Page 1 of 12
PS9.1 | Common Psychosexual Disorders — SDL Guide
Learning Objectives
- Classify psychosexual disorders by phase of the sexual response cycle using ICD-11 framing
- Differentiate organic from psychogenic aetiologies of common sexual dysfunctions
- Describe the clinical features of erectile dysfunction, premature ejaculation, hypoactive sexual desire disorder, vaginismus, and dyspareunia
- Outline the diagnostic approach, including mental status considerations, for psychosexual disorders
- Apply the PLISSIT model to frame counselling and management of psychosexual disorders
INSTRUCTIONS
Sexual health is an integral dimension of human wellbeing and an important domain of clinical psychiatry. Psychosexual disorders are common, underdiagnosed, and carry significant psychological burden. This module equips you with the clinical framework to recognise, assess, and sensitively manage the most frequently encountered sexual dysfunctions. A non-judgemental, patient-centred approach is foundational to every consultation in this domain.
References
- Ahuja N. A Short Textbook of Psychiatry, 8th ed. Jaypee Brothers; 2022. Chapter 15. (textbook)
- Kaplan HI, Sadock BJ. Synopsis of Psychiatry, 11th ed. Wolters Kluwer; 2015. Chapter 20. (textbook)
- ICD-11 for Mortality and Morbidity Statistics. World Health Organization; 2022. Chapter 17 (Conditions related to sexual health). (guideline)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 38-year-old married man presents to your outpatient psychiatric clinic accompanied by his wife. He whispers to you before she enters: 'I have not been able to perform for six months. My marriage is breaking.' You notice his distress and embarrassment. He has been avoiding bedtime, has stopped socialising, and scores 8/25 on the International Index of Erectile Function (IIEF). His wife confides that she has also lost interest in intimacy and feels frustrated and guilty. How do you approach this consultation with sensitivity, clinical rigour, and therapeutic intent? By the end of this module, you will have the tools to do exactly that.
WHY THIS MATTERS
Psychosexual disorders affect an estimated 30–40% of adults at some point in their lives, yet most patients never disclose these problems to a clinician. In Indian clinical settings, shame, cultural silence, and fear of stigma are powerful barriers. As a psychiatrist, you will encounter these concerns embedded in presentations of depression, marital conflict, infertility workup, and relationship crises. Competency PS9.1 requires you to describe common psychosexual disorders — this is not merely academic; early, sensitive clinical recognition prevents diagnostic delay, reduces psychological suffering, and preserves relationships. The PLISSIT model you will learn here is a practical tool applicable in any brief outpatient encounter.
RECALL
Before we begin, let us draw on what you already know:
- Sexual response cycle (Masters and Johnson, Kaplan's triphasic model): Desire → Arousal → Orgasm → Resolution. Kaplan later added the desire phase as a distinct entity preceding physiological arousal.
- Neurotransmitters relevant to sexual function: dopamine facilitates desire and arousal; serotonin inhibits orgasm (hence SSRIs → delayed ejaculation/anorgasmia); nitric oxide (NO) mediates penile smooth muscle relaxation and erection.
- Endocrine axes: testosterone is the principal driver of libido in both males and females; oestrogen modulates vaginal lubrication and clitoral engorgement; prolactin excess (hyperprolactinaemia) suppresses desire via inhibition of GnRH.
- Autonomic control: erection is parasympathetic ('point' = parasympathetic); ejaculation is sympathetic ('shoot' = sympathetic).
- Mental Healthcare Act 2017: replaces the Mental Health Act 1987; prohibits discrimination; affirms dignity of persons with mental illness.
Classification of Psychosexual Disorders by Phase
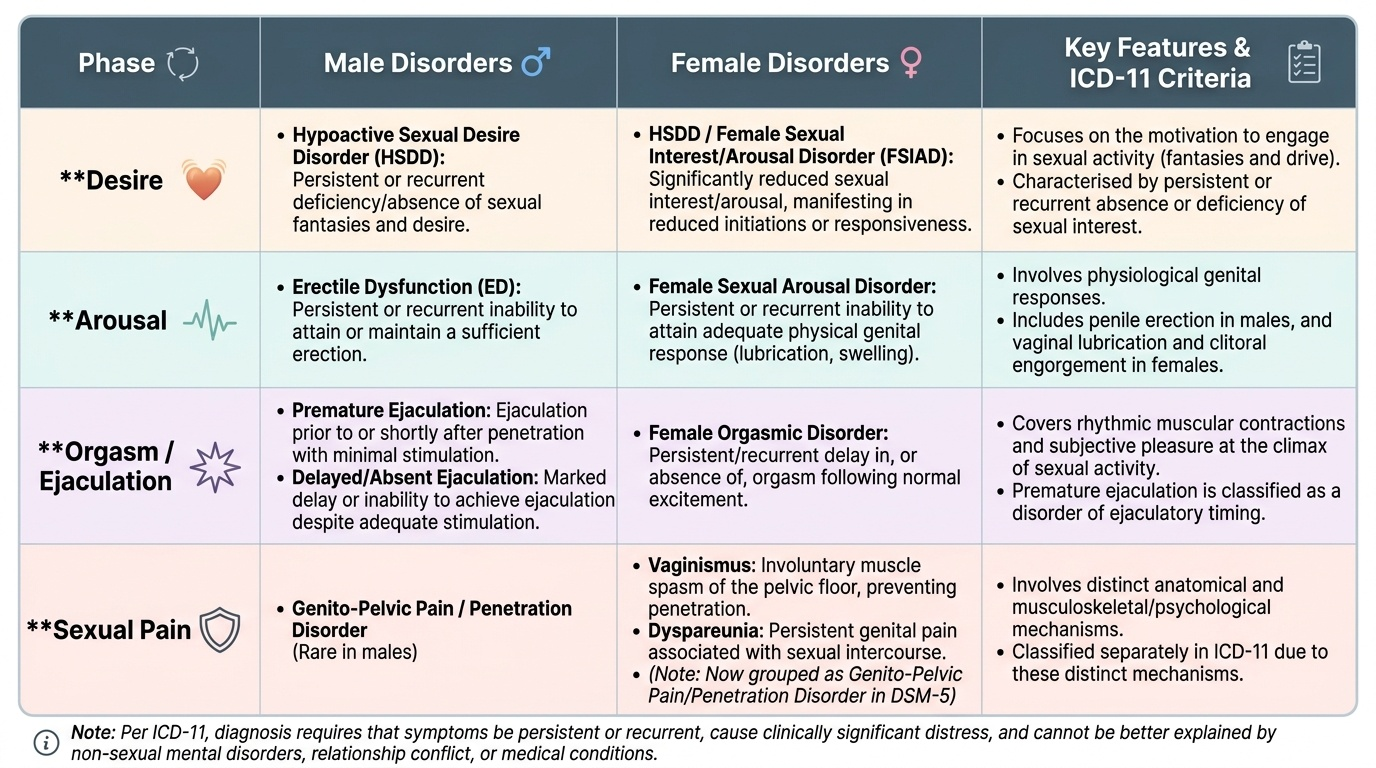
Sexual dysfunctions are best understood by locating them within the sexual response cycle. The ICD-11 (Chapter 17 — Conditions Related to Sexual Health) classifies sexual dysfunctions according to the phase they primarily disrupt: desire, arousal, orgasm, or sexual pain. This phase-based framing guides both diagnosis and management, because different phases have distinct neurobiological substrates, aetiologies, and treatment targets.
Provided image
The desire phase encompasses sexual interest — the motivation to engage in sexual activity, including fantasies and drive. Disorders here are characterised by persistent or recurrent absence or deficiency of sexual interest. The arousal phase involves physiological genital response: penile erection in males and vaginal lubrication and clitoral engorgement in females. Disorders at this stage include erectile dysfunction in males and female sexual arousal disorder. The orgasm phase covers the rhythmic muscular contractions and subjective pleasure at the climax of sexual activity. Orgasmic disorders include delayed/absent orgasm and, in males, premature ejaculation (which is classified here as a disorder of ejaculatory timing rather than a separate phase). Sexual pain disorders — vaginismus and dyspareunia — are classified separately in ICD-11 as they involve a distinct anatomical and musculoskeletal/psychological mechanism.
For clinical purposes, ICD-11 requires that the disturbance be persistent or recurrent (not situational or transient), cause clinically significant distress to the individual, and not be better explained by a non-sexual mental disorder, relationship distress, or another medical condition.
| Phase | Male Disorders | Female Disorders |
|---|---|---|
| Desire | Hypoactive sexual desire disorder (HSDD) | HSDD / Female sexual interest–arousal disorder |
| Arousal | Erectile dysfunction | Female sexual arousal disorder |
| Orgasm / Ejaculation | Premature ejaculation; delayed/absent ejaculation | Female orgasmic disorder |
| Sexual pain | Genito-pelvic pain / penetration disorder (male, rare) | Vaginismus; Dyspareunia (now Genito-pelvic pain/penetration disorder in DSM-5) |
Common Psychosexual Disorders — Clinical Presentation
The five disorders most commonly encountered in clinical psychiatry are erectile dysfunction (ED), premature ejaculation (PE), hypoactive sexual desire disorder (HSDD), vaginismus, and dyspareunia. Each has a distinct clinical signature that should prompt systematic enquiry.
Erectile dysfunction is defined as persistent inability to attain or maintain a penile erection sufficient for satisfactory sexual activity. The ICD-11 criterion requires the difficulty to be present on most or all sexual occasions over at least several months. ED affects an estimated 10–20% of men in community surveys, with prevalence rising steeply with age (over 50% in men >70 years). The clinical presentation often includes avoidance of intimacy, diminished self-esteem, partner distress, and anxiety about future performance. The clinician should distinguish total (never achieves erection) from selective (achieves with some partners/situations/on waking) loss to guide organic-vs-psychogenic differentiation.
Premature ejaculation is characterised by ejaculation occurring persistently before or within approximately one minute of vaginal penetration, on almost all occasions, and accompanied by significant distress. The International Society of Sexual Medicine (ISSM) defines lifelong PE (primary: present since first sexual experience) versus acquired PE (secondary: develops after a period of normal ejaculatory control). DSM-5 uses a threshold of approximately one minute; ICD-11 uses 'too quickly for both partners to enjoy the interaction.' Ejaculatory latency time (IELT) <1 minute is a commonly applied cut-off in research and clinical practice.
Hypoactive sexual desire disorder is the most prevalent sexual dysfunction in women and is increasingly recognised in men. It presents as persistent or recurrent absence of sexual fantasies and desire for sexual activity, causing marked distress. In women, DSM-5 merges HSDD with female arousal disorder as 'Female Sexual Interest/Arousal Disorder (FSIAD)' — ICD-11 retains them as distinct categories based on the dominant complaint. HSDD in men may present as loss of interest in sex, avoidance of intimacy, and loss of spontaneous erections.
Vaginismus is the involuntary contraction of the perivaginal muscles (primarily levator ani) that makes vaginal penetration difficult, painful, or impossible. Primary vaginismus (never achieved penetration) is common in newly married women in cultures where sexual debut is within marriage. Secondary vaginismus (onset after a period of successful intercourse) may follow trauma, surgery, or infection. ICD-11 combines vaginismus and dyspareunia as genito-pelvic pain/penetration disorder in DSM-5, reflecting their frequent co-occurrence.
Dyspareunia is recurrent genital pain during intercourse, affecting women more than men. It may be superficial (entry pain — often musculoskeletal or vaginal) or deep (pelvic — often secondary to endometriosis, PID, or structural pathology). Psychological perpetuating factors (anticipatory anxiety, muscle guarding, avoidance) maintain the disorder even after the primary cause is treated.
SELF-CHECK
A 30-year-old woman presents with inability to permit vaginal penetration on all attempts since marriage six months ago. She is distressed and her husband is supportive. Which of the following correctly describes her condition?
A. Secondary vaginismus due to psychological trauma
B. Primary vaginismus — involuntary perivaginal muscle contraction preventing penetration, present since first attempt
C. Female sexual arousal disorder
D. Hypoactive sexual desire disorder
Reveal Answer
Answer: B. Primary vaginismus — involuntary perivaginal muscle contraction preventing penetration, present since first attempt
Primary vaginismus is defined as involuntary, recurrent contraction of the perivaginal (levator ani) muscles causing penetration to be difficult, painful, or impossible, present from the first attempt at intercourse. Secondary vaginismus develops after a period of successful penetration. Arousal disorder and HSDD involve desire and lubrication, not muscle contraction preventing penetration.
Psychopathology and Aetiology — Organic versus Psychogenic
Differentiating organic from psychogenic causes is one of the most clinically important tasks in evaluating psychosexual disorders, because it directs the treatment strategy. In practice, most cases — particularly ED and HSDD — have a mixed aetiology, with organic factors lowering the threshold and psychological factors maintaining or amplifying the dysfunction. The astute clinician holds both simultaneously rather than defaulting to either extreme.
For erectile dysfunction, the classic differentiator is the nocturnal penile tumescence (NPT) test: men with psychogenic ED typically have preserved nocturnal erections (REM sleep-associated, autonomically mediated), whereas organic ED shows absent or reduced NPT. A practical proxy is the presence of morning erections or erections with masturbation despite failure with a partner — suggesting psychogenic causation. Organic causes include vascular disease (the commonest — atherosclerosis of the internal pudendal artery), diabetes mellitus (neuropathy + vasculopathy), hypogonadism, hyperprolactinaemia, medications (antihypertensives — particularly beta-blockers, thiazides; antipsychotics; SSRIs; finasteride), pelvic surgery, and smoking.
Psychological precipitants and perpetuants include performance anxiety (the most potent psychogenic driver — 'spectatoring': the man observes his own performance rather than engaging, breaking the natural erection reflex), depression (anhedonia, reduced libido, fatigue), relationship conflict, past traumatic sexual experiences, and religious/cultural guilt. These factors cause and maintain the anxiety-erection failure cycle: failed erection → anxiety → sympathetic arousal → detumescence → confirmed failure → intensified anxiety.
For HSDD, hormonal causes (low testosterone in men, postmenopausal oestrogen decline in women) are common organic factors. Medications — especially SSRIs, antipsychotics (via hyperprolactinaemia), and hormonal contraceptives — are frequently overlooked organic causes. Relationship dissatisfaction, history of abuse, and mood disorders are major psychological aetiologies.
For premature ejaculation, psychogenic factors (anxiety, conditioning, early sexual experiences associated with speed/secrecy) predominate in lifelong PE; acquired PE may reflect prostatitis, hyperthyroidism, or serotonergic imbalance. The neurobiological substrate of lifelong PE may involve 5-HT receptor hypersensitivity — which explains the efficacy of dapoxetine (a short-acting SSRI) as first-line pharmacotherapy.
For vaginismus and dyspareunia, gynaecological/structural causes (infection, endometriosis, inadequate lubrication, post-menopausal atrophy) must be excluded first. Psychological perpetuating factors — fear of pain, anticipatory anxiety, avoidance, partner pressure — are almost universally present and must be addressed concurrently.
| Feature | Psychogenic ED | Organic ED |
|---|---|---|
| Onset | Sudden, situational | Gradual, global |
| Morning erections | Preserved | Absent or reduced |
| With masturbation | Often achievable | Reduced |
| NPT test | Normal | Abnormal |
| Psychological triggers | Present (anxiety, conflict) | Often absent |
| Associated vascular/metabolic risk | Often absent | Usually present |