Page 2 of 14
RD4.1 | Imaging Requisitions, Urgency Communication and Specialist Clarification — SDL Guide (Part 2)
Conveying Clinical Urgency and Clarifying Appropriateness
Two of the three behaviours that RD4.1 names explicitly are conveying clinical urgency to drive correct scheduling, and clarifying appropriateness when in doubt — and both depend on understanding how a radiology department triages and what it means for a study to be appropriate. Urgency is not a single binary of 'urgent or not'; it is a graded judgement that determines where the patient sits in a long queue, and miscommunicating it harms patients in both directions. Over-flagging every request as urgent erodes the meaning of the word and delays the genuinely time-critical patient, while under-flagging a true emergency causes fatal delay. Appropriateness, meanwhile, is the question of whether this study is the right test for this question at all — and the requesting clinician shares responsibility for it.
Conveying urgency — a workable three-tier scheme:
- Routine: no time pressure; the study can be scheduled in the normal queue (days to weeks). Most outpatient imaging.
- Urgent: needed same-day or within ~24 hours because the result will change management soon (e.g. ?DVT in a symptomatic outpatient, suspected significant infection).
- Emergent: needed immediately because delay risks death or major morbidity, and the radiologist should be telephoned, not merely sent an electronic request. Examples include suspected aortic dissection, suspected acute stroke within the thrombolysis window, suspected testicular torsion, and major trauma. For an emergent request, always speak to the radiologist directly and state the time-critical reason.
Clarifying appropriateness — the justification duty:
- When you are unsure whether a study is the right test, or whether it is justified at all, telephone the radiologist before ordering. The radiologist can advise the correct modality, a lower-dose alternative, or whether imaging is needed at all.
- Appropriateness is supported by published referral guidance — the ACR Appropriateness Criteria internationally and AERB referral guidance in India — which rank imaging options by clinical scenario. Under AERB and ICRP principles, every ionising study must be justified, and that justification is shared by the clinician who requests it, not delegated entirely to the radiologist.
- Asking 'is this the right test, and will it change my management?' is the single most powerful appropriateness check, and clarifying with the radiologist when the answer is unclear is exactly the collaborative behaviour RD4.1 requires.
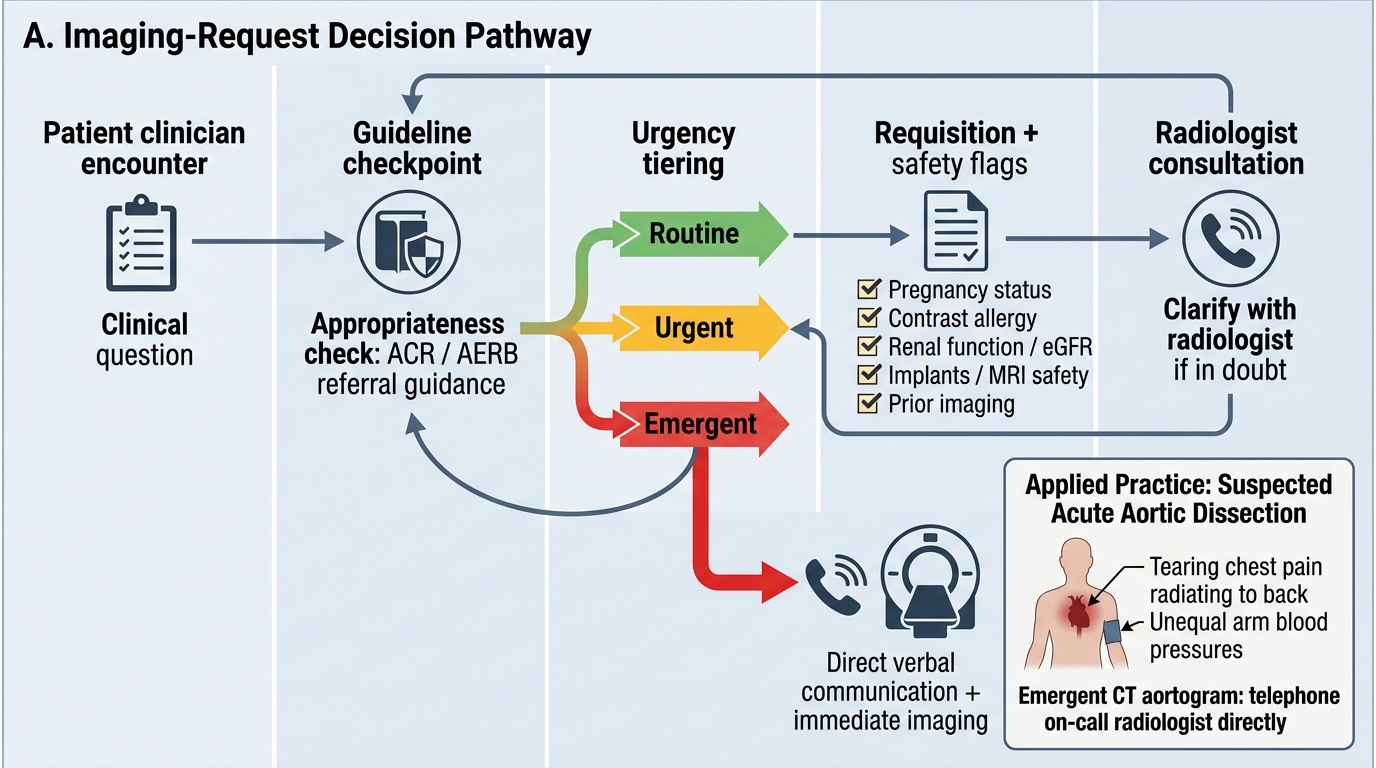
Imaging-Request Decision Pathway
SELF-CHECK
A 58-year-old man presents to the clinic with sudden severe 'tearing' chest pain radiating to the back and a 25 mmHg systolic blood-pressure difference between the arms. You suspect acute aortic dissection. What is the MOST appropriate way to communicate this imaging request?
A. Submit a routine electronic CT request and await the normal queue
B. Submit an electronic request marked 'urgent' and continue with other patients
C. Telephone the on-call radiologist directly, state it is an emergent suspected aortic dissection, and request an immediate CT aortogram
D. Order a routine chest X-ray first and reassess in a few hours
Reveal Answer
Answer: C. Telephone the on-call radiologist directly, state it is an emergent suspected aortic dissection, and request an immediate CT aortogram
Suspected acute aortic dissection is a true emergency where delay risks death, so it should be conveyed as an EMERGENT request by telephoning the radiologist directly rather than relying on an electronic queue — even one marked 'urgent'. Direct verbal communication of the time-critical reason ensures immediate scheduling of the CT aortogram. A routine queue or a delayed chest X-ray reassessment would introduce dangerous delay.
Applied Practice — Worked Requisitions and Closing the Loop
Bringing the components, the method and the urgency/appropriateness judgement together, consider how a real requisition is built and what happens after the study is done — because collaboration with the imaging service does not end when the request is submitted. Closing the loop means acting on the report, ensuring critical results are communicated and received, and not repeating imaging that already exists. Duplicate imaging is a common, costly and (for ionising studies) harmful failure that almost always traces back to a requesting clinician who did not check what had already been done or did not read the existing report.
Worked example — transforming a poor requisition into a good one. Poor: 'USG abdomen. Pain.' Good: 'Mrs Y, 45, RUQ pain and fever 24 h, Murphy's sign positive, ?acute cholecystitis. No prior imaging. Not pregnant. Urgent — same-day please. Contact: Dr Z, ext 412.' The good version names the patient and question, gives focused history, states urgency, addresses safety (pregnancy), and provides contact details — the radiologist can act on it without a phone call.
Closing the imaging loop — the requesting clinician's continuing responsibilities:
- Read the actual report, not just the impression line, and correlate it with the clinical picture (the report may say 'clinical correlation advised' precisely because the question was vague).
- Acknowledge and act on critical/unexpected findings: radiology departments have critical-result communication pathways (e.g. a direct call for an unexpected mass or a life-threatening finding); ensure there is a named clinician to receive and act on these.
- Avoid duplicate imaging: check whether the study has already been done — including at other facilities — before re-requesting. Repeating a CT because the prior images were not retrieved is avoidable radiation.
- Re-clarify if the report does not answer the question: if the report is ambiguous or does not address your clinical concern, contact the radiologist rather than ordering a different scan reflexively.
This closed loop — clear request, correct study, report read and acted upon, no needless repetition — is the full shape of the collaboration RD4.1 describes.
CLINICAL PEARL
Pearl 1 — The specific clinical question is the heart of the requisition. A radiologist can choose the right protocol and search pattern only if they know what you are asking. 'Abdominal pain, please scan' is not a question; '?acute appendicitis' is. If you write nothing else well, write the question well.
Pearl 2 — A blank safety field is not the same as 'no risk'. Recording 'eGFR 78', 'not pregnant', 'no implants' tells the radiologist you checked; leaving the field blank tells them nothing and forces a phone call or an unsafe assumption. Fill every safety flag with present/absent, not silence.
Pearl 3 — Phone, don't queue, for emergencies. For suspected aortic dissection, acute stroke in the thrombolysis window, testicular torsion or major trauma, speak to the radiologist directly. Electronic 'urgent' flags are easily missed; a phone call is not.
Pearl 4 — When in doubt about whether a test is right, ask the radiologist BEFORE ordering. Clarifying appropriateness is a competency, not an imposition — radiologists would far rather advise on the correct study than report an inappropriate one.
Self-Assessment — Requisition, Urgency and Justification
Use these scenarios to test whether you can construct safe requisitions, tier urgency correctly, and clarify appropriateness. Write your answer before reading the discussion.
Scenario A: A 28-year-old woman, last menstrual period uncertain, presents with left iliac fossa pain. The intern requests a CT abdomen-pelvis and writes only 'LIF pain' on the form. List the deficiencies in this requisition and rewrite it.
Discussion: Deficiencies: no specific clinical question, no provisional diagnosis, no pregnancy status despite reproductive age, no urgency, no consideration of a non-ionising first-line study. A rewritten requisition: 'Woman 28, LIF pain 8 h, ?ovarian torsion vs ?appendicitis vs ?ectopic; LMP uncertain — pregnancy test pending/positive? Please advise modality; would prefer pelvic USG first given reproductive age and to avoid ionising radiation. Urgent — same-day. Contact: Dr A, ext 210.' The key safety move is excluding pregnancy and defaulting to ultrasound before any ionising study.
Scenario B: You are unsure whether a young patient with mechanical low back pain of 3 weeks and no red flags needs an MRI lumbar spine, which the patient is requesting. What is the most appropriate action?
Discussion: This is an appropriateness question. Uncomplicated mechanical back pain without red flags does not warrant early MRI, which often shows incidental degenerative findings that mislead management. The appropriate action is to apply referral guidance (ACR Appropriateness Criteria / AERB referral guidance) and, if in any doubt, to telephone the radiologist to clarify before ordering. Imaging is justified only if it will change management — here, watchful waiting and review for red flags is appropriate, and clarifying with the radiologist exemplifies the RD4.1 collaboration behaviour.
Scenario C: A radiologist telephones you about an incidental 3 cm renal mass found on a CT you requested for another reason, and there is no plan documented for follow-up. What does closing the loop require here?
Discussion: Closing the loop requires that the critical/incidental finding is received by a named responsible clinician, documented, and acted upon with a clear follow-up plan (here, urological referral and dedicated renal imaging). Acknowledging the radiologist's critical-result communication, recording it, and arranging definitive follow-up — rather than letting it disappear in the notes — is the requesting clinician's responsibility and the final step of the collaborative loop.