Page 1 of 8
PS12.1 | Suicide Risk Assessment — SDL Guide
Learning Objectives
- Recognise the clinical and public health importance of suicide risk assessment in the Indian context
- Apply the governing principles of empathic, non-judgmental, structured suicide risk assessment
- Conduct a structured assessment covering suicidal ideation, intent, plan, means/access, past attempts, and protective factors
- Interpret the risk factor profile using the SAD PERSONS framework and stratify risk as low, moderate, or high
- Formulate a safety plan, advise on means restriction, and document the assessment with medico-legal accuracy
- Demonstrate understanding of the Mental Healthcare Act 2017 provisions relevant to attempted suicide
INSTRUCTIONS
Suicide risk assessment is one of the most consequential clinical skills a psychiatrist — or any physician — must master. This self-directed module walks you through the principles, method, and applied practice of structured risk assessment, grounded in Ahuja and Kaplan & Sadock. Complete each section in sequence, attempt the embedded quizzes without reviewing the answers first, and use the self-assessment vignette at the end to consolidate your competence before clinical exposure.
References
- Ahuja N. A Short Textbook of Psychiatry. 8th ed. Jaypee Brothers; 2022. Chapter: Suicide and Parasuicide. (textbook)
- Sadock BJ, Sadock VA, Ruiz P. Kaplan & Sadock's Synopsis of Psychiatry. 11th ed. Wolters Kluwer; 2015. Chapter 32: Suicide. (textbook)
- Mental Healthcare Act 2017. Government of India. Gazette of India, 7 April 2017. Section 115. (legislation)
- National Mental Health Programme, Ministry of Health & Family Welfare, India. Guidelines on Suicide Prevention. 2022. (guideline)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 22-year-old engineering student presents to the emergency department after being found unresponsive by his roommate. He had consumed an unknown quantity of his mother's anxiolytics and left a note apologising to his family. He is now conscious and medically stable. The psychiatry resident on call is asked to see him. Standing at the bedside, she faces the question every clinician eventually confronts: where do I begin, and what exactly am I assessing? This module equips you to answer that question — not just tonight, but for every patient who arrives in that chair across the years of your practice.
WHY THIS MATTERS
Suicide is the second leading cause of death among 15–29-year-olds globally and among the top five causes of death in young Indians. India accounts for approximately 17% of global suicide deaths. Every year in India, nearly 170,000 people die by suicide — roughly one death every three minutes. Yet the majority of people who die by suicide had contact with a healthcare provider in the weeks before their death, which means clinicians have repeated opportunities to intervene. Structured suicide risk assessment is the instrument of that intervention. When done well, it identifies who is at imminent risk, guides the intensity of care, informs safety planning, and may directly prevent a death. When done poorly — or not at all — it creates false reassurance and medico-legal exposure. Competency PS12.1 requires you to perform this assessment; this SDL teaches you how.
RECALL
Before proceeding, recall the following from your prior learning: the biopsychosocial model of psychiatric illness (Year 2, PS1), the principles of psychiatric communication and the mental status examination (PS11), and the mood disorders you have studied — particularly major depressive disorder and bipolar disorder, which carry the highest psychiatric risk for suicide. Also recall your study of substance use disorders, which significantly amplify risk. You do not need to re-read those topics now, but having them mentally available will help you situate each clinical concept in this SDL within a broader understanding of the patient.
Why Suicide Risk Assessment Is a Core Clinical Skill
Suicide risk assessment is not a peripheral psychiatric sub-skill reserved for specialists working in inpatient units. It is a foundational clinical competency that every physician — whether a general practitioner, an emergency medicine physician, or a postgraduate psychiatry trainee — must be able to perform reliably and systematically. The reason is straightforward: suicidal ideation and behaviour cross all specialties and all settings. Patients experiencing suicidal distress present to general OPDs, medical wards, emergency rooms, and community health centres far more often than they present to dedicated psychiatric services. A physician who cannot perform a structured risk assessment when confronted with such a patient is clinically deficient in a way that can directly cost a life.
The epidemiological burden makes this particularly urgent in the Indian context. The National Crime Records Bureau (NCRB) data for 2022 recorded 170,924 suicide deaths in India — a rate of approximately 12.4 per 100,000 population. Young adults (18–30 years) and agricultural communities carry a disproportionate share of this burden. Family problems, illness, and financial difficulties are the three most commonly cited contributing factors in NCRB data. Contrary to the perception that suicide is unpredictable, research consistently shows that the majority of individuals who die by suicide communicated their distress to someone — a family member, a friend, or a healthcare provider — in the days or weeks before death. This window of contact is the clinician's opportunity.
The clinical stakes of assessment extend beyond mortality prevention. Performed correctly, a structured assessment guides immediate management decisions: is this patient safe to discharge, or does she need admission? Does she need 24-hour observation, or is outpatient follow-up with a safety plan sufficient? These decisions require a systematic, documented clinical evaluation — not an intuitive impression. The structured approach also provides medico-legal protection: a documented risk assessment that records what was asked, what was found, and what was decided is a defensible clinical record. An undocumented or unstructured encounter is not.
Finally, suicide risk assessment is an act of compassionate clinical engagement. When a clinician asks directly and without embarrassment about suicidal thoughts, she signals to the patient that his distress is legitimate, that it can be spoken, and that help exists. This signal itself has genuine therapeutic value — it breaks the silence that often isolates patients from the very care that could protect them. For all these reasons — epidemiological, clinical, medico-legal, and therapeutic — the skill you are learning in this module is among the most important you will acquire in psychiatry.
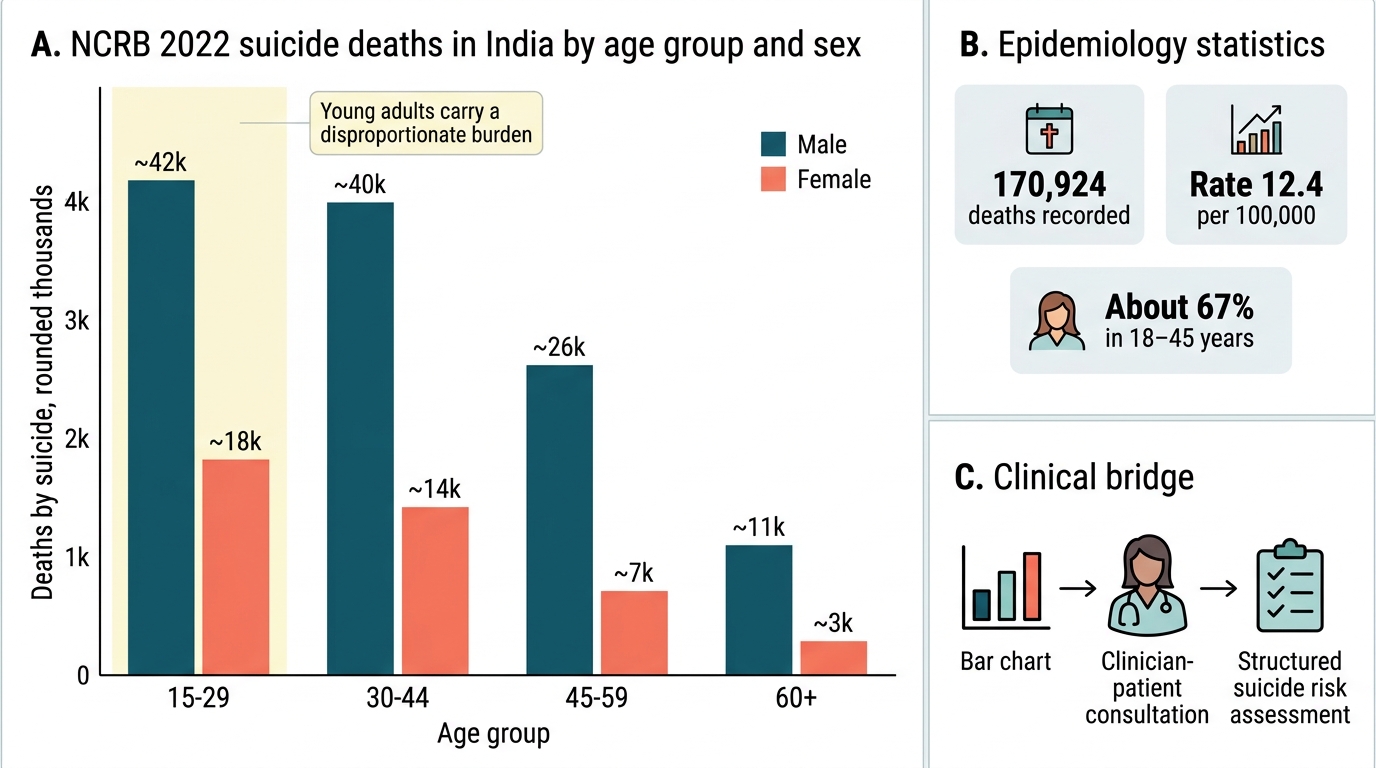
NCRB 2022 Suicide Burden by Age and Sex
SELF-CHECK
Which of the following best describes the burden of suicide deaths in India as recorded by NCRB 2022?
A. Approximately 50,000 deaths per year, rate ~3 per 100,000
B. Approximately 170,000 deaths per year, rate ~12.4 per 100,000
C. Approximately 300,000 deaths per year, rate ~22 per 100,000
D. Approximately 20,000 deaths per year, rate ~1.5 per 100,000
Reveal Answer
Answer: B. Approximately 170,000 deaths per year, rate ~12.4 per 100,000
NCRB 2022 data recorded 170,924 suicide deaths in India, corresponding to a rate of approximately 12.4 per 100,000 population. India accounts for around 17% of global suicide deaths and carries one of the largest national burdens in absolute numbers. This epidemiological reality underscores why every clinician must be able to perform a structured suicide risk assessment.
Governing Principles of Risk Assessment
Several foundational principles must govern every suicide risk assessment you conduct. Understanding these principles is not merely academic — they shape the quality of information you elicit, the safety of the clinical encounter, and the therapeutic relationship you build with a patient who is often deeply ambivalent about both living and disclosing her distress.
The first and most clinically important principle is that asking about suicide does not increase the risk of suicide. This is one of the most persistent and dangerous misconceptions in clinical practice, and it must be dispelled explicitly at the outset. Clinicians sometimes avoid direct inquiry, fearing they will 'plant the idea' in a vulnerable patient's mind. The evidence consistently refutes this: multiple systematic reviews and prospective studies have found no evidence that asking about suicidal ideation increases suicidal ideation, plans, or behaviour. On the contrary, direct, empathic questioning typically relieves distress by allowing the patient to speak about something she has been carrying in silence. If you approach this topic with hesitation or circumlocution, you communicate to the patient that her distress is shameful or unspeakable — and you simultaneously fail to obtain the clinical information you need to protect her.
The second principle is directness combined with empathy. The clinical language for asking about suicide must be clear and unambiguous. Euphemisms such as "have you been having any negative thoughts?" or "are you in a bad place?" are clinically inadequate because they allow the patient to answer without disclosing suicidal content. You must ask, in plain clinical terms: "Are you having thoughts of ending your life?" or "Have you thought about killing yourself?" This directness must be delivered within a framework of empathic warmth — your tone, posture, and pace must communicate that you are asking because you are concerned and want to understand, not because you are filling in a checklist.
The third principle is non-judgmental stance. Suicidal patients often expect condemnation, dismissal, or alarm from clinicians. Any hint of judgment — whether expressed verbally ("why would you do something like that?") or non-verbally (visible shock, hurrying through the interview) — closes the clinical conversation. You must be able to hear accounts of suicidal intent, planning, and prior attempts without expressing moral disapproval or visible distress.
The fourth principle concerns the legal framework in India. Under the Mental Healthcare Act 2017, specifically Section 115, a person who attempts suicide is presumed to be suffering from severe stress and shall not be punished under any law in force. This represents a decisive break from the era when Section 309 of the Indian Penal Code (IPC) was used to criminalise suicide attempt. The predecessor legislation, the Mental Health Act 1987, did not contain this decriminalisation provision. Clinicians must correctly cite the current Act — the Mental Healthcare Act 2017 — and understand its implications: the patient who has attempted suicide is not a criminal; she is a person in acute distress who requires care and rehabilitation. This legal framing should inform how you introduce yourself and how you communicate with both the patient and her family.
The fifth principle is awareness of confidentiality limits. The information shared during a suicide risk assessment is generally protected by clinical confidentiality. However, when the risk assessment reveals imminent danger to the patient's life, the clinician has both an ethical and a legal obligation to act — including informing the family and arranging appropriate care — even if the patient has not explicitly consented. This exception to confidentiality should be explained to the patient at the outset of the assessment, not invoked as a surprise after disclosure.
These five principles collectively create the conditions under which meaningful, accurate, and therapeutically helpful risk assessment is possible.
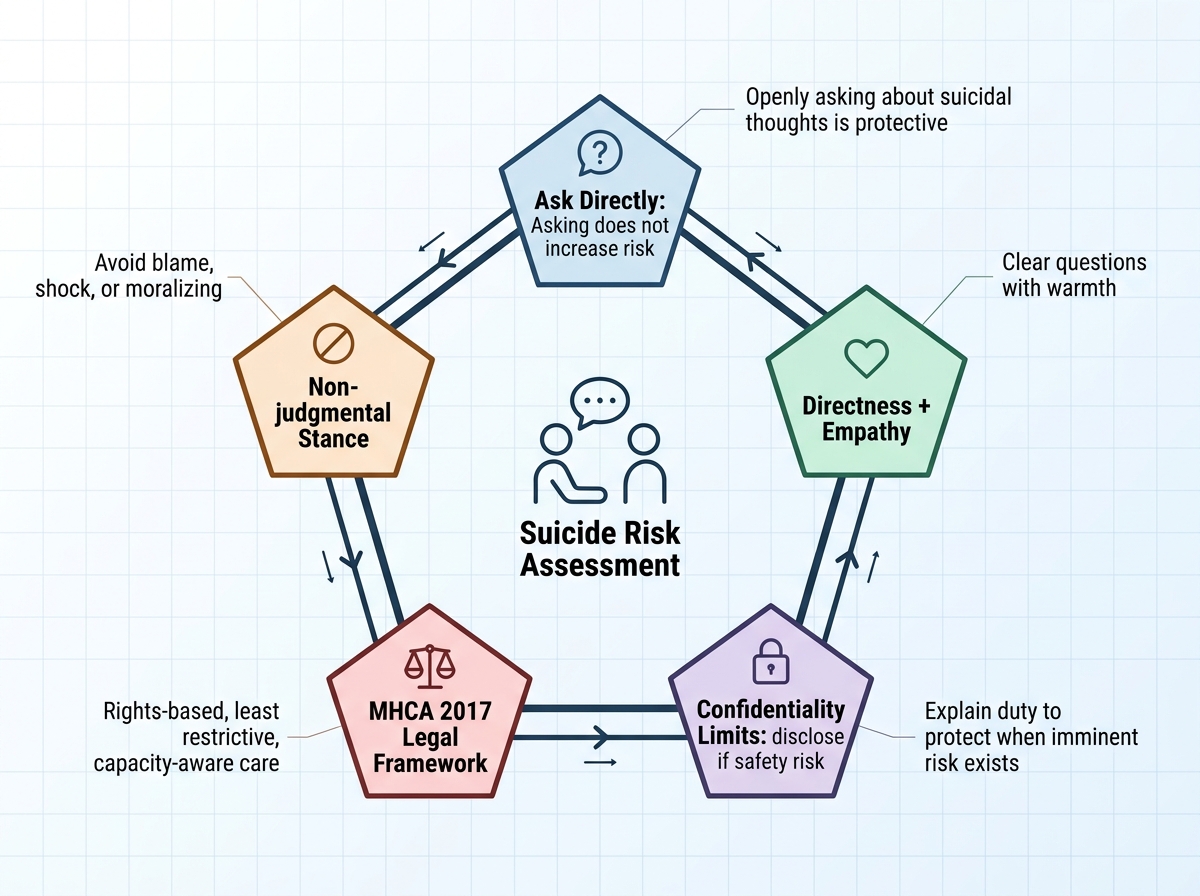
Five Governing Principles of Suicide Risk Assessment
The Structured Assessment Method — Domains and Sequence
A reliable suicide risk assessment follows a structured sequence of clinical inquiry across six interconnected domains. These domains are not a rigid checklist to race through; they are a framework for systematic clinical exploration, each building on the preceding one. The sequence has an internal logic: you begin with the patient's current mental state and thoughts (ideation), then explore the degree of intentionality (intent and plan), then assess the concrete level of danger (means access), then understand the historical risk trajectory (past attempts), and finally identify the factors that may buffer against the risk (protective factors). Together, they create a comprehensive clinical picture.
Suicidal ideation is the starting point. Ideation exists on a spectrum from passive death wishes ("I wish I were dead"; "I wish I wouldn't wake up") to active suicidal ideation (specific thoughts of killing oneself). You must establish: Is the ideation present? How frequent are the thoughts? How intense? How persistent? Passive death wishes without active intent carry lower immediate risk but must not be dismissed — they represent a starting point on a spectrum that can progress. The Columbia Suicide Severity Rating Scale (C-SSRS), a validated structured instrument, provides a useful framework for grading ideation by intensity and persistence, though clinical judgment always complements any structured tool.
Intent refers to the patient's subjective sense of whether she intends to act on her thoughts. A patient may have vivid suicidal imagery but report no intention to act; another may describe fleeting thoughts but express strong intent. Intent is elicited by direct questions: "Do you intend to act on these thoughts?" and "What stops you from acting on them?" The presence of clear intent dramatically shifts the urgency of the assessment.
Plan refers to the degree of forethought and specificity. A vague wish to die differs substantially from a patient who has identified a specific method, a specific time, and a specific place. Ask: "Have you thought about how you would do it?" A specific, detailed plan indicates substantially higher risk than unformed ideation, both because it signals intent and because it signals access to means.
Means access refers to whether the patient has or can readily obtain the means to carry out her plan. A patient who plans to use firearms and has a weapon at home is in a qualitatively different risk category from one whose plan involves means she cannot easily access. Means restriction — limiting access to lethal means — is one of the most evidence-based population-level and individual-level interventions in suicide prevention, and this assessment domain directly informs that intervention.
Past attempts are the single strongest predictor of future suicide. A prior attempt roughly tenfold increases the risk of a completed suicide compared with someone with no prior attempt. You must assess: Has the patient previously attempted suicide? How many times? What method was used? What was the medical severity of the attempt? What precipitated it? Did the patient regret survival? Each of these details refines the current risk picture.
Protective factors are the counterweight to risk factors. They include reasons for living (children, religious beliefs, fear of death or pain, family obligations), social support (relationships, access to care), engagement in treatment, and future orientation (plans, goals). These factors do not cancel risk — a patient with strong protective factors can still be at high risk — but they inform the management plan and the basis for safety planning.
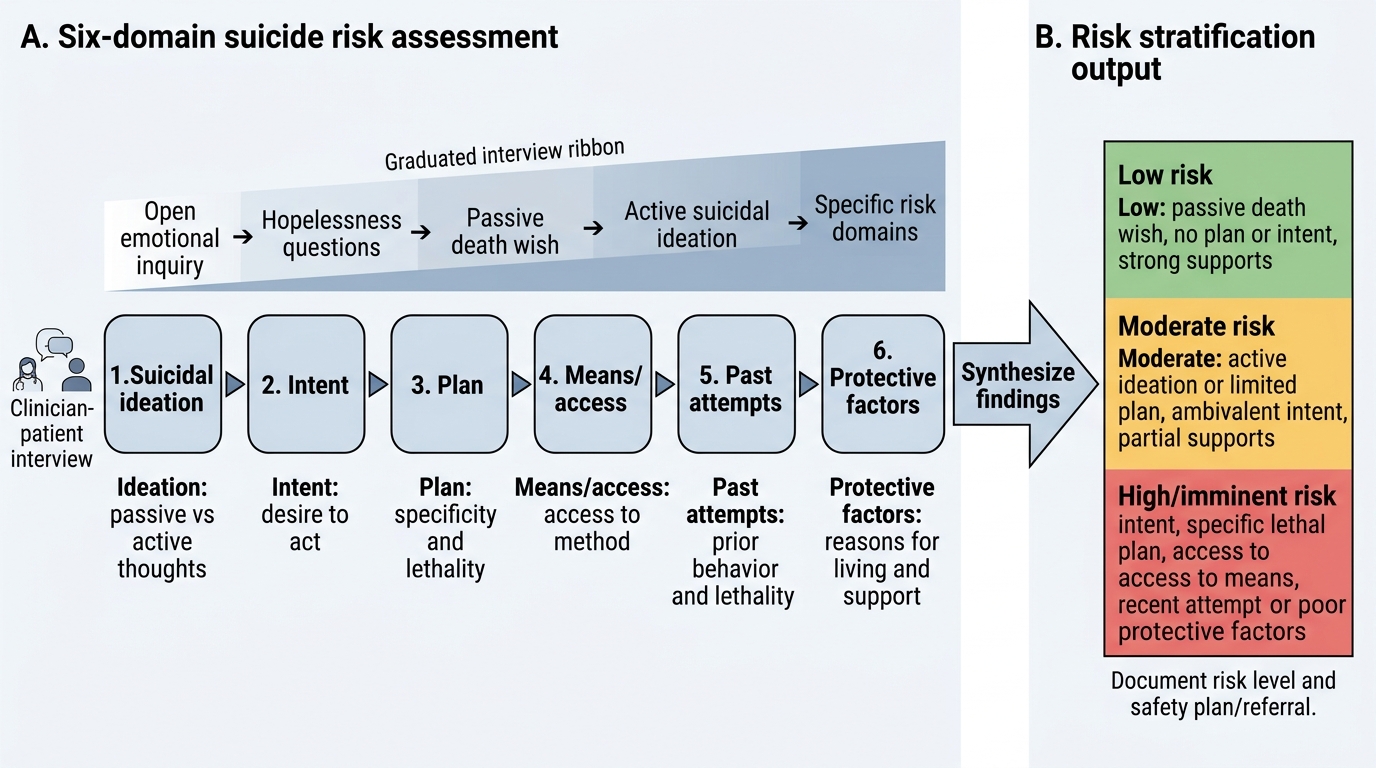
Structured Suicide Risk Assessment Flowchart
The interview technique that threads these six domains together is a graduated escalation of directness. You begin with open inquiry about the patient's current emotional state and wellbeing, transition to questions about hopelessness ("Does the future feel hopeless to you?"), then move to passive ideation ("Have you ever wished you were dead?"), and finally to active ideation and each specific domain above. This graduated approach respects the patient's readiness while ensuring that no domain is omitted.
SELF-CHECK
A 28-year-old woman presents with persistent low mood. She says, 'I sometimes wish I could just fall asleep and not wake up.' She denies any plan or intent to harm herself. Which assessment domain does her statement MOST directly represent?
A. Active suicidal ideation with intent
B. Passive death wish (passive suicidal ideation)
C. A suicidal plan with a specific method
D. Evidence of a prior suicide attempt
Reveal Answer
Answer: B. Passive death wish (passive suicidal ideation)
The statement 'I wish I could fall asleep and not wake up' is the prototypical expression of a passive death wish — a wish for death without active ideation about self-harm or a specific method. This is at the lower end of the suicidal ideation spectrum but must not be dismissed; it represents an entry point into structured assessment. Active ideation requires specific thoughts of killing oneself; a plan requires specificity of method, time, and place.