Page 1 of 9
PS3.1 | Psychoactive Substance Use Disorders — SDL Guide
Learning Objectives
- Identify the clinical features of intoxication and withdrawal for alcohol, nicotine/tobacco, cannabis, and opioids in the Indian context.
- Distinguish ICD-11 harmful use from substance dependence using the three defining criteria.
- Describe the emergency timeline of alcohol withdrawal, including delirium tremens, and explain the rationale for thiamine before glucose.
- Outline the pharmacological and brief-intervention management of common substance use disorders encountered in primary care.
INSTRUCTIONS
Substance use disorders are among the most prevalent psychiatric conditions in India, with alcohol and tobacco carrying the highest disease burden. As a future clinician you will encounter patients at every stage — from early harmful use through established dependence — in primary care clinics, emergency departments, and general wards. Skill in recognising these disorders, managing withdrawal safely, and initiating evidence-based treatment is an essential competency for the Indian Medical Graduate.
References
- Ahuja N. A Short Textbook of Psychiatry, 8th edition. Jaypee, 2022 — Chapters 15–16 (textbook)
- Kaplan & Sadock's Synopsis of Psychiatry, 11th edition — Chapter 20 (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 45-year-old male agricultural labourer is brought to the emergency department by his family. He is tremulous, sweating profusely, and agitated. He had his last drink 30 hours ago. His family reports he drinks at least 500 mL of country liquor daily and becomes 'dangerous' when he stops. Within the hour he has a generalised tonic-clonic seizure. How do you manage him — and what are you afraid might happen in the next 48 hours? This case opens one of the most clinically urgent chapters in psychiatry.
WHY THIS MATTERS
India has the third-highest burden of alcohol use disorders globally, with over 57 million people affected. Tobacco — including smokeless forms such as gutka, khaini, and zarda — kills more than 1 million Indians annually. Opioid dependence, particularly to pharmaceutical codeine cough syrups and heroin in certain states, is rising. Cannabis ('ganja') remains widely used. As an Indian Medical Graduate, you are the first point of contact for patients in withdrawal, for smokers seeking cessation help, and for families dealing with a dependent relative. The NMC competency PS3.1 requires you to both identify and manage these disorders. Missing an alcohol withdrawal emergency can be fatal; missing an opportunity for brief advice in a tobacco user costs life-years.
RECALL
Before we begin, revisit concepts from your earlier studies. From Pharmacology (PH), recall that tolerance develops when repeated exposure to a drug produces diminishing effect, requiring higher doses for the same response — a key neuroadaptive process. From Physiology (PY), recall the role of GABA (inhibitory) and glutamate (excitatory) in synaptic transmission, because alcohol's effects on these systems explain both its intoxication effects and the hyperexcitability seen in withdrawal. From Biochemistry (BI), recall that thiamine (vitamin B1) is an essential cofactor for pyruvate dehydrogenase and transketolase in glucose metabolism — its depletion in chronic alcohol use underlies the risk of Wernicke encephalopathy. These foundations will anchor everything that follows.
Substance Classification and Prevalence in India
Psychoactive substances are chemical agents that alter mood, cognition, perception, or behaviour by acting on the central nervous system. Understanding their classification is necessary before describing clinical presentations, because each class produces a characteristic syndrome of intoxication and a predictable withdrawal pattern. The major classes encountered in the Indian context can be organised by their primary pharmacological action on the CNS.

Provided image
CNS Depressants include alcohol (ethanol), sedative-hypnotic benzodiazepines, and opioids. These agents share the property of CNS depression; withdrawal from all of them produces a rebound hyperexcitable state, though of varying clinical severity. Alcohol is by far the most prevalent depressant substance in India, with harmful use concentrated among men aged 25–55 in both urban and rural settings. CNS Stimulants include amphetamines and cocaine; while globally significant, these are less prevalent than alcohol or opioids in most Indian regions. Nicotine, delivered through smoked tobacco (bidis, cigarettes) and smokeless tobacco (gutka, khaini, zarda, pan masala), is the most widely consumed psychoactive substance in India, affecting over 260 million users. Smokeless tobacco use is particularly prevalent in rural and lower-income populations and is uniquely linked to oral cancers. Cannabis (ganja/charas) is consumed by approximately 3.1% of the Indian population, often co-used with tobacco. Opioids — including heroin, opium, and pharmaceutical codeine preparations — are the third most commonly misused class; opioid dependence is especially prevalent in the north-western states (Punjab, Haryana) and the north-eastern corridor.
Hallucinogens (LSD, psilocybin) and solvents/inhalants (correction fluid, petrol sniffing — seen in street children and adolescents) complete the spectrum. An accurate substance history specifying the substance, route, daily amount, duration of use, and any prior withdrawal episodes is the clinical starting point for all these presentations.
Clinical Presentation of Intoxication
The clinical presentation of a patient using a psychoactive substance depends on whether they are acutely intoxicated (substance present and active) or in withdrawal (substance removed, neuroadaptation unmasked). Distinguishing these states is essential for safe management and requires a careful history, collateral information, and a targeted examination.
Provided image
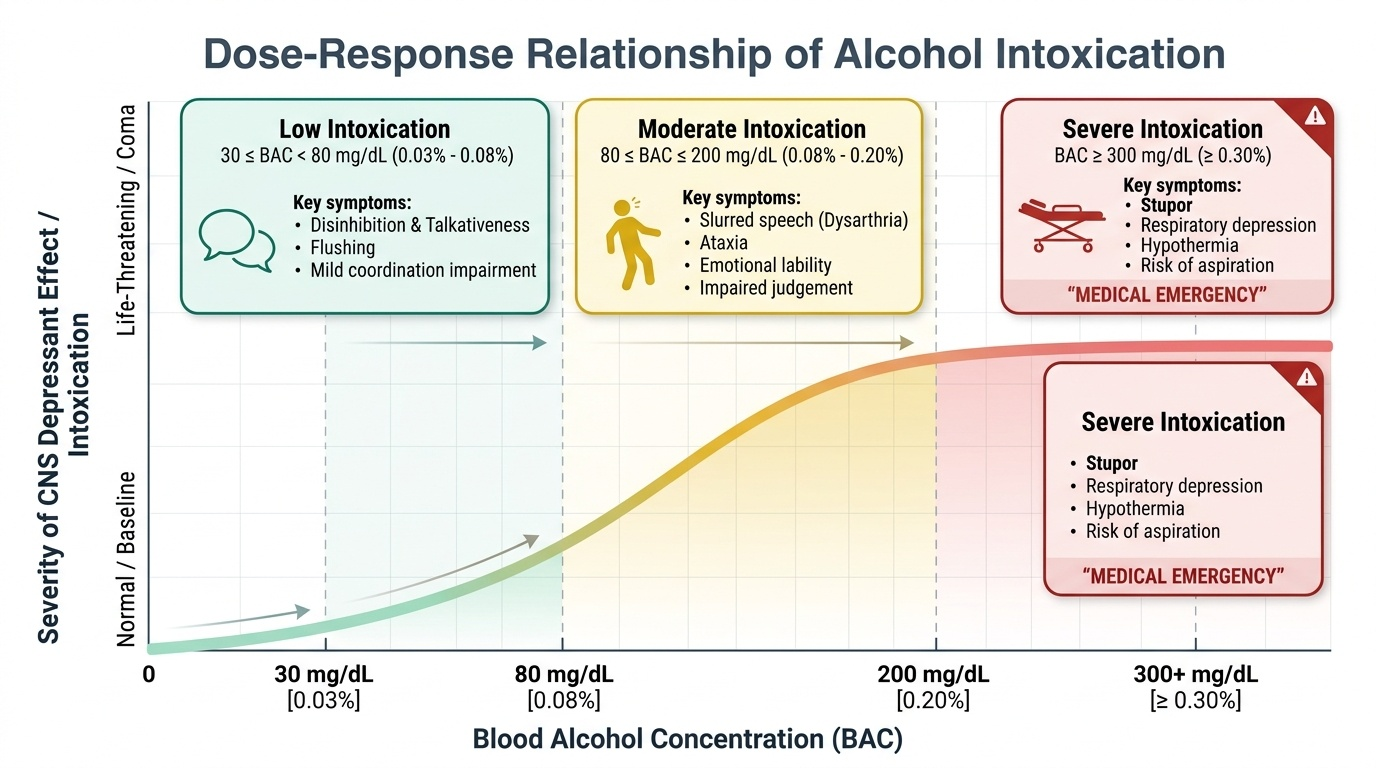
Alcohol intoxication is dose-dependent. At low blood alcohol levels (BAC ~30–80 mg/dL), the patient shows disinhibition, talkativeness, flushing, and mild coordination impairment. At moderate levels (80–200 mg/dL), slurred speech (dysarthria), ataxia, emotional lability, and impaired judgement become apparent. Severe intoxication (>300 mg/dL) produces stupor, respiratory depression, hypothermia, and risk of aspiration — a medical emergency. Idiosyncratic alcohol intoxication (pathological intoxication) describes disproportionate aggression and confusion after small amounts; it is uncommon but medico-legally important.
Nicotine/tobacco intoxication is rarely the presenting complaint in clinical settings. Acute nicotine toxicity — seen with massive dose (e.g., nicotine patches plus smoking, or insecticide poisoning) — causes nausea, vomiting, diarrhoea, bradycardia, hypersalivation, tremors, and in severe cases convulsions and respiratory paralysis via nicotinic receptor desensitisation.
Cannabis intoxication presents within minutes of smoking and includes conjunctival injection (red eyes), dry mouth, tachycardia, increased appetite, impaired short-term memory, and a perceptual distortion ranging from mild euphoria to frank psychosis (cannabis-induced psychotic disorder). Acute cannabis-induced psychosis is an increasing clinical problem in India given high-potency cannabis availability.
Opioid intoxication produces the classic triad: miosis (pinpoint pupils), respiratory depression, and reduced consciousness. Skin is warm, face flushed. In heroin overdose, respiratory rate may fall below 8 breaths/minute — a life-threatening emergency treatable with naloxone 0.4–2 mg IV/IM (repeat every 2–3 minutes, short duration of action requires monitoring and repeat dosing).
Alcohol Withdrawal: The Emergency Timeline
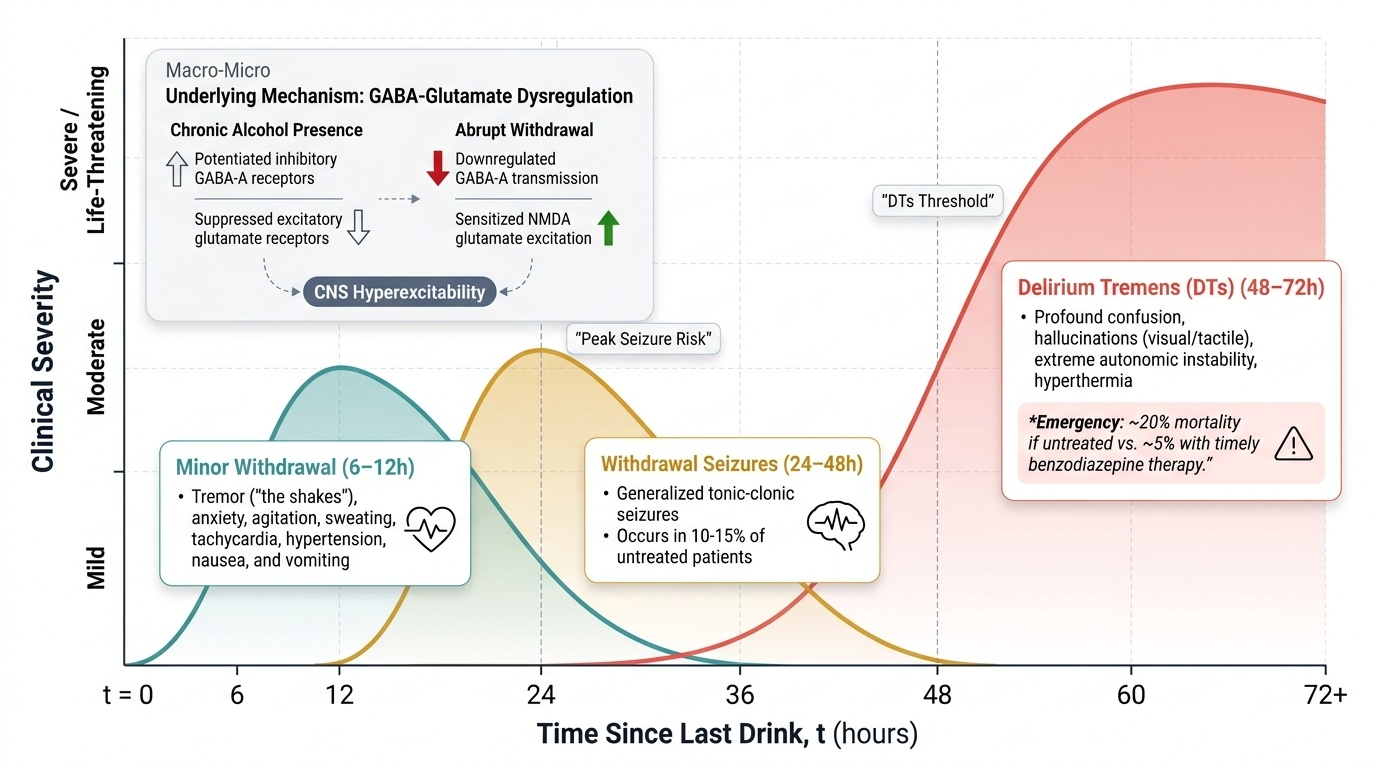
Alcohol withdrawal is the most medically dangerous withdrawal syndrome encountered in clinical practice and produces a predictable, time-stamped sequence of signs over a 72-hour window after the last drink. Every clinician — regardless of specialty — must know this timeline because severity escalates rapidly and mortality from untreated delirium tremens approaches 20% without treatment, compared with approximately 5% with timely, adequate benzodiazepine therapy. The mechanism is GABA-glutamate dysregulation: chronic alcohol potentiates inhibitory GABA-A receptors and suppresses excitatory glutamate (NMDA) receptors; upon abrupt removal of alcohol, the brain is left with profoundly downregulated GABA inhibition and upregulated, sensitised glutamate-driven excitation, producing the clinical state of CNS hyperexcitability that manifests as tremor, seizures, and ultimately delirium. This is not metaphor — it is pharmacophysiology, and it predicts the clinical course precisely enough to guide treatment timing. Understanding the phases also helps you counsel patients: the patient who says 'I just stopped — I feel fine' at 8 hours may be in serious danger at 48 hours.
Provided image
The withdrawal timeline unfolds in three overlapping phases:
- Minor withdrawal (6–12 hours after last drink): The earliest symptoms are anxiety, agitation, tremulousness ("shakes"), sweating, tachycardia, hypertension, nausea, and vomiting. These are predominantly autonomic. The patient remains alert and oriented. This phase persists and intensifies through the next several hours.
- Withdrawal seizures (24–48 hours, peak ~24 hours): Generalised tonic-clonic seizures occur in approximately 10–15% of untreated patients. Importantly, these are typically brief, self-limited, and few in number — prolonged or recurrent seizures suggest another aetiology (e.g., subdural haematoma, which must be excluded in falls-prone alcohol-dependent patients). Hallucinosis (tactile, visual, or auditory hallucinations with clear consciousness) may begin in this phase — distinct from delirium tremens.
- Delirium Tremens (48–72 hours, peak at 72 hours): The most severe manifestation, characterised by delirium (fluctuating consciousness, disorientation, agitation) plus autonomic storm (fever, tachycardia, hypertension, profuse sweating) plus vivid hallucinations (classically visual — animals, insects — the 'pink elephants' of folk memory). Delirium tremens is a medical emergency with mortality of up to 5% (with treatment) and up to 20% if untreated, from hyperthermia, cardiovascular collapse, and aspiration.
Not every patient who stops drinking will progress to delirium tremens; risk factors include prior history of delirium tremens, concurrent illness, prolonged heavy use, and older age. Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) is a validated 10-item scale that quantifies withdrawal severity and guides dosing decisions.
SELF-CHECK
A patient with alcohol dependence had his last drink 30 hours ago. He is now confused, agitated, febrile (38.8°C), tachycardic, and reporting that he can see insects crawling on the wall. What is the most likely diagnosis?
A. Alcohol hallucinosis (clear consciousness, auditory hallucinations only)
B. Delirium tremens (delirium + autonomic storm + hallucinations, 48–72 h window)
C. Minor alcohol withdrawal (anxiety, tremor, sweating at 6–12 h)
D. Wernicke encephalopathy (ophthalmoplegia, ataxia, confusion)
Reveal Answer
Answer: B. Delirium tremens (delirium + autonomic storm + hallucinations, 48–72 h window)
Delirium tremens is the correct answer. It typically peaks at 48–72 hours after the last drink (this patient is at 30 hours, early but possible). The triad of delirium (fluctuating consciousness, disorientation, agitation), autonomic storm (fever, tachycardia), and hallucinations (classically visual) defines DTs. Alcohol hallucinosis occurs with clear consciousness and is predominantly auditory. Minor withdrawal occurs at 6–12 hours and lacks delirium. Wernicke encephalopathy has a classic triad of ophthalmoplegia, ataxia, and confusion — a separate entity requiring thiamine urgently.