Page 1 of 11
RD7.2 | Imaging in ASOM and CSOM — SDL Guide
Learning Objectives
- State the clinical situations in which imaging is — and is not — indicated in acute suppurative otitis media (ASOM) and chronic suppurative otitis media (CSOM).
- Justify HRCT temporal bone as the workhorse modality for CSOM and complications, and MRI (with non-echo-planar diffusion-weighted imaging) as the modality for cholesteatoma detection, recurrence and intracranial complications.
- Recognise the key HRCT findings of cholesteatoma — non-dependent soft tissue, scutum erosion, ossicular erosion — and the surgically critical erosions of the tegmen, facial canal and lateral semicircular canal.
- Distinguish 'safe' (mucosal/tubotympanic) from 'unsafe' (squamous/atticoantral, cholesteatomatous) CSOM on imaging grounds.
- Integrate provided imaging findings into the management of ASOM and CSOM — including choice of mastoidectomy, surgical caution and the use of diffusion-weighted MRI for recurrence surveillance.
INSTRUCTIONS
Otitis media is one of the commonest conditions you will see in any ENT or paediatric clinic, yet most of it never needs a scan. The skill that RD7.2 demands is not ordering imaging reflexively but knowing the few situations where imaging changes the operation or saves a life — and then being able to read the temporal bone the surgeon will operate on. This module walks you through the clinical triggers for imaging, the rationale for choosing HRCT temporal bone versus MRI, the findings you must recognise, and exactly how those findings rewrite the surgical plan.
References
- Sutton's Textbook of Radiology and Imaging, 8th edition, Chapter on the Temporal Bone and Petrous Apex (textbook)
- Grainger & Allison's Diagnostic Radiology, 7th edition, Chapter on the Temporal Bone (textbook)
- AERB (Atomic Energy Regulatory Board, India) Safety Code for Medical Diagnostic X-ray Equipment and ALARA principles (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 9-year-old girl is brought to casualty on day 5 of a painful, discharging right ear. She now has fever, a tender boggy swelling behind the ear that pushes the pinna forward, and she is unusually drowsy. The intern reaches for antibiotics — but the ENT registrar asks a different question first: 'Has the infection broken out of the middle-ear cleft?' That single question is answered not by the otoscope but by a scan. In uncomplicated acute otitis media a scan is unnecessary and only adds radiation; but the moment a post-auricular abscess, a drooping face, or altered consciousness appears, an HRCT temporal bone — and often an MRI of the brain — becomes the investigation that decides whether this child goes to the ward or straight to theatre. Knowing which patient needs the scanner, and being able to read what it shows, is the applied skill this module builds.
WHY THIS MATTERS
Chronic suppurative otitis media is among the leading preventable causes of acquired hearing loss in India, and its most dangerous form — cholesteatoma — silently erodes bone, threatening the facial nerve, the inner ear and the brain. The NMC competency RD7.2 asks you to integrate provided imaging findings and the description of appearances into the management of ASOM and CSOM — a knows-how (KH) level skill, not mere recall. Whether you become a family physician who must decide when to refer, or a surgeon who plans the mastoidectomy, the ability to link the ear discharge in front of you to the temporal-bone scan on the screen is what keeps a benign-looking ear from becoming meningitis or a dead ear. Every CSOM clinic, every febrile discharging ear in casualty, and every pre-operative ENT planning meeting draws on exactly this reasoning.
RECALL
Before reading further, recall the anatomy and pathology that the imaging will reveal:
- Temporal-bone anatomy (from Anatomy): the middle-ear cleft contains the three ossicles (malleus, incus, stapes); the scutum is the sharp bony spur at the lateral wall of the attic (epitympanum); the tegmen tympani/mastoideum is the thin bony roof separating the middle ear and mastoid from the middle cranial fossa; the facial nerve canal runs through the middle ear (tympanic segment) and mastoid (mastoid segment); the lateral (horizontal) semicircular canal bulges into the attic/aditus.
- ASOM vs CSOM (from ENT): ASOM is acute pyogenic infection of the middle ear with an intact or recently perforated drum; CSOM is chronic infection with a persistent perforation and discharge for more than 6–12 weeks, divided into the mucosal/tubotympanic ('safe') type (central perforation, no bone erosion) and the squamous/atticoantral ('unsafe') type (attic or marginal perforation, cholesteatoma, bone erosion).
- Cholesteatoma: an abnormal accumulation of keratinising stratified squamous epithelium within the middle-ear cleft; it is not a tumour but its enzymatic and pressure effects erode bone — hence the danger.
- CT density and MRI signal: bone is bright (high attenuation) on CT, making CT ideal for cortical erosion; soft tissues (pus, granulation, cholesteatoma) are all of similar low/intermediate density on CT, so CT cannot tell them apart — that is where MRI, especially diffusion-weighted imaging, becomes essential.
Clinical Scenario — When the ENT Surgeon Asks for Imaging in Otitis Media
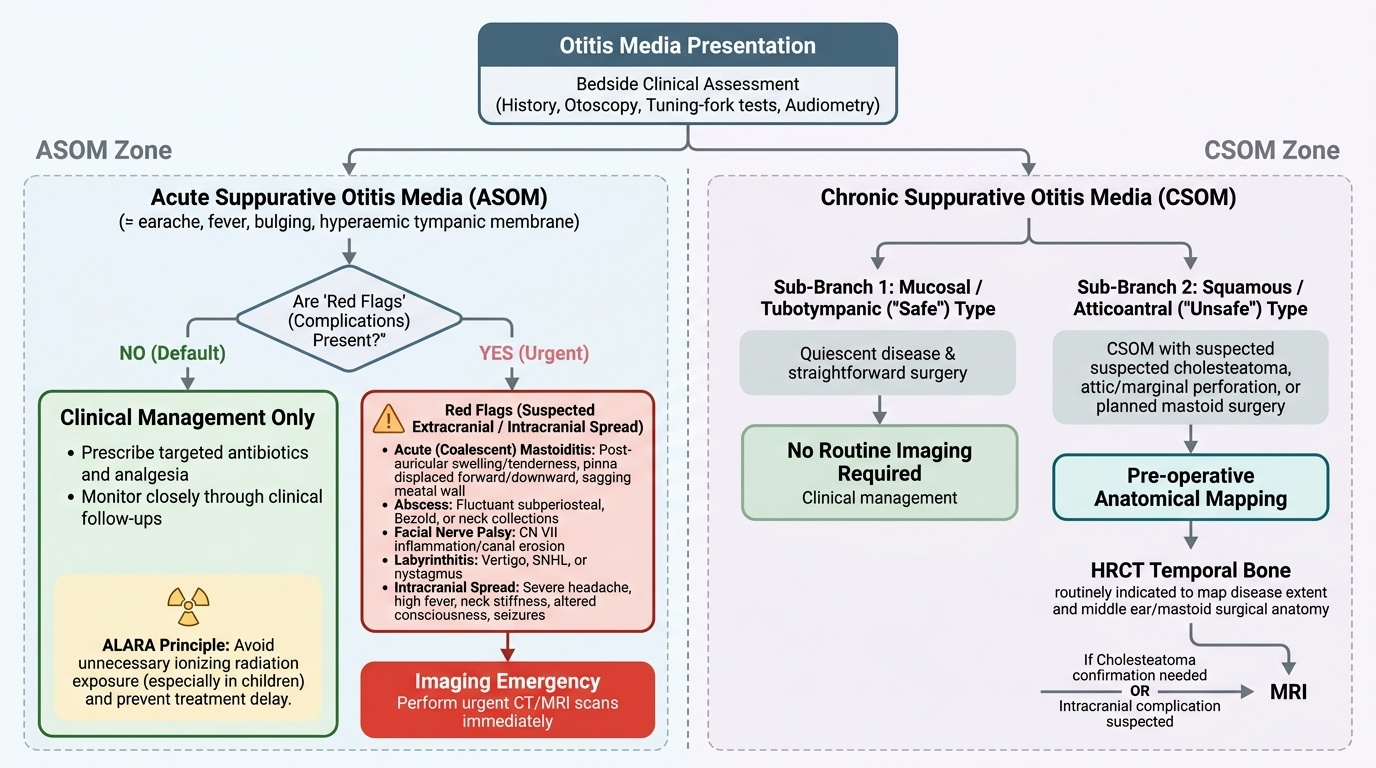
The single most important principle in imaging otitis media is restraint: the overwhelming majority of acute and chronic ear infections are diagnosed and managed entirely on clinical grounds — history, otoscopy, tuning-fork tests and audiometry — without any scan at all. Acute suppurative otitis media (ASOM) is a clinical diagnosis. A child with earache, fever and a bulging, hyperaemic tympanic membrane needs antibiotics and analgesia, not a CT scanner. Imaging in ASOM is reserved exclusively for the situation in which the infection is suspected to have escaped the confines of the middle-ear cleft — that is, when a complication is brewing. Ordering a scan for uncomplicated otitis media exposes the patient (very often a child) to unnecessary ionising radiation and delays treatment, violating the ALARA principle. The clinician's task at the bedside is therefore not 'should I image?' by default, but 'are there red flags that mandate imaging now?'
The red flags that convert ASOM from a clinical diagnosis into an imaging emergency are:
- Acute (coalescent) mastoiditis — post-auricular swelling, redness and tenderness with the pinna pushed forwards and downwards; sagging of the posterosuperior meatal wall.
- Subperiosteal, Bezold or other neck abscess — a fluctuant collection over or below the mastoid.
- Facial nerve palsy — implying erosion or inflammation along the facial canal.
- Labyrinthitis — vertigo, sensorineural hearing loss or nystagmus suggesting inner-ear involvement.
- Intracranial spread — severe headache, persistent high fever, neck stiffness, altered consciousness, seizures or focal neurological signs, raising meningitis, sigmoid sinus thrombosis or intracranial abscess.
Chronic suppurative otitis media (CSOM) has a different imaging logic. The mucosal/tubotympanic ('safe') type often needs no imaging if the disease is quiescent and surgery is straightforward. But the squamous/atticoantral ('unsafe') type — and any CSOM with cholesteatoma, an attic or marginal perforation, or planned mastoid surgery — is routinely imaged with HRCT temporal bone to map the disease and the surgical anatomy before the operation, and with MRI when cholesteatoma must be confirmed or an intracranial complication is suspected.
Provided image
Imaging Strategy — HRCT Temporal Bone, MRI and the Obsolete Plain Film
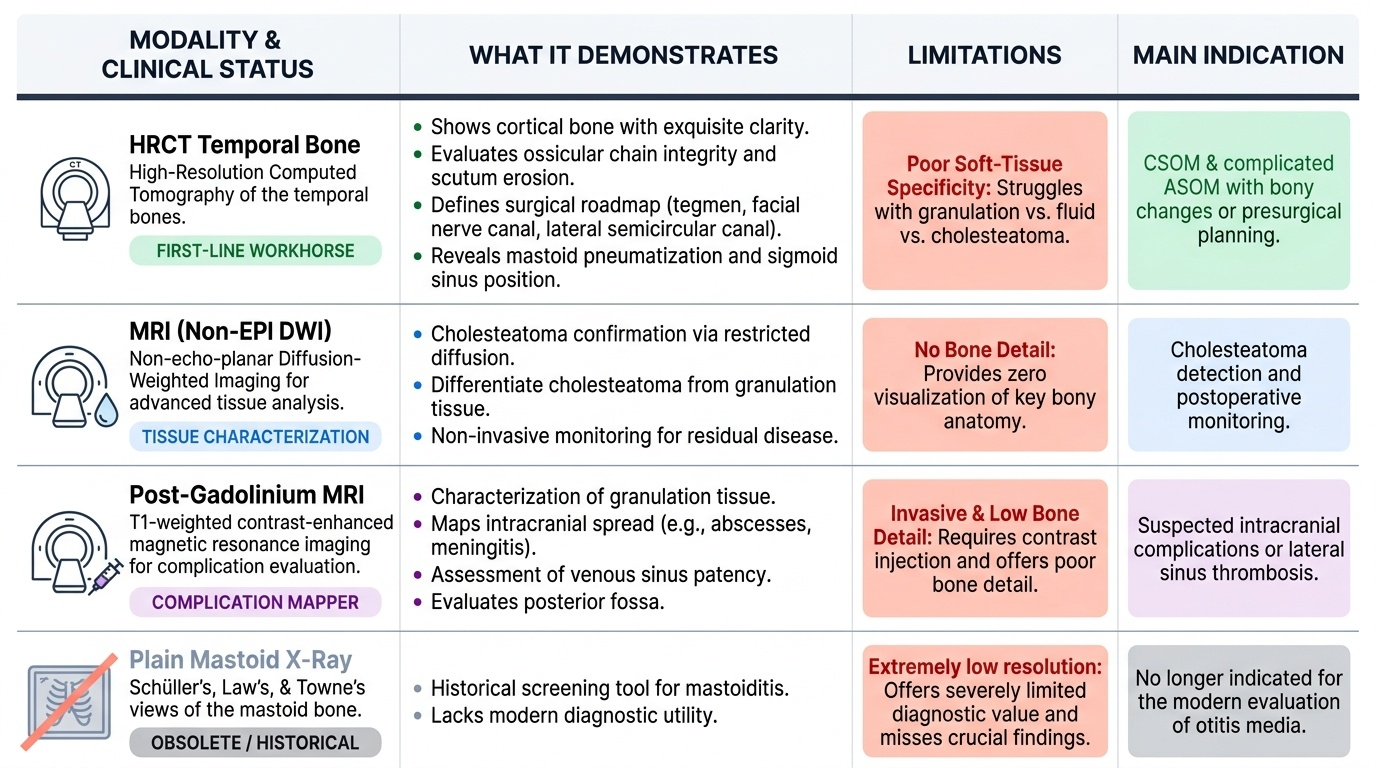
Once imaging is indicated, modality choice follows directly from a single fact of physics: the temporal bone is a dense, intricately air-filled bone, and disease here is judged by what it does to that bone and to the soft tissues within it. High-resolution computed tomography (HRCT) of the temporal bone is the workhorse first investigation for CSOM and complicated ASOM. Acquired as sub-millimetre slices reconstructed in axial and coronal planes with a bone algorithm, HRCT shows cortical bone with exquisite clarity. It defines the extent of disease, the integrity of the ossicular chain, erosion of the scutum (the hallmark of attic cholesteatoma), and — critically for the surgeon — the status of the tegmen, facial nerve canal and lateral semicircular canal, all of which determine how dangerous the operation will be. HRCT also reveals the degree of mastoid pneumatisation and the position of the sigmoid sinus, giving the surgeon a roadmap before the first incision. Its one weakness is that soft tissues — pus, granulation tissue, cholesteatoma and cholesterol granuloma — all look alike (non-specific soft-tissue density); HRCT shows that the middle ear is opacified, but not always with what.
That soft-tissue limitation is exactly what MRI overcomes. The pivotal sequence is non-echo-planar (non-EPI) diffusion-weighted imaging (DWI): cholesteatoma, because of its packed keratin, restricts water diffusion and lights up bright on DWI with a low ADC value, whereas granulation tissue and most post-operative scar do not show the same restriction. Non-EPI DWI therefore lets MRI confirm cholesteatoma, distinguish it from granulation, and — most valuably — detect residual or recurrent cholesteatoma after surgery without re-opening the ear. Post-gadolinium T1 images help in a different way: cholesteatoma does not enhance internally (only a thin peripheral rim), while granulation tissue enhances avidly, and gadolinium delineates intracranial complications such as meningitis, dural enhancement, abscess and sigmoid sinus thrombosis (best shown with MR venography). MRI also images the brain and posterior fossa that CT covers poorly.
Plain mastoid X-ray (Schüller's, Law's, Towne's views) is now largely obsolete for this purpose. It cannot resolve the ossicles, the scutum or the critical canals, and it cannot characterise soft tissue; superimposition of dense bone obscures exactly the structures that matter. It survives only as a historical or resource-limited fallback and should not be relied upon when HRCT is available. Throughout, the ALARA principle governs CT use — sub-millimetre temporal-bone protocols are dose-optimised, and CT is avoided altogether when it would not change management — while MRI demands its own safety screening for contraindications such as non-MR-conditional pacemakers, cochlear implants and intra-ocular metallic foreign bodies.
Provided image
SELF-CHECK
An 8-year-old with uncomplicated acute suppurative otitis media — earache, fever and a bulging red tympanic membrane, no neurological signs and no post-auricular swelling — is brought to the clinic. The parents request 'a scan to be sure'. What is the most appropriate imaging decision?
A. HRCT temporal bone now, to map the middle ear before it worsens
B. No imaging; ASOM is a clinical diagnosis and imaging is reserved for suspected complications
C. Plain mastoid X-ray (Schüller's view) as a low-radiation screening test
D. MRI brain with contrast to exclude early intracranial spread in every case
Reveal Answer
Answer: B. No imaging; ASOM is a clinical diagnosis and imaging is reserved for suspected complications
Uncomplicated ASOM is a clinical diagnosis treated with antibiotics and analgesia; imaging is not routine and only adds radiation (ALARA), particularly in children. Imaging — HRCT temporal bone, with MRI for intracranial concern — is indicated only when a complication is suspected (acute mastoiditis, subperiosteal abscess, facial palsy, labyrinthitis or intracranial spread). Plain mastoid X-ray is obsolete and cannot resolve the relevant anatomy, and routine MRI in every case is unjustified.
Image Findings and Interpretation — Reading the Temporal Bone in ASOM and CSOM
Interpreting temporal-bone imaging is a disciplined search for two questions: where is the disease, and what has it destroyed? Reading the scan in this structured way — rather than simply noting 'middle ear opacified' — is what turns an image into a surgical plan. The findings differ sharply between complicated ASOM, safe CSOM and unsafe (cholesteatomatous) CSOM, and the clinician must be able to recognise each pattern and the specific erosions that carry surgical and life-threatening significance. Because soft tissues are non-specific on CT, the reading combines the bony information from HRCT with the tissue characterisation from MRI DWI; neither alone gives the full picture in difficult cases. A useful habit is to read every temporal-bone scan in a fixed order — middle-ear and mastoid contents, then the scutum, then the ossicular chain, then the tegmen, facial canal and lateral semicircular canal — so that no surgically critical erosion is ever overlooked.
Complicated ASOM — what HRCT and MRI show:
- Coalescent mastoiditis: loss (demineralisation/erosion) of the thin bony septa between mastoid air cells, which become confluent and fluid-filled, plus opacification of the mastoid and middle ear.
- Subperiosteal abscess: a rim-enhancing fluid collection over the mastoid cortex, often with an adjacent cortical defect; best characterised on contrast CT or MRI.
- Intracranial complications (on contrast-enhanced MRI): meningeal/dural enhancement, intracranial (extradural, subdural or temporal-lobe/cerebellar) abscess, and sigmoid sinus thrombosis seen as a non-enhancing filling defect in the sinus on post-contrast images or MR venography.
Safe (mucosal/tubotympanic) CSOM — what HRCT shows:
- Soft-tissue opacification or fluid in the middle ear and mastoid without bone erosion; the scutum, ossicles and critical canals are intact. Tympanosclerosis may appear as foci of calcification.
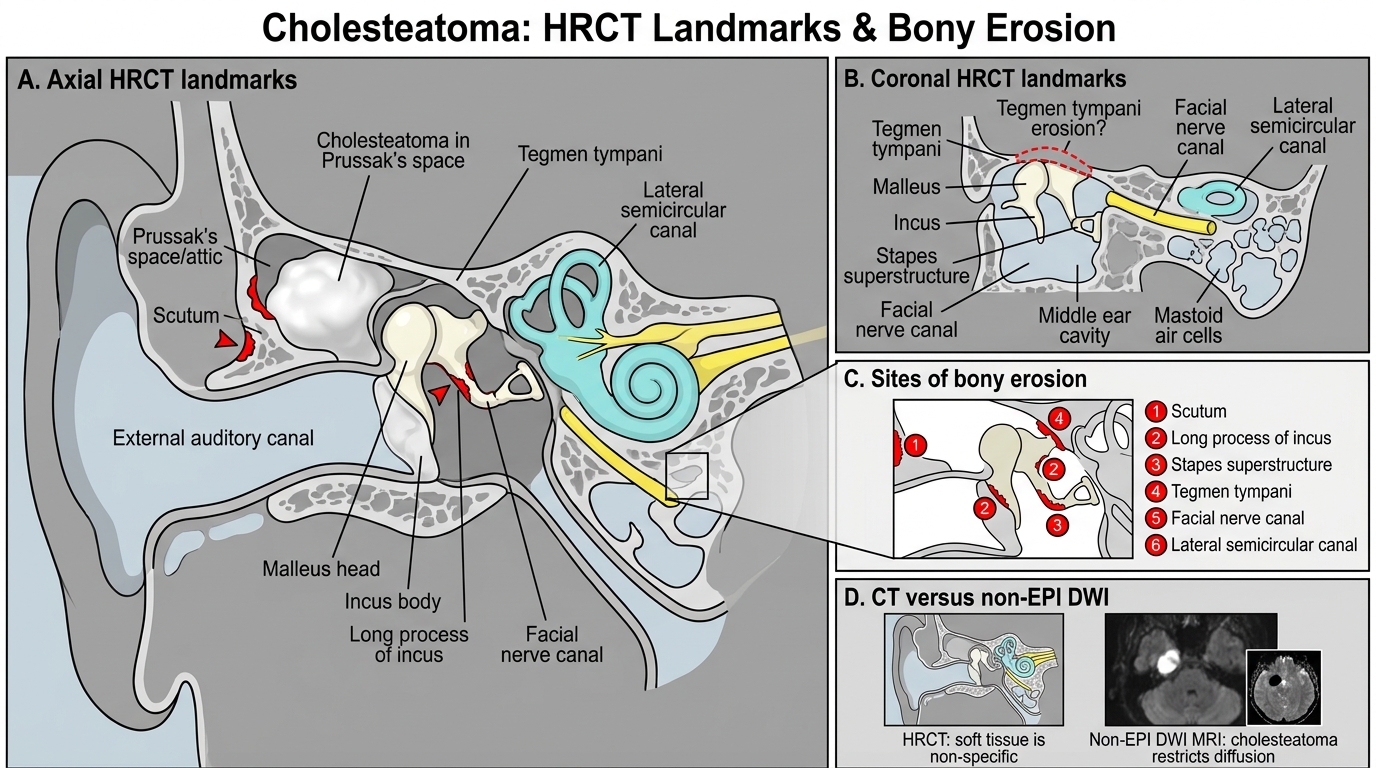
Unsafe (squamous/atticoantral) CSOM with cholesteatoma — the findings you must not miss:
- A non-dependent soft-tissue mass, classically in Prussak's space (the attic, between the scutum and the neck of the malleus), which expands the space rather than simply layering dependently like fluid.
- Scutum erosion — blunting/erosion of the sharp scutum is an early and characteristic sign of attic cholesteatoma.
- Ossicular erosion — the long process of the incus and the stapes superstructure are most often eroded, frequently with associated conductive hearing loss.
- Surgically critical erosions: tegmen dehiscence (risk of intracranial extension and CSF leak), facial nerve canal erosion (risk of facial palsy and intra-operative nerve injury) and lateral semicircular canal fistula (risk of vertigo, sensorineural loss and a labyrinthine breach during surgery).
- On MRI, the soft tissue restricts on non-EPI DWI (bright, low ADC) — confirming cholesteatoma and distinguishing it from non-restricting granulation tissue or cholesterol granuloma (the latter classically bright on both T1 and T2).
HRCT Temporal Bone Landmarks in Cholesteatoma
SELF-CHECK
A 30-year-old with long-standing right ear discharge and an attic perforation has an HRCT temporal bone showing a non-dependent soft-tissue mass in Prussak's space with erosion of the scutum and the long process of the incus. The middle ear is otherwise opacified and the surgeon needs to know whether this is cholesteatoma or just granulation tissue. Which investigation best characterises the soft tissue?
A. Repeat HRCT with intravenous iodinated contrast, which will enhance cholesteatoma strongly
B. Plain mastoid X-ray (Law's view) to confirm the attic disease
C. MRI with non-echo-planar diffusion-weighted imaging — cholesteatoma restricts diffusion (bright on DWI, low ADC) whereas granulation tissue does not
D. No further imaging is needed; HRCT soft-tissue density reliably distinguishes cholesteatoma from granulation
Reveal Answer
Answer: C. MRI with non-echo-planar diffusion-weighted imaging — cholesteatoma restricts diffusion (bright on DWI, low ADC) whereas granulation tissue does not
On HRCT, cholesteatoma, granulation tissue and cholesterol granuloma all appear as non-specific soft-tissue density, so CT cannot reliably tell them apart. Non-echo-planar (non-EPI) diffusion-weighted MRI is the key sequence: cholesteatoma restricts diffusion (bright on DWI with low ADC) because of its packed keratin, whereas granulation tissue does not. Cholesteatoma does not enhance internally (only a thin peripheral rim), so contrast CT does not characterise it well, and plain X-ray cannot resolve the attic anatomy.