Page 4 of 14
RD1.1 | Core Principles of X-ray, Fluoroscopy, CT, Ultrasound, Nuclear Medicine and MRI — SDL Guide
Learning Objectives
- Describe the physical basis and equipment of X-ray, fluoroscopy, CT, ultrasound, nuclear medicine and MRI.
- State the clinical niche, radiation dose, and key safety constraints for each modality.
- Apply the ALARA principle and identify the role of the AERB as India's radiation regulator.
- Select the appropriate first-line imaging modality for common clinical scenarios.
- Identify contraindications to contrast agents and to MRI.
INSTRUCTIONS
Medical imaging is the foundation of modern diagnosis, yet the clinical power of each modality depends entirely on understanding its physical basis, dose profile, and safety envelope. An MBBS graduate ordering investigations must know not only which modality answers the clinical question best but also why — and what harms the inappropriate choice carries. This module equips you with that reasoning framework before you encounter patients in ward and casualty settings.
References
- Sutton's Textbook of Radiology, 6th edition, Chapter 1 (Physics of Medical Imaging) (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter 1 (Principles of Medical Imaging) (textbook)
- Atomic Energy Regulatory Board (AERB) Safety Manual for Diagnostic Radiology, India (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old woman in her first trimester arrives at the emergency department after a road-traffic accident. The trauma team wants to order a full-body CT scan. Her abdomen is tender and the surgical team is concerned about solid-organ injury. Before clicking 'order,' pause: CT delivers ~8–10 mSv to the abdomen — equivalent to several hundred chest X-rays — and the fetal gonads are in the beam. Is there an alternative? Could focused abdominal sonography for trauma (FAST) answer the immediate life-threatening question without ionising the fetus? This collision between clinical urgency and radiation risk lives at the heart of radiodiagnosis. Every imaging decision you make as a clinician will require this reasoning: which modality, which dose, which benefit outweighs which risk.
WHY THIS MATTERS
Misplaced imaging requests are one of the most correctable sources of patient harm in hospital practice. Ordering a CT instead of an ultrasound in a pregnant woman, requesting plain films where MRI would be diagnostic, or giving iodinated contrast to a patient with eGFR of 22 — each is a clinical error, not a radiology department problem. The NMC competency RD1.1 requires you to understand the physical basis of each modality so that your ordering decisions are grounded in evidence, not habit. Furthermore, India's Atomic Energy Regulatory Board (AERB) mandates that all ionising procedures be clinically justified — a standard that falls on the requesting clinician, not only the radiologist. This knowledge is tested in your clinical postings, in professional examinations, and in every ward round discussion that begins with 'what imaging should we do?'
RECALL
Before reading further, bring to mind the basic physics you learned in Year-1:
- Electromagnetic spectrum: X-rays occupy the high-frequency, short-wavelength end of the EM spectrum and carry enough energy to ionise atoms.
- Wave–particle duality: X-ray photons interact with matter via photoelectric absorption (dominant at low kV, determines tissue contrast) and Compton scattering (dominant at higher kV, contributes to scatter).
- Sound waves: Ultrasound is mechanical — longitudinal pressure waves propagate through tissue; they are not electromagnetic and carry no ionising energy.
- Magnetic field and nuclear spin: Protons (hydrogen nuclei) have spin angular momentum; in a strong external magnetic field they align and precess at the Larmor frequency. This is the physical foundation of MRI.
- Radioactivity: Gamma rays are high-energy photons emitted by unstable nuclei — the basis of nuclear medicine imaging.
If any of these feel unfamiliar, a quick review of your Year-1 biophysics notes before continuing will make the mechanisms below much clearer.
Why Imaging Modalities Matter: The Diagnostic Toolbox in Clinical Practice
Modern clinical diagnosis rests on a toolkit of six imaging modalities, each answering a specific class of clinical question with a distinct physical mechanism. The intellectual error that leads to inappropriate imaging is treating the six modalities as interchangeable alternatives ranked by availability or cost. They are not interchangeable: each modality has a primary clinical niche defined by the tissue contrast it generates, the spatial resolution it achieves, the temporal resolution it offers, the radiation dose it delivers or does not deliver, and the safety constraints it carries. Choosing the right modality is one of the most consistently testable clinical reasoning skills in final-year medicine, and it is also one of the most frequent points of avoidable patient harm — from unnecessary radiation in children to delayed diagnosis when an inappropriate modality is chosen for time-critical presentations.
A framework that will serve you throughout clinical training groups these modalities into two families by energy source:
- Ionising radiation modalities — X-ray/plain radiography, fluoroscopy, computed tomography (CT), and nuclear medicine scintigraphy. Each deposits ionising energy in tissue and carries a dose that must be justified under the ALARA principle (As Low As Reasonably Achievable).
- Non-ionising modalities — diagnostic ultrasound (USG) and magnetic resonance imaging (MRI). Neither deposits ionising energy; USG uses mechanical sound waves and MRI uses a static magnetic field combined with radiofrequency pulses.
The clinical implication is immediate: when an equivalent diagnostic answer is available from a non-ionising modality, the ionising option requires explicit clinical justification. This is the reasoning logic that underlies every imaging request.
Ionising Modalities — X-ray, Fluoroscopy, CT and Nuclear Medicine
Understanding each ionising modality requires grasping its physical basis, the clinical image it produces, and the approximate radiation dose it delivers — because dose is a direct input to the risk-benefit calculus that governs every request.
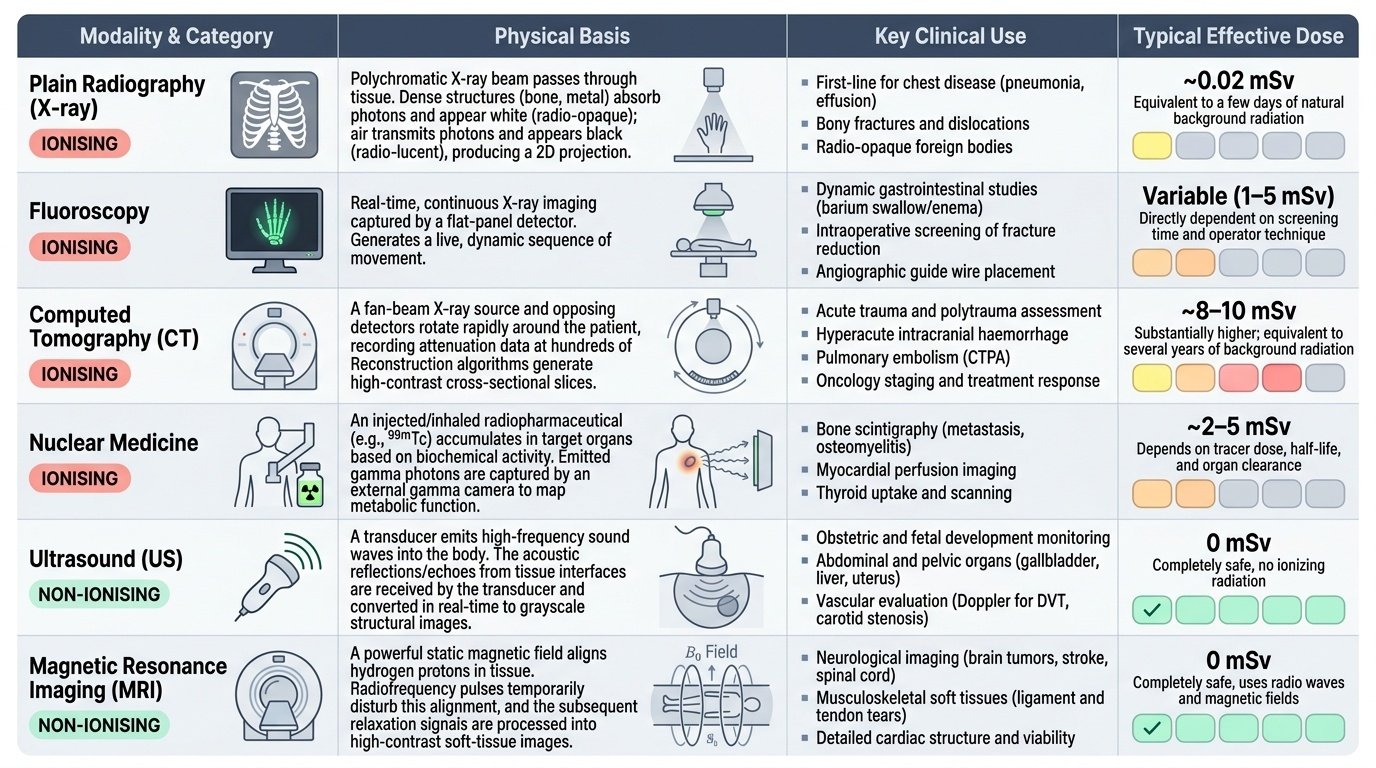
Plain radiography (X-ray) generates a two-dimensional projection image. The X-ray tube emits a polychromatic beam of photons; as they pass through tissue, dense structures (cortical bone, metal, calcification) absorb more photons and appear white (opaque/radio-opaque) on the final image, while air-filled structures transmit nearly all photons and appear black (radio-lucent). The effective dose of a chest X-ray is approximately 0.02 mSv — comparable to a few days of background radiation. Plain radiography is first-line for chest disease, bony fractures, and foreign bodies.
Fluoroscopy is real-time, continuous X-ray imaging displayed on a monitor. The image intensifier (or modern flat-panel detector) captures a live sequence, enabling dynamic studies — barium swallow, barium enema, and intraoperative screening of fracture reduction. Fluoroscopy delivers a higher cumulative dose than a single static X-ray because of its prolonged acquisition; dose depends directly on screening time and operator technique.
Computed tomography (CT) rotates a fan-beam X-ray source around the patient while detectors on the opposite side record attenuation data at hundreds of angles. A reconstruction algorithm generates cross-sectional images with far superior contrast resolution compared with plain films, and modern multi-detector CT (MDCT) acquires volumetric data in seconds. The effective dose is substantially higher: a CT abdomen–pelvis is approximately 8–10 mSv. CT is first-line for acute trauma, intracranial haemorrhage, pulmonary embolism, and cancer staging.
Nuclear medicine scintigraphy introduces a radiopharmaceutical — a compound labelled with a gamma-emitting radionuclide (e.g., technetium-99m, ^99mTc) — intravenously or by inhalation. The radiopharmaceutical accumulates in target tissue based on its biochemical behaviour, and a gamma camera images the emitted photons from outside the body. The result is a functional image: it shows HOW tissue is working, not what it looks like anatomically. Common applications include bone scintigraphy (metastasis, osteomyelitis), thyroid scanning, ventilation–perfusion (V/Q) lung scan, and renal (DTPA/MAG3) scans. PET-CT combines a positron-emitting tracer (typically ^18F-FDG, taken up by metabolically active tumours) with CT for precise anatomical localisation.
Provided image
Non-ionising Modalities — Diagnostic Ultrasound and MRI
The two non-ionising modalities exploit entirely different physical phenomena and carry distinct safety profiles.
Diagnostic ultrasound (USG) uses piezoelectric crystals in a transducer that convert electrical pulses into high-frequency sound waves (typically 2–18 MHz for clinical use; higher frequencies give better resolution but less penetration). The waves propagate through tissue, and at acoustic interfaces (boundaries between tissues of different acoustic impedance) a portion is reflected back as an echo. The transducer also functions as a receiver; the time delay and amplitude of returning echoes are processed to build a real-time grey-scale image (B-mode). Doppler imaging adds velocity information by detecting frequency shifts in moving blood cells. USG produces no ionising radiation and has no confirmed biological harm at diagnostic power levels, making it the first-line modality for abdominal, pelvic, biliary, renal, obstetric, thyroid, and vascular assessment, and the preferred or exclusive modality in pregnancy and paediatric patients.
Magnetic resonance imaging (MRI) exploits the nuclear magnetic resonance (NMR) properties of hydrogen protons, which are abundant in biological tissue (predominantly in water and fat). The patient is placed in a strong static magnetic field (typically 1.5–3 Tesla in clinical systems). A radiofrequency (RF) pulse tuned to the Larmor frequency of protons at that field strength tips the magnetisation vector. When the RF pulse is switched off, protons relax back to equilibrium in two independent ways: longitudinal recovery (T1 relaxation) and transverse decay (T2 relaxation). Different tissues relax at different rates, creating inherently superior soft-tissue contrast compared with any ionising modality. Varying pulse sequences (T1-weighted, T2-weighted, FLAIR, diffusion-weighted imaging/DWI, etc.) accentuates different tissue characteristics. No ionising radiation is used.
MRI contraindications — this is a patient safety imperative: MRI is NOT free of contraindications. The strong static magnetic field and RF pulses are hazardous in the presence of:
- Certain cardiac pacemakers and ICDs (most older devices; newer MRI-conditional devices require specific protocols)
- Cochlear implants (unless explicitly MRI-conditional)
- Intra-ocular ferromagnetic foreign bodies (sheet-metal workers — screening X-ray mandatory before MRI)
- Certain cerebral aneurysm clips (ferromagnetic clips may move in the field)
- Some penile implants and joint prostheses (device-specific; many are now MRI-safe at 1.5 T)
Claiming 'MRI has no contraindications' is factually wrong and clinically dangerous.
SELF-CHECK
A 6-year-old child presents with right-sided abdominal pain and fever. Appendicitis is suspected. Which imaging modality is the appropriate first-line investigation to avoid radiation exposure?
A. Abdominal CT with intravenous contrast
B. Plain X-ray of the abdomen
C. Abdominal ultrasound
D. MRI abdomen
Reveal Answer
Answer: C. Abdominal ultrasound
Ultrasound is first-line in paediatric abdominal assessment because it carries no ionising radiation and can visualise an inflamed, non-compressible appendix. CT delivers significant radiation dose and is reserved for cases where ultrasound is inconclusive. Plain X-ray has poor sensitivity for appendicitis. MRI is an option in equivocal cases but is slower and less accessible; USG is the initial step.