Page 2 of 17
RD7.3 | CT Brain in Stroke — SDL Guide (Part 2)
Impact on Diagnosis and Management — Thrombolysis, Thrombectomy and Beyond
The clinical power of CT brain in stroke lies precisely in how directly its findings translate into treatment decisions, often within the same hour of imaging. No other investigation in hospital medicine is more directly tied to an immediate, time-critical therapeutic action than the NCCT brain in a potential stroke — the result gates one of the most effective neurological treatments available. Three major management pathways pivot on the CT result, and understanding this chain of imaging-to-decision is the applied core of RD7.3.
Pathway 1 — IV thrombolysis (alteplase):
Once NCCT confirms NO haemorrhage and NO established large-core infarct, the patient with a clinically confirmed ischaemic stroke is assessed for IV alteplase eligibility. The standard window is onset to needle time ≤4.5 hours (AHA/ASA 2019 extended from the original 3-hour window). Key eligibility criteria include:
- NCCT: no haemorrhage; early ischaemic changes may be present but extensive early infarct (ASPECTS ≤6 or >1/3 MCA territory involvement on CT) increases haemorrhagic transformation risk.
- BP must be <185/110 mmHg before and maintained <180/105 mmHg after infusion.
- No recent surgery, active bleeding, prior stroke, or coagulation disorder as per contraindications.
The dose is alteplase 0.9 mg/kg IV (max 90 mg), with 10% as bolus and 90% over 60 minutes.
Pathway 2 — Mechanical thrombectomy (MT):
When CTA (performed after NCCT) identifies a large-vessel occlusion (LVO) — typically proximal MCA (M1/M2), ICA, or basilar artery — the patient is assessed for mechanical thrombectomy regardless of whether thrombolysis is given. MT is effective up to:
- 6 hours from onset for patients meeting standard NCCT criteria.
- Up to 24 hours in selected patients with significant penumbra by CTP or MRI mismatch (DAWN trial: clinical-imaging mismatch; DEFUSE 3 trial: perfusion mismatch). These extended-window patients MUST be screened with CT perfusion or MRI — not NCCT alone.
Pathway 3 — Supportive care and secondary prevention:
Patients who are outside the thrombolysis window, or who have haemorrhagic stroke, receive supportive management. CT guides the initial trajectory:
- In ICH: blood pressure control (target <140 mmHg systolic in the first hour per AHA/ASA 2022 ICH guidelines), neurosurgical evaluation for evacuation (lobar haematoma >30 mL with deteriorating GCS), and reversal of anticoagulation.
- In ischaemic stroke outside the window: antiplatelet therapy (aspirin 300 mg loading in the first 24–48 hours when haemorrhage is excluded), statin initiation, blood pressure and glucose management, and early secondary-prevention workup (cardiac monitoring, carotid duplex, lipid profile).
What CT cannot do well: CT is insensitive for infarcts in the first 6 hours (early signs are subtle), posterior-fossa infarcts (beam-hardening artefact from the petrous bones reduces posterior-fossa resolution), and small lacunar infarcts (better on MRI-FLAIR/DWI). When CT is negative but the clinical presentation is convincing for stroke, MRI with DWI is the next step.
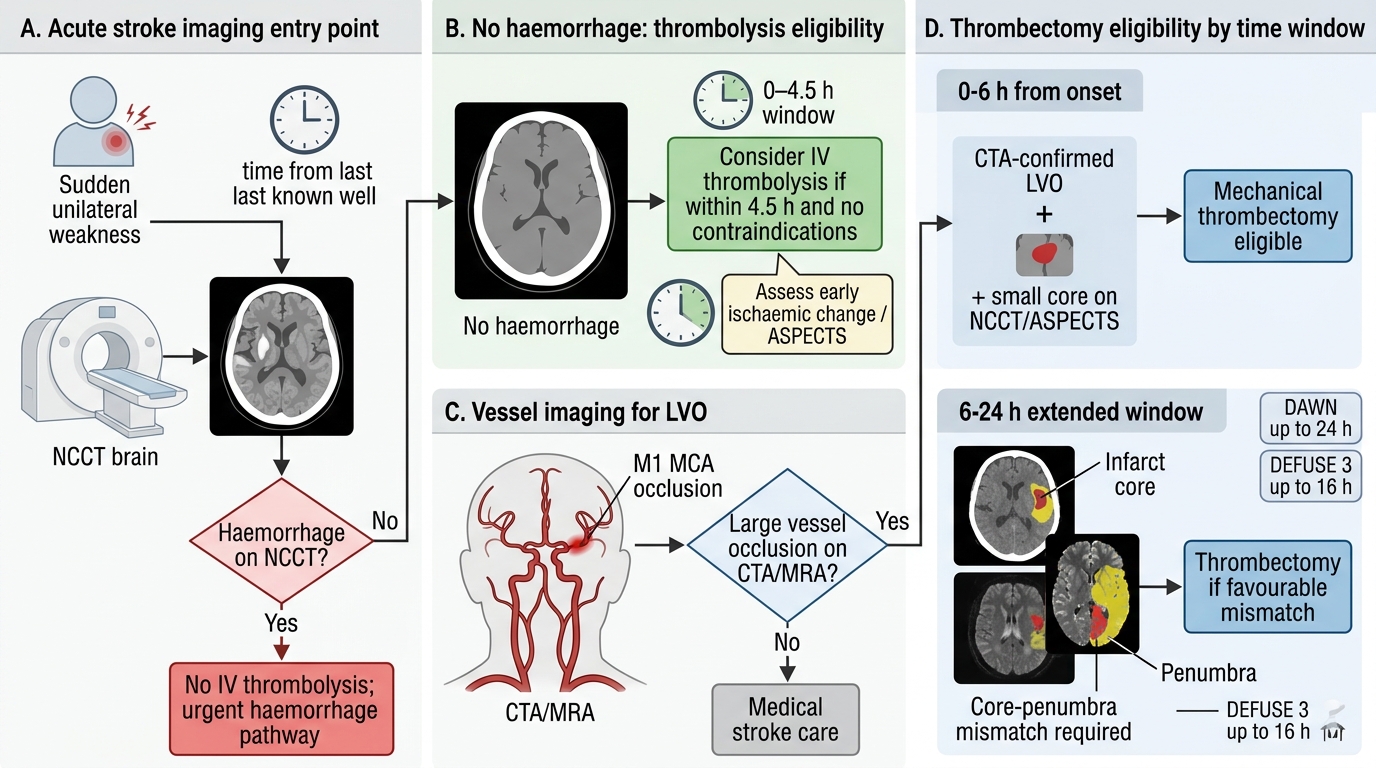
Acute Stroke Imaging and Reperfusion Decision Pathway
SELF-CHECK
A 67-year-old man presents 7 hours after onset of right-sided weakness. NCCT brain shows no haemorrhage and subtle loss of grey-white differentiation in the left MCA territory (ASPECTS 7). CTA shows left M1 MCA occlusion. What is the MOST appropriate next step in imaging to determine thrombectomy eligibility?
A. No further imaging; CT angiography confirms LVO and standard thrombectomy eligibility extends to 24 hours for all LVO patients
B. CT perfusion or MRI with DWI to assess ischaemic core vs penumbra mismatch — required for extended window eligibility beyond 6 hours
C. Repeat NCCT at 12 hours to determine if the infarct has progressed before deciding
D. Catheter angiography as the only definitive method to determine perfusion status
Reveal Answer
Answer: B. CT perfusion or MRI with DWI to assess ischaemic core vs penumbra mismatch — required for extended window eligibility beyond 6 hours
The DAWN and DEFUSE 3 trials demonstrated mechanical thrombectomy benefit up to 24 hours (DAWN) and 16 hours (DEFUSE 3) in patients with LVO AND a favourable imaging mismatch — meaning significant penumbra (salvageable tissue) relative to the infarct core. This mismatch is measured by CT perfusion or MRI DWI/perfusion. CTA alone identifies LVO but does not quantify salvageable tissue. Beyond 6 hours, perfusion imaging is mandatory to select patients for MT; not all LVO patients in the extended window have salvageable penumbra.
CLINICAL PEARL
Pearl 1 — The hyperdense MCA sign: A hyperdense MCA is often the ONLY CT abnormality in the first 1–2 hours of a large MCA territory stroke — the brain itself may look normal. Always check the Sylvian fissure for asymmetric hyperdensity. Its presence should immediately prompt CTA for thrombectomy planning, even when other CT changes are absent.
Pearl 2 — CT vs MRI in the acute window: MRI-DWI is more sensitive than NCCT for early ischaemia — but it is NOT required for the thrombolysis decision. NCCT to exclude haemorrhage is sufficient. Insisting on MRI before thrombolysis in a hospital where MRI takes 45 minutes will cost the patient millions of neurons. The rule is: use the fastest reliable tool to answer the critical question, not the most sensitive tool available.
Pearl 3 — ASPECTS score matters: ASPECTS ≤6 on the pre-treatment CT identifies patients with large established infarct cores who have high risk of haemorrhagic transformation with reperfusion. Know the concept — it appears in viva and structured examinations, and it is the basis for thrombectomy patient selection in many trial protocols.
Self-Assessment — CT Stroke Decisions
Work through these scenarios as if you are the clinician on call. Write your reasoning before reading the discussion.
Scenario A: A 55-year-old man has sudden-onset global aphasia and right hemiplegia, 1 hour after onset. NCCT brain is normal. His neurological deficit is confirmed. Should thrombolysis be withheld because the CT is 'normal'?
Discussion: No. An NCCT brain that is normal in the first 1–2 hours is entirely consistent with acute ischaemic stroke — CT has low sensitivity for early infarction. The purpose of the NCCT is to EXCLUDE haemorrhage; once it is confirmed negative, and clinical eligibility criteria are met, thrombolysis proceeds. A negative CT does not mean no stroke. Obtain CTA simultaneously to check for LVO.
Scenario B: A 78-year-old woman presents 9 hours after waking up with left-sided weakness ('wake-up stroke' — exact onset unknown). NCCT shows no haemorrhage. CTA shows right M1 MCA occlusion. ASPECTS is 8 (two early ischaemic regions deducted). Should she receive thrombolysis? Can she receive thrombectomy?
Discussion: Thrombolysis is generally not given beyond 4.5 hours from known onset, and in wake-up stroke the onset is considered the last-seen-well time (when she went to sleep). However, CT perfusion (or MRI with DWI/PWI mismatch) can identify patients with significant salvageable penumbra who may benefit from mechanical thrombectomy under DAWN/DEFUSE 3 extended criteria (up to 24 hours from last-seen-well for DAWN). If perfusion imaging shows large penumbra and small core, MT is indicated. ASPECTS 8 (minimal established infarct) supports possible benefit.
Scenario C: A 45-year-old woman with no known comorbidities presents with sudden severe occipital headache and stiff neck, GCS 14/15. NCCT brain is ordered. What specific finding are you looking for and what is the next step if CT is negative?
Discussion: The presentation is classic for subarachnoid haemorrhage (SAH). On NCCT, look for hyperdensity in the basal cisterns, Sylvian fissures, and interhemispheric fissure. CT sensitivity for SAH is approximately 98% within 12 hours but declines thereafter (blood is isodense with CSF as it is metabolised). If CT is normal but clinical suspicion is high, lumbar puncture for xanthochromia (yellow discolouration of CSF due to haemoglobin breakdown products) is mandatory. CT angiography is then performed to identify the underlying aneurysm.