Page 1 of 17
RD5.1 | Normal X-ray Anatomy in Adults, Neonates and Children — SDL Guide
Learning Objectives
- Apply a fixed, systematic search pattern to a chest, abdominal, musculoskeletal and Water's-view radiograph.
- Identify and name the normal radiographic structures on each of these films in an adult.
- Recognise the normal neonatal thymic shadow ('sail sign') and avoid mistaking it for pathology.
- Recognise normal epiphyses, ossification centres and growth plates (physes) on a paediatric joint film and distinguish them from fractures.
- State the projection-dependent pitfalls (AP vs PA, supine) that produce false-positive findings such as spurious cardiomegaly.
INSTRUCTIONS
Image interpretation begins not with disease but with a deeply internalised picture of normal. A clinician who cannot confidently say 'this chest film is normal' cannot reliably say which one is abnormal — and the two most dangerous errors in early radiology are missing a real lesion and inventing one that is not there. This module builds the disciplined normal-radiograph template across the chest, abdomen, musculoskeletal system and paranasal sinuses, and then layers on the two special-population normals — the neonatal thymus and the paediatric growth plate — that are most often misread as pathology. Master the normal here and the emergency-interpretation and age-estimation skills that follow become pattern-matching against a known baseline.
References
- Sutton's Textbook of Radiology and Imaging, 7th edition, Chapters on the Normal Chest and Skeletal System (textbook)
- Grainger & Allison's Diagnostic Radiology, 7th edition, Sections on the Normal Chest and Paediatric Skeleton (textbook)
- Atomic Energy Regulatory Board (AERB) Safety Code for Diagnostic Radiology, India — paediatric dose optimisation (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A first-year resident is handed the chest X-ray of a 2-week-old neonate admitted with poor feeding. She sees a broad, triangular soft-tissue density at the right upper mediastinum and writes 'right upper-zone mass — suggest CT.' The consultant glances at the film and says one word: thymus. The 'mass' is the normal neonatal thymic shadow — the classic 'sail sign' — present in almost every healthy infant. The resident's error was not a knowledge gap about tumours; it was an absent template of normal. She had never deliberately learnt what a NORMAL neonatal chest film looks like, so the first unfamiliar shadow became a lesion. This is the single most important truth of image interpretation: you detect the abnormal only against a securely held picture of the normal. Before you can read pathology, you must be able to read — and confidently report — a normal radiograph in an adult, a neonate and a child.
WHY THIS MATTERS
Every clinician who orders a plain radiograph will, sooner or later, look at the image before the formal report arrives — in casualty at 2 a.m., on a ward round, in a peripheral health centre with no radiologist on site. The NMC competency RD5.1 is explicit that an MBBS graduate must be able to interpret NORMAL X-ray images of the chest, abdomen and musculoskeletal system, and specifically must identify the normal neonatal thymic shadow and the normal paediatric epiphysis and growth plate. The clinical stakes are symmetrical. Calling a normal film abnormal launches a cascade of unnecessary CT scans (radiation, cost, incidentalomas), referrals and parental anxiety; calling an abnormal film normal delays a diagnosis that may be time-critical, such as a pneumothorax or a displaced fracture. Both errors are reduced by the same discipline: a fixed search pattern applied to a securely learnt normal template, with explicit awareness of the projection and age-related variants that masquerade as disease. This is a daily, examinable, patient-safety skill — not a radiologist's specialism alone.
RECALL
Before reading further, bring to mind the anatomy and physics you have already learnt that this skill depends on:
- Thoracic anatomy (AN, Year 1): the position of the trachea and carina, the cardiac chambers that form each heart border (right border = right atrium; left border = left ventricle and the aortic knuckle/pulmonary outflow above), the hila (pulmonary arteries and veins), and the domes of the diaphragm.
- Abdominal anatomy: the retroperitoneal psoas muscles, the renal and hepatic/splenic outlines, and the normal distribution of bowel gas.
- Skeletal anatomy: the cortex (dense outer bone), medulla (trabecular inner bone), the joint space (radiolucent because articular cartilage is not visible on plain film), and physiological alignment.
- Radiographic densities (RD-foundation): the five basic densities from darkest to brightest — air (black), fat, soft tissue/water, bone, and metal/contrast (white) — and that an X-ray is a SUMMATION (projection) image, so overlapping structures add up.
- Paediatric skeletal development (AN/PY): that children's long bones grow at cartilaginous growth plates (physes) which are radiolucent and progressively ossify and fuse with age.
If any of these feel hazy, a quick review now will make the systematic read below far easier to follow.
Why a Disciplined Normal-Radiograph Template Is the First Interpretation Skill
Radiograph interpretation is a perceptual skill built on a stored template, not a list of facts to recall. Expert radiologists do not consciously reason their way across every film; they hold a richly detailed internal model of the normal appearance for each projection and each age group, and an abnormality declares itself as a departure from that model. The beginner's problem is that the template is sparse: with no securely held picture of normal, every unfamiliar shadow is ambiguous, and the brain resolves ambiguity unpredictably — sometimes by ignoring a real lesion, sometimes by inventing one. The corrective is twofold and is the heart of this module: first, deliberately build the normal template region by region; second, impose a fixed search pattern so that no area is skipped under the time pressure and tunnel-vision that produce 'satisfaction of search' errors (stopping after the first finding and missing a second).
The clinical consequences of an absent or weak normal template are concrete and bidirectional:
- False positives — calling normal abnormal — generate unnecessary CT scans (and their radiation dose), specialist referrals, repeat films, cost, and patient/parental anxiety. In children, the misread normal thymus and the misread growth plate are the classic examples.
- False negatives — calling abnormal normal — delay diagnosis. A small apical pneumothorax, an early consolidation behind the heart, or a subtle cortical fracture is missed precisely because the reader never compared the film against a complete normal checklist.
The competency RD5.1 therefore asks for more than 'looking at X-rays': it asks you to identify the named normal structures on the chest, abdomen and musculoskeletal films, and to recognise the two paediatric normals (thymic shadow, epiphysis/growth plate) that are most often misclassified. Building that template is the first and most transferable interpretation skill, because the emergency-interpretation (RD5.3) and age-estimation (RD5.2) skills that follow are simply structured deviations from this normal baseline.
Governing Principles — Densities, Projection, Silhouette and the Search Pattern
Four governing principles underpin every normal read, and getting them right prevents the most common false-positive errors. The first is the five radiographic densities: from darkest to brightest on the film, air (lung, bowel gas — black), fat (grey-black), soft tissue / water (muscle, blood, solid organs — mid grey), bone / calcification (white), and metal / contrast (brightest white). A structure is visible only where it abuts a tissue of DIFFERENT density; this is the basis of the next principle. The second is the silhouette sign: two structures of the SAME density in contact lose their border. The right heart border is seen because the air-filled right middle lobe abuts the soft-tissue heart; if right-middle-lobe pneumonia replaces that air with water density, the right heart border is effaced — a normal silhouette LOST signals disease, and a normal silhouette PRESENT is reassuring.
The third principle is projection, the single most important guard against spurious findings. A PA (postero-anterior) erect chest film — patient's chest against the detector, beam from behind — is the standard: the heart is close to the detector and magnified minimally, so the cardiothoracic ratio is normally <0.5. An AP (antero-posterior) or supine/portable film magnifies the heart and widens the mediastinum because the heart is farther from the detector; you must NOT diagnose cardiomegaly on an AP or supine film. Rotation, inspiration depth and patient position all alter appearances and are checked first. The fourth principle is the fixed search pattern — a memorised checklist applied identically every time so no zone is skipped.
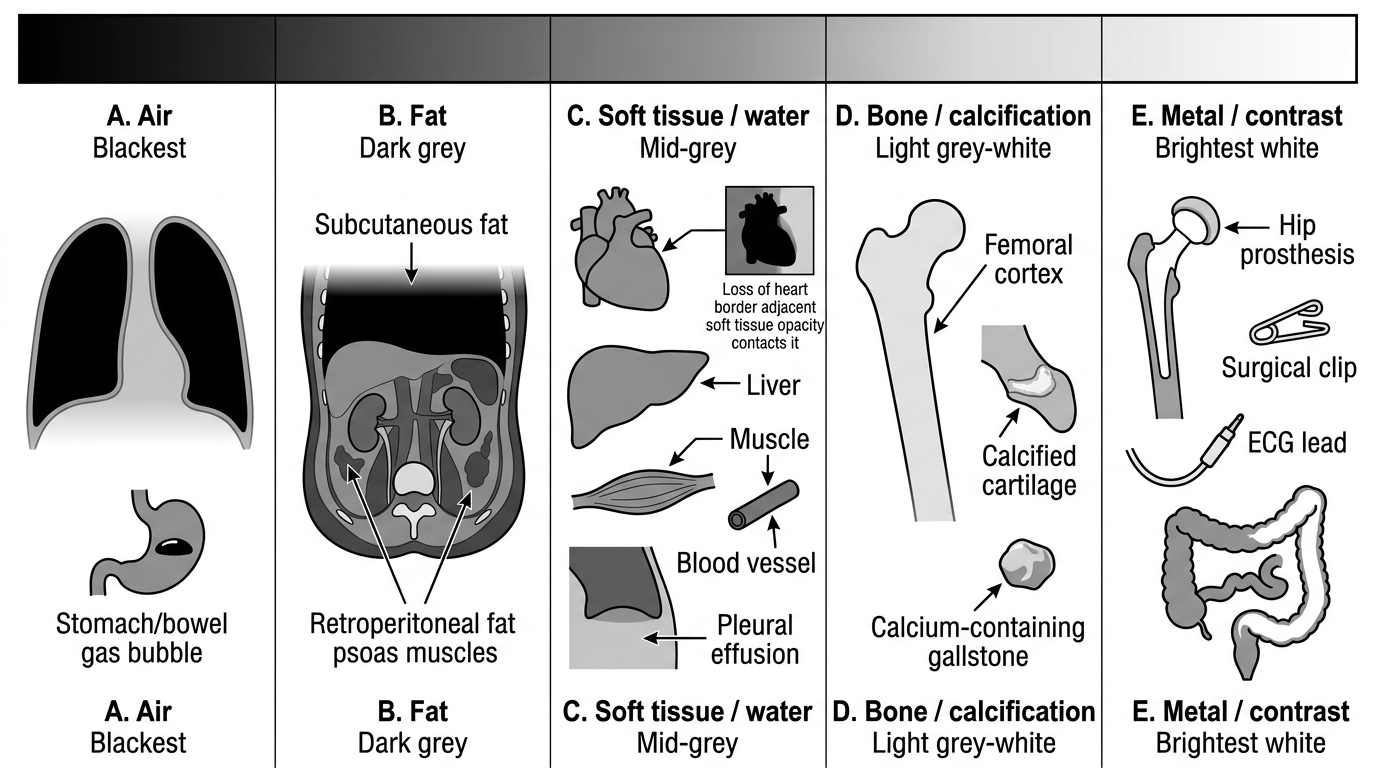
Five Basic Radiographic Densities
- Air — lung parenchyma, gastric/bowel gas (blackest).
- Fat — subcutaneous fat, retroperitoneal fat outlining the psoas and kidneys.
- Soft tissue / water — heart, solid organs, muscle, blood, effusions (all the same mid-grey, hence the silhouette sign).
- Bone / calcification — cortex, calcified cartilage, gallstones with calcium.
- Metal / contrast — prostheses, surgical clips, ECG leads, iodinated/barium contrast (brightest).
Method — A Systematic Read of the Adult Chest, Abdomen, MSK and PNS Films
A systematic read is a memorised sequence applied to every film so that perception is exhaustive rather than opportunistic. Always begin with the demographics and technical adequacy — patient identity and date, projection (PA vs AP), rotation (medial ends of the clavicles equidistant from the spinous processes), inspiration (5–6 anterior ribs above the diaphragm on a good adult inspiration), and penetration. Only then read the anatomy in a fixed order. The mnemonic frameworks below are not the point — the discipline of never skipping a zone is. Below, each region's normal structures are listed in the order a sound search pattern names them.
Chest (PA erect): Airway and mediastinum — trachea central, carina, aortic knuckle, mediastinal width. Breathing/lungs — both lung fields compared zone by zone, vascular markings tapering to the periphery, no focal opacity. Cardiac — cardiac borders (right border = right atrium; left border = left ventricle), cardiothoracic ratio <0.5 on a PA film. Diaphragm — both hemidiaphragms (right usually slightly higher than left), sharp costophrenic and cardiophrenic angles, no air under the diaphragm. Everything else (bones and soft tissues) — ribs, clavicles, scapulae, and the soft tissues including the breast shadows.
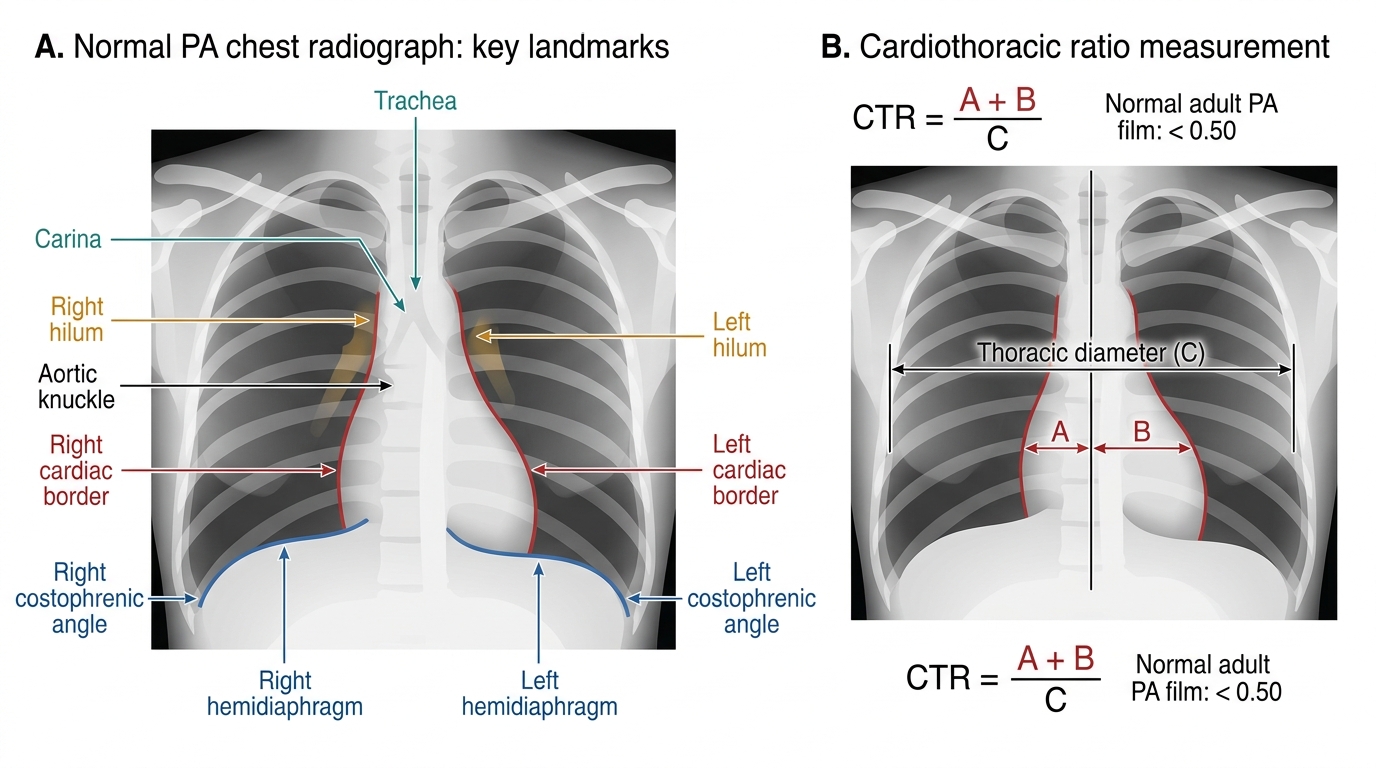
Normal PA Chest Radiograph Landmarks and Cardiothoracic Ratio
Abdomen (supine AXR): bowel gas pattern (small bowel central with valvulae conniventes crossing the full lumen; large bowel peripheral with haustra that do not cross), no abnormal dilatation, the psoas muscle outlines (loss may indicate retroperitoneal pathology but is a soft sign), renal, hepatic and splenic outlines where fat planes allow, the bony pelvis and lumbar spine, and no abnormal calcification or free gas.
Musculoskeletal (long bones, joints, spine): assess in the order alignment, bone (cortex continuous and smooth, normal trabecular pattern in the medulla), cartilage/joint (the joint space — actually articular cartilage, which is radiolucent — should be uniform and preserved), and soft tissues. Always obtain TWO orthogonal views (e.g. AP and lateral) because a fracture or dislocation can be invisible on a single projection. Be aware that nutrient vessel canals cross the cortex obliquely and are a normal finding, not a fracture.
Paranasal sinuses — Water's (occipitomental) view: this is the standard PNS projection. Normally the frontal, maxillary and ethmoid air cells are LUCENT (air-filled, dark); the orbits and the maxillary antra are symmetrical; and the petrous ridges are projected BELOW the floor of the maxillary antra in a correctly angled Water's view (an important technical check). Loss of the normal sinus lucency — an opaque antrum or an air–fluid level — signals sinus pathology against this normal baseline.
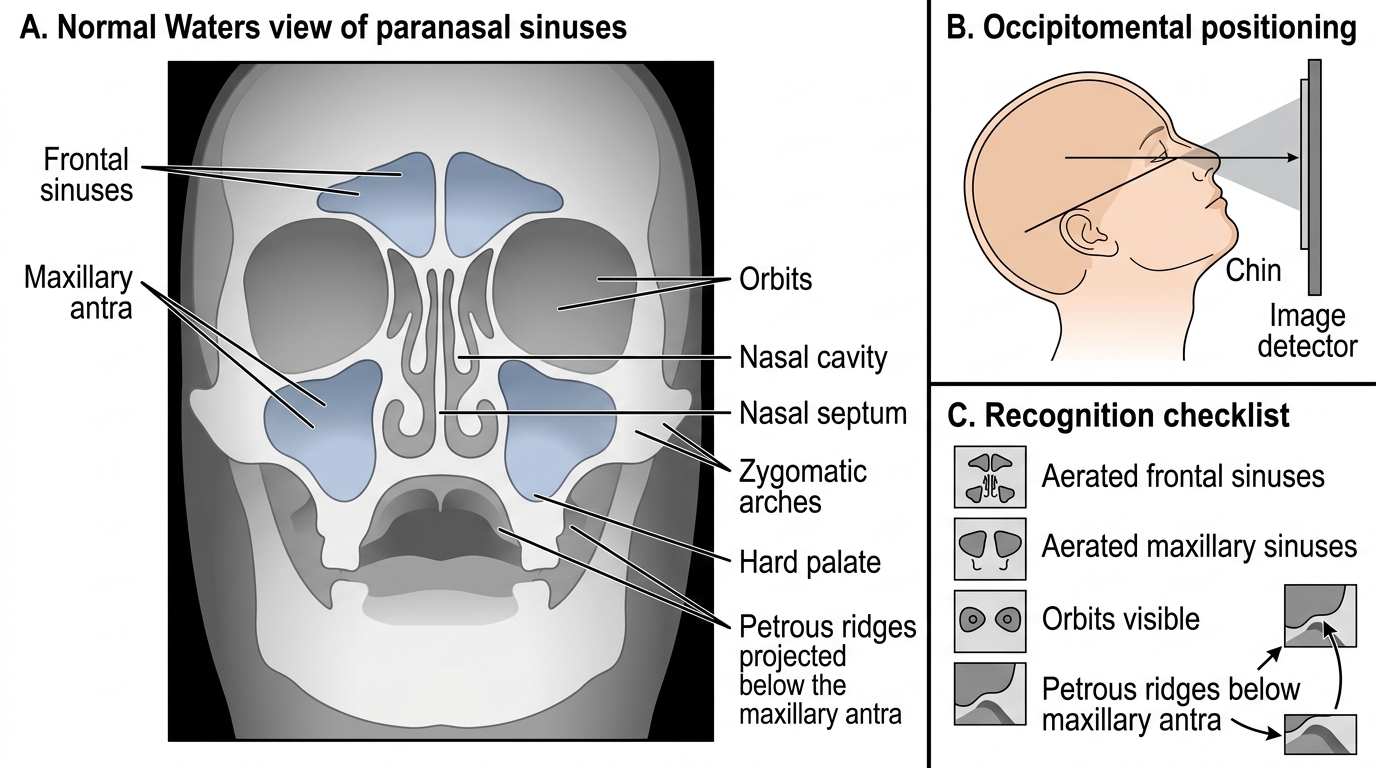
Normal Waters View of the Paranasal Sinuses
SELF-CHECK
A portable supine AP chest radiograph of an adult ICU patient shows a cardiothoracic ratio that appears to be about 0.55. The lungs are clear and the patient has no clinical signs of heart failure. What is the most appropriate interpretation?
A. Cardiomegaly is confirmed; request an urgent echocardiogram
B. The apparent enlargement may be due to AP/supine magnification; cardiothoracic ratio cannot be reliably assessed on an AP film
C. The film proves a pericardial effusion
D. The cardiothoracic ratio is normal because <0.6 is the cut-off on any projection
Reveal Answer
Answer: B. The apparent enlargement may be due to AP/supine magnification; cardiothoracic ratio cannot be reliably assessed on an AP film
The cardiothoracic ratio <0.5 cut-off applies to a PA erect film. On an AP or supine portable film the heart is farther from the detector and is magnified, so the cardiac shadow appears larger and the mediastinum wider. You cannot diagnose cardiomegaly from an AP film; the finding must be confirmed on a PA film or by echocardiography correlated with clinical signs. The 0.6 'cut-off on any projection' is incorrect.