any duration if hospitalised' exception is clinically important: it recognises that severe mania may require inpatient management before a full week has elapsed. Both ICD-11 and DSM-5 encode this exception, and students should state it explicitly when citing the duration criterion.
Provided image
Alongside the core mood change, a manic episode is characterised by a cluster of associated features, summarised by the mnemonic DIG FAST — Distractibility, Irritability or inflated self-esteem, Grandiosity, Flight of ideas, Activity increase or psychomotor agitation, Sleep reduced (decreased need for sleep without feeling tired), and Talkativeness (pressured speech). DSM-5 requires three or more of these associated symptoms (four if mood is only irritable rather than elevated). These features distinguish mania from ordinary happiness or excitement: the patient's mood is typically not congruent with their circumstances, the energy is frenzied rather than purposeful, and the judgement is impaired.
It is essential to recognise that grandiosity in mania can reach delusional intensity — the patient may believe they have a special mission from God, that they possess extraordinary powers, or that they are a famous or important person. When delusions or hallucinations are present alongside a manic episode, the diagnosis is manic episode with psychotic features — a more severe presentation requiring antipsychotic augmentation in addition to mood stabilisation.
The functional consequence of a manic episode is significant and almost always negative, despite the patient's subjective sense of well-being. Reckless behaviour during mania — impulsive spending, sexual disinhibition, aggressive confrontations, substance use — can have devastating consequences for finances, relationships, occupation, and physical safety. Importantly, the patient typically lacks insight into the pathological nature of their experience, making voluntary engagement with treatment difficult.
Hypomania is a milder, time-limited variant of elevated mood with the same qualitative features as mania but differing on two dimensions: the duration criterion is at least four days (not one week), and the episode does not cause marked functional impairment or require hospitalisation. Hypomania, by definition, does not include psychotic features. This distinction has major nosological importance: in the DSM-5 framework, recurrent hypomanic episodes alternating with depressive episodes constitute Bipolar II disorder, while full manic episodes define Bipolar I disorder.
SELF-CHECK
A 22-year-old woman presents with 5 days of elevated mood, increased energy, decreased need for sleep, pressured speech, and spending large sums of money online. She has missed work and her husband is worried. She has no prior psychiatric history. What is the minimum additional information you need to distinguish between mania and hypomania?
A. Whether she has delusions or hallucinations, because hypomania always has psychotic features
B. The exact number of DIG FAST symptoms present, because hypomania requires only two
C. Whether the episode has caused marked functional impairment or required hospitalisation, because this determines the manic vs hypomanic distinction
D. The serum lithium level, because only confirmed bipolar disorder can present this way
Reveal Answer
Answer: C. Whether the episode has caused marked functional impairment or required hospitalisation, because this determines the manic vs hypomanic distinction
The manic versus hypomanic distinction rests primarily on the presence of marked functional impairment or the need for hospitalisation (both indicate mania), and on whether psychotic features are present (psychosis = mania, not hypomania). Duration is also relevant (mania ≥1 week, hypomania ≥4 days), but in this case both thresholds are met (5 days ≥4 days). The fact that she has missed work suggests impairment — but the clinical assessment of 'marked' impairment determines the distinction. Hypomania does not have psychotic features (not 'always has'). The number of DIG FAST symptoms does not distinguish the two. Serum lithium is irrelevant at diagnosis.
Psychopathology and Aetiology of Mania and Bipolar Disorder
Understanding mania requires understanding bipolar disorder as a whole — a recurrent, episodic illness in which the brain cycles between states of mood elevation (mania/hypomania) and depression, with inter-episode periods of relative euthymia (normal mood). The aetiology, like that of depression, is best approached through the biopsychosocial model, but with a stronger biological weighting than unipolar depression.
From a biological perspective, bipolar disorder is among the most heritable of psychiatric conditions, with heritability estimates of 60–80% from twin studies. First-degree relatives of people with bipolar disorder have a 10-fold increased risk compared to the general population. Candidate genes implicated include those involved in monoamine neurotransmission, circadian rhythm regulation (the CLOCK gene), and intracellular second-messenger pathways. At the neurobiological level, mania is associated with hyperactivity of the mesolimbic dopaminergic pathway — explaining the euphoria, reward-seeking, and goal-directed hyperactivity. Norepinephrine excess contributes to the hyperarousal and reduced need for sleep. The circadian disruption in bipolar disorder is a prominent feature: sleep disturbance is not merely a symptom but a trigger — sleep deprivation can precipitate a manic episode in a susceptible individual.
Medical and pharmacological precipitants of mania deserve special attention in primary care, because the first-contact physician may inadvertently cause or worsen mania through prescribing decisions. Antidepressant monotherapy — particularly in a patient with unrecognised bipolar disorder — is a well-documented precipitant of antidepressant-induced mania or cycling acceleration. Corticosteroids, thyroid hormones, stimulants, alcohol (via withdrawal), and recreational drugs (cocaine, amphetamines, cannabis) can all trigger or worsen manic states. An episode of mania following corticosteroid therapy in a patient with known asthma, for example, should not be reflexively attributed to bipolar disorder without excluding the drug as a cause.
Psychological triggers, while less powerful than in unipolar depression, include disrupted sleep schedules, significant life events (both negative and positive), and irregular daily routines that destabilise biological rhythms. Social factors include poor treatment adherence, lack of social support, and high expressed emotion in the family environment, which is associated with higher relapse rates in both mania and depression.
The concept of episode sensitisation (analogous to kindling in depression) applies to bipolar disorder as well: with each successive episode, the threshold for triggering the next episode lowers, episodes may become more frequent, and inter-episode recovery becomes less complete. This is one of the key arguments for long-term prophylactic mood stabiliser therapy — the goal of which is not merely to treat episodes but to prevent their occurrence altogether.
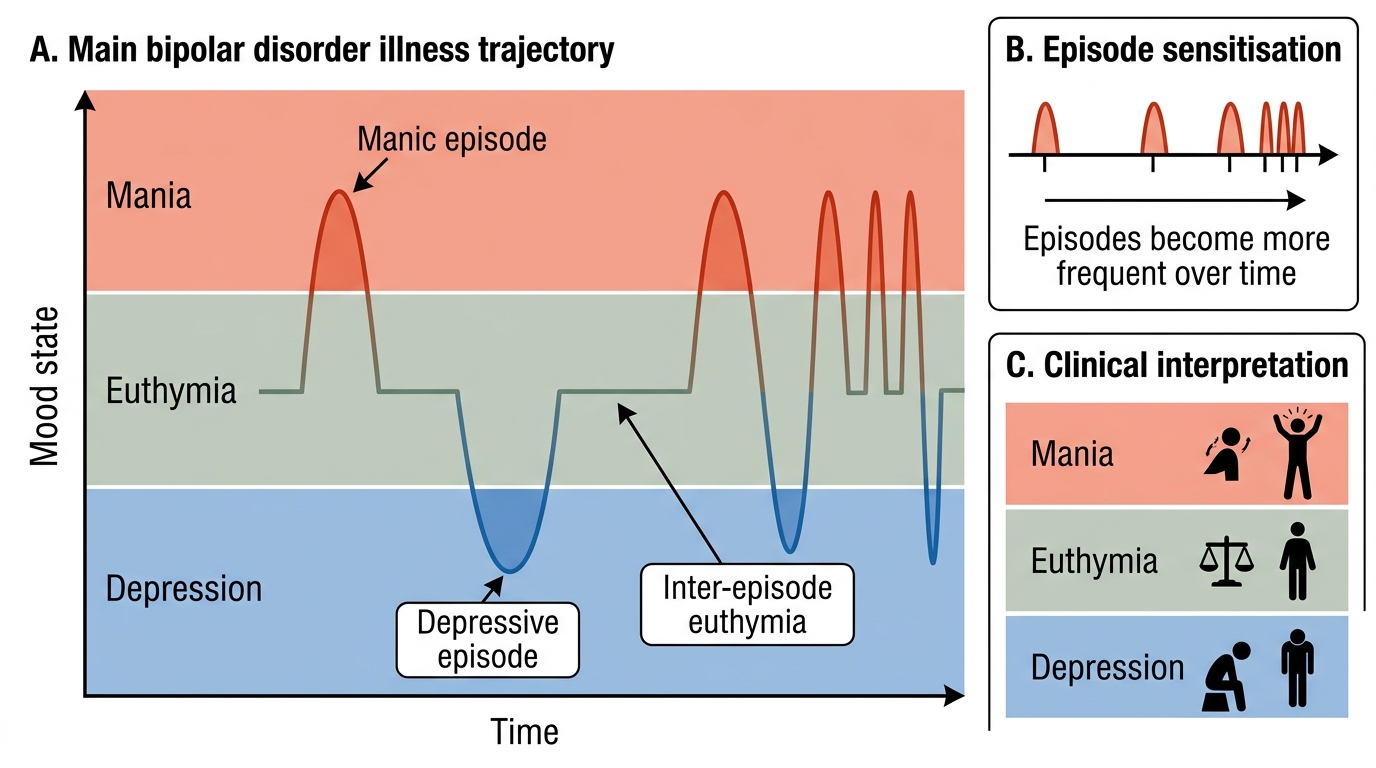
Bipolar Disorder Illness Trajectory
Diagnosis and Mental Status Examination in Mania
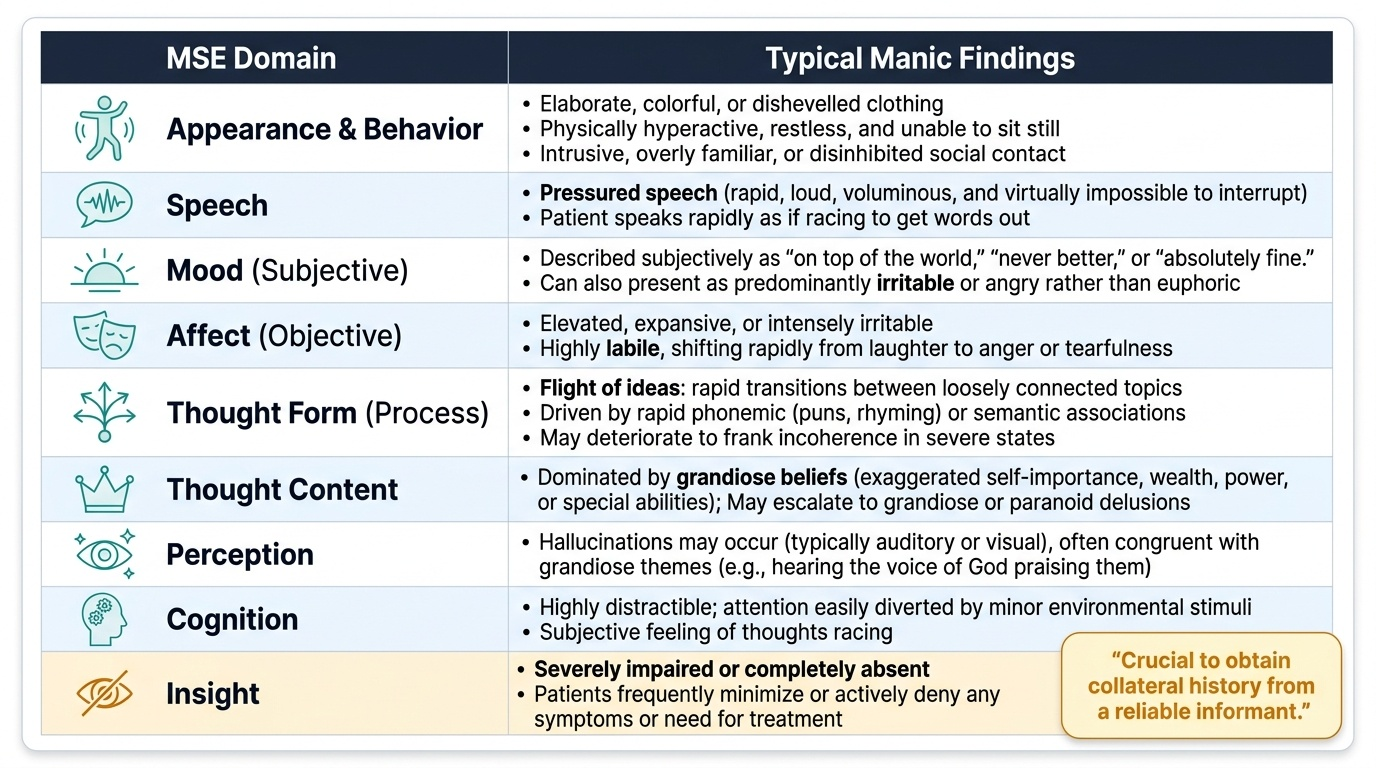
The diagnosis of a manic episode is clinical, based on a careful history and mental status examination. As in depression, there is no confirmatory biomarker. The history should cover the onset and duration of the current episode, the pattern of previous mood episodes (both depressive and elevated), family history of bipolar disorder, current medications (with specific focus on antidepressants, steroids, stimulants), and substance use. Critically, you need collateral history from a reliable informant — the patient in the throes of mania frequently lacks insight and may minimise or actively deny symptoms.
Provided image
The mental status examination in mania presents a distinctive and often immediately recognisable picture. Appearance and behaviour: the patient is often dishevelled or elaborately dressed, physically hyperactive, and unable to sit still. They may make intrusive, overly familiar contact with the examiner. Speech is classically pressured — rapid, loud, voluminous, and difficult to interrupt, with the patient speaking as if racing to get words out. Mood subjectively is described as 'on top of the world,' 'never better,' or 'absolutely fine,' though some manic patients present with a predominantly irritable rather than euphoric mood. Affect is elevated and expansive, or irritable and labile. Thought form shows flight of ideas — rapid transitions between loosely connected topics, driven by phonemic or semantic associations, often with puns and rhymes. In severe mania, this may deteriorate to frank incoherence. Thought content is dominated by grandiose themes — special powers, divine missions, extraordinary talent or wealth. Perceptions: mood-congruent hallucinations (e.g. hearing the voice of God confirming the grandiose belief) may be present in mania with psychotic features. Cognition: attention and concentration are severely impaired by distractibility, though formal cognitive functions are not globally lost. Insight is typically absent or severely impaired — this is one of the most clinically important features because it directly impairs treatment engagement and informed consent.
Assessing for suicide risk in mania is mandatory and non-trivial. Although the subjective mood is elevated, manic patients are at significant risk of harm — through reckless behaviour (road traffic accidents, financial catastrophe, risky sexual encounters) and through the depressive phase that often follows a manic episode. During mixed affective states — in which manic and depressive features co-occur — suicide risk is particularly high.
Organics to exclude: thyroid disease (hyperthyroidism can mimic or precipitate mania), substance intoxication (cocaine, amphetamines, cannabis), corticosteroid use, and neurological conditions (frontotemporal dementia, right temporal lobe tumour, post-stroke mania, HIV CNS involvement). A basic metabolic panel, TSH, urine toxicology, and — where clinically indicated — neuroimaging form the initial exclusion workup for a first presentation of mania.
SELF-CHECK
A 29-year-old man with known bipolar I disorder is brought in during what his family describes as a manic episode. On MSE he has pressured speech, flight of ideas, grandiose delusions about being a prophet, and he denies any illness. Which MSE finding most directly explains why gaining his consent to treatment is particularly challenging?
A. Pressured speech — because the patient cannot listen long enough to receive information
B. Absent insight — because the patient does not believe he is ill and therefore sees no reason for treatment
C. Grandiose delusions — because the patient believes he is too important to need treatment
D. Flight of ideas — because the patient cannot process information in a linear sequence
Reveal Answer
Answer: B. Absent insight — because the patient does not believe he is ill and therefore sees no reason for treatment
Absent insight — the patient's lack of recognition that he is experiencing a psychiatric illness — is the primary MSE finding that impairs voluntary engagement with treatment in mania. Without insight, the patient has no subjective reason to accept medication or hospitalisation. Pressured speech, flight of ideas, and grandiose delusions all contribute to the clinical picture, but absent insight is the most direct barrier to the consent process. Under the Mental Healthcare Act 2017, provisions for emergency assessment and treatment without consent may apply when insight is absent and risk is high.