Page 7 of 17
RD7.3 | Imaging Findings in Cardiac Failure — SDL Guide
Learning Objectives
- Recognise the clinical presentations of heart failure and state the diagnostic questions that imaging is asked to answer (cardiomegaly, congestion, and ejection fraction).
- Justify the chest radiograph as the first-line bedside study and echocardiography as the key functional modality, and outline the advanced roles of cardiac MRI and lung ultrasound.
- Identify the chest-radiograph signs of pulmonary venous congestion and correlate them with rising pulmonary capillary pressure.
- Use the echocardiographic ejection fraction to classify heart failure (HFrEF, HFmrEF, HFpEF) and link the classification to management.
- Integrate imaging findings into the diagnosis and management of heart failure, including distinguishing cardiogenic from non-cardiogenic pulmonary oedema.
INSTRUCTIONS
Heart failure is a clinical syndrome, but its diagnosis, classification and monitoring depend heavily on imaging. The chest radiograph provides an immediate bedside read on cardiac size and pulmonary congestion, while echocardiography supplies the single most important piece of functional information — the ejection fraction — that determines treatment. As a final-year student and future clinician, you will order and interpret these studies constantly on the wards and in casualty. This module teaches you how to read the imaging of heart failure, how its findings map onto the underlying haemodynamics, and how those findings drive management — the applied focus of competency RD7.3.
References
- Sutton's Textbook of Radiology, 6th edition, Chapter on Cardiac and Cardiothoracic Imaging (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter on the Heart and Pulmonary Circulation (textbook)
- ESC 2021 Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure (guideline)
- ACC/AHA/HFSA 2022 Guideline for the Management of Heart Failure (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 68-year-old man is brought to casualty at midnight, sitting bolt upright, gasping for breath, with frothy pink sputum and crackles to the mid-zones. The intern reaches for a CT scan to 'find the cause'. But the two investigations that will actually change the next hour of this man's care are far simpler: a portable chest radiograph and a bedside echocardiogram. The chest X-ray will, within minutes, confirm the cardiomegaly and the bat-wing alveolar oedema of acute pulmonary oedema and let diuresis begin; the echo will reveal whether his ejection fraction is severely reduced or preserved, which determines the long-term drugs that prevent his next admission. In heart failure, the highest-yield imaging is not the most advanced — it is the radiograph at the bedside and the echocardiogram that quantifies function. Knowing how to read both, and what they mean for treatment, is the difference between effective resuscitation and aimless investigation.
WHY THIS MATTERS
Heart failure is one of the commonest reasons for medical admission and re-admission, and its prevalence rises steeply with age, hypertension, ischaemic heart disease and diabetes — all increasingly common in India. The clinical features (breathlessness, orthopnoea, fatigue, oedema) overlap with respiratory and renal disease, so imaging is essential both to confirm the syndrome and to classify it. The NMC competency RD7.3 requires you to integrate imaging findings into the management of cardiac failure in the internal medicine setting — and this is a genuinely daily task. Every acute breathless patient needs a chest radiograph interpreted for congestion; every confirmed heart-failure patient needs an echocardiogram to measure the ejection fraction, because the entire structure of modern guideline-directed therapy is built on whether that fraction is reduced or preserved. Reading these studies competently is a core internal-medicine and emergency skill, not a radiology specialism.
RECALL
Before reading further, recall the following foundations from your earlier years:
- Starling forces and pulmonary oedema (from physiology): fluid moves out of pulmonary capillaries when capillary hydrostatic pressure rises. In left heart failure, the failing left ventricle raises left atrial and therefore pulmonary capillary pressure; once this exceeds the plasma oncotic pressure, fluid floods first the interstitium and then the alveoli — the physiological basis of every radiographic sign of congestion.
- Left versus right heart failure (from IM): left heart failure produces pulmonary congestion (breathlessness, orthopnoea, crackles); right heart failure produces systemic congestion (raised JVP, hepatomegaly, peripheral oedema). Many chronic patients have both (congestive cardiac failure).
- Ejection fraction (EF): the proportion of end-diastolic blood volume ejected per beat, normally about 55–70%. A reduced EF reflects impaired systolic contraction; failure can also occur with a normal EF when the ventricle cannot relax and fill properly (diastolic dysfunction).
- The cardiothoracic ratio (CTR): on an erect frontal (PA) chest radiograph, the ratio of the maximum transverse cardiac diameter to the maximum internal thoracic diameter; normally up to 0.5. It is the simplest radiographic index of heart size.
Clinical Scenario — Suspected Heart Failure and the Role of Imaging
Imaging in heart failure is driven entirely by the clinical questions the syndrome raises, and the first task is to be clear about what those questions are before requesting any study. A patient presenting with breathlessness, orthopnoea, paroxysmal nocturnal dyspnoea, fatigue or peripheral oedema may have heart failure — but the clinician needs imaging to answer three specific questions: is the heart enlarged, is there pulmonary congestion, and how well is the left ventricle actually pumping? Each of these is answered by a different modality, and recognising which question is being asked prevents both reflexive over-imaging and the failure to obtain the one study (the echocardiogram) that will define the patient's treatment for years. This disciplined mapping of clinical question to imaging modality is precisely the integrative reasoning competency RD7.3 expects in the internal-medicine department.
The clinical presentations that prompt heart-failure imaging include:
- Acute pulmonary oedema: sudden severe breathlessness, orthopnoea, frothy sputum, widespread crackles — a medical emergency.
- Chronic exertional breathlessness and fatigue with reduced exercise tolerance, often with a history of hypertension or ischaemic heart disease.
- Fluid overload: peripheral oedema, raised jugular venous pressure, and weight gain.
- A new murmur or cardiomegaly found incidentally, prompting assessment of structure and function.
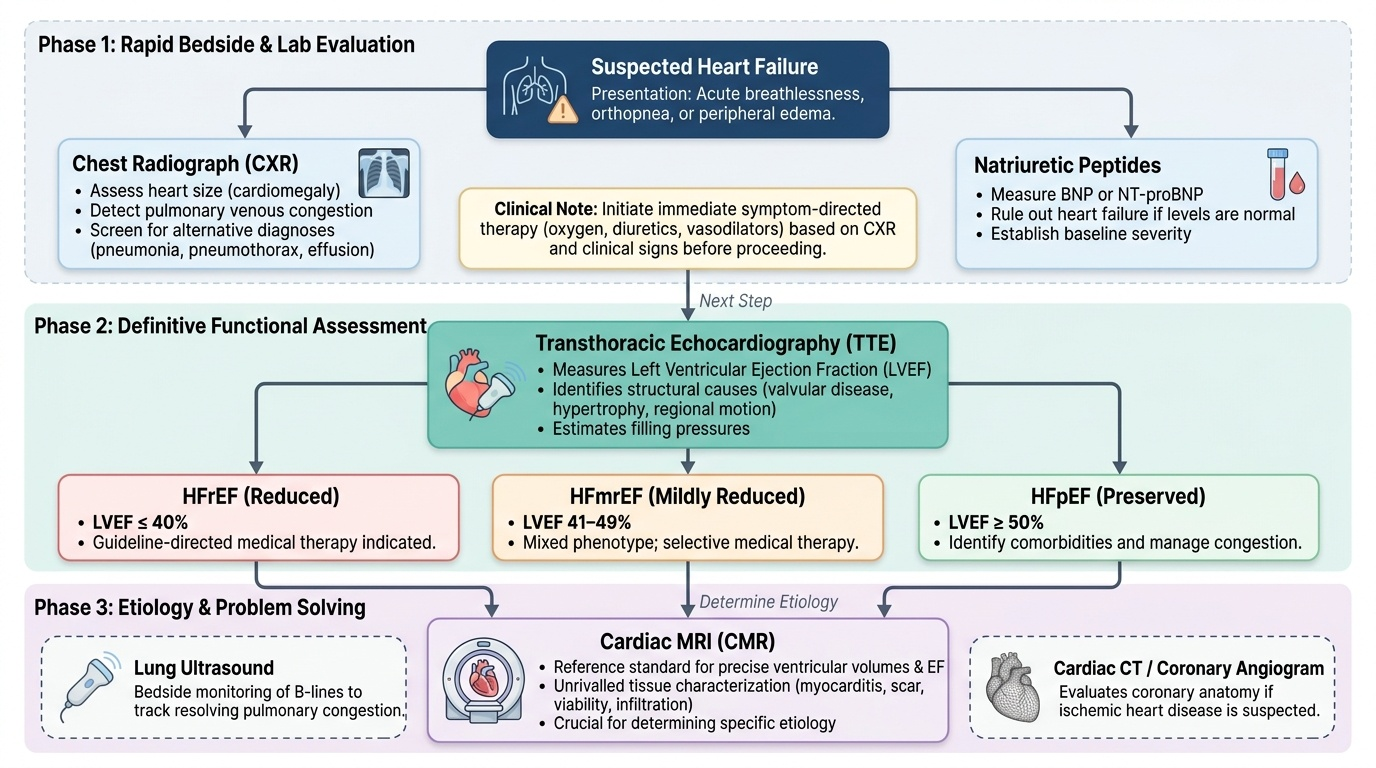
The role of imaging in these presentations is complemented by natriuretic peptides (BNP / NT-proBNP): a normal level makes heart failure unlikely and can reduce the need for urgent echocardiography, while a raised level supports the diagnosis and prioritises imaging. The two imaging studies that answer the core questions are the chest radiograph (cardiomegaly and congestion) and transthoracic echocardiography (the ejection fraction and the structural cause). Understanding that these two studies, used together, answer most clinical questions in heart failure — and that advanced imaging is reserved for specific problem-solving — is the foundation of a rational imaging strategy.
Imaging Strategy — CXR First, Echocardiography for Function
The imaging strategy in heart failure follows a logical sequence in which a fast, universally available study answers the immediate questions and a more sophisticated study answers the question that determines long-term therapy. The chest radiograph and the echocardiogram are complementary, not competing: the radiograph is a rapid bedside snapshot of heart size and lung congestion that can be obtained in the resuscitation room within minutes, whereas the echocardiogram is the definitive functional study that measures the ejection fraction and characterises the structural cause. Reserving the advanced modalities — cardiac MRI, CT, and lung ultrasound — for specific indications keeps the pathway efficient. Reasoning through this hierarchy, rather than ordering a battery of tests, is the strategic skill at the centre of competency RD7.3.
Chest radiograph (CXR) — first-line, bedside:
The CXR is fast, portable and available everywhere. In the acutely breathless patient it immediately shows cardiomegaly and the signs of pulmonary venous congestion, allowing congestion-directed treatment (diuresis, oxygen, vasodilators) to begin before any other test returns. It also screens for alternative or contributory diagnoses such as pneumonia, pneumothorax or a large pleural effusion. Its limitation is that it cannot measure cardiac function.
Transthoracic echocardiography — the key functional modality:
Echocardiography is the central investigation in heart failure because it measures the left-ventricular ejection fraction (LVEF) and thereby classifies the patient into HFrEF (reduced, LVEF <40%), HFmrEF (mildly reduced, 41–49%) or HFpEF (preserved, ≥50%). It also identifies the structural cause (valvular disease, regional wall-motion abnormality from prior infarction, hypertrophy, pericardial effusion) and estimates filling pressures. Because guideline-directed medical therapy is selected according to the EF category, the echocardiogram is indispensable.
Advanced and adjunct modalities (problem-solving):
These are reserved for specific questions rather than routine use.
- Cardiac MRI is the reference standard for ventricular volumes and EF and is unrivalled for tissue characterisation (myocarditis, infiltration, scar/viability), guiding aetiology-specific treatment.
- Lung ultrasound at the bedside detects B-lines, a rapid sign of interstitial pulmonary congestion useful for monitoring decongestion.
- CT (including coronary CT angiography) assesses coronary disease as an underlying cause and clarifies structural anatomy; iodinated contrast is generally avoided when the eGFR is below 30 mL/min/1.73m².
Provided image
SELF-CHECK
A 72-year-old woman is admitted with acute breathlessness and a chest radiograph showing cardiomegaly with bat-wing alveolar oedema. After initial diuresis she stabilises. Which investigation is most important to guide her long-term heart-failure therapy?
A. A repeat chest radiograph to confirm resolution of the oedema
B. Transthoracic echocardiography to measure the left-ventricular ejection fraction and classify the heart failure
C. Coronary CT angiography as the first functional test in all heart-failure patients
D. A natriuretic peptide (BNP) level, which provides the ejection fraction
Reveal Answer
Answer: B. Transthoracic echocardiography to measure the left-ventricular ejection fraction and classify the heart failure
The chest radiograph confirmed congestion and guided acute treatment, but it cannot measure cardiac function. Transthoracic echocardiography is the key functional modality: it measures the left-ventricular ejection fraction and classifies the patient as HFrEF (<40%), HFmrEF (41–49%) or HFpEF (≥50%), which determines guideline-directed medical therapy. BNP supports or refutes the diagnosis but does not give the ejection fraction. Coronary CT angiography assesses coronary disease as a cause but is not the routine first functional test for classifying heart failure.
Imaging Findings — CXR Signs of Failure and Echo Parameters
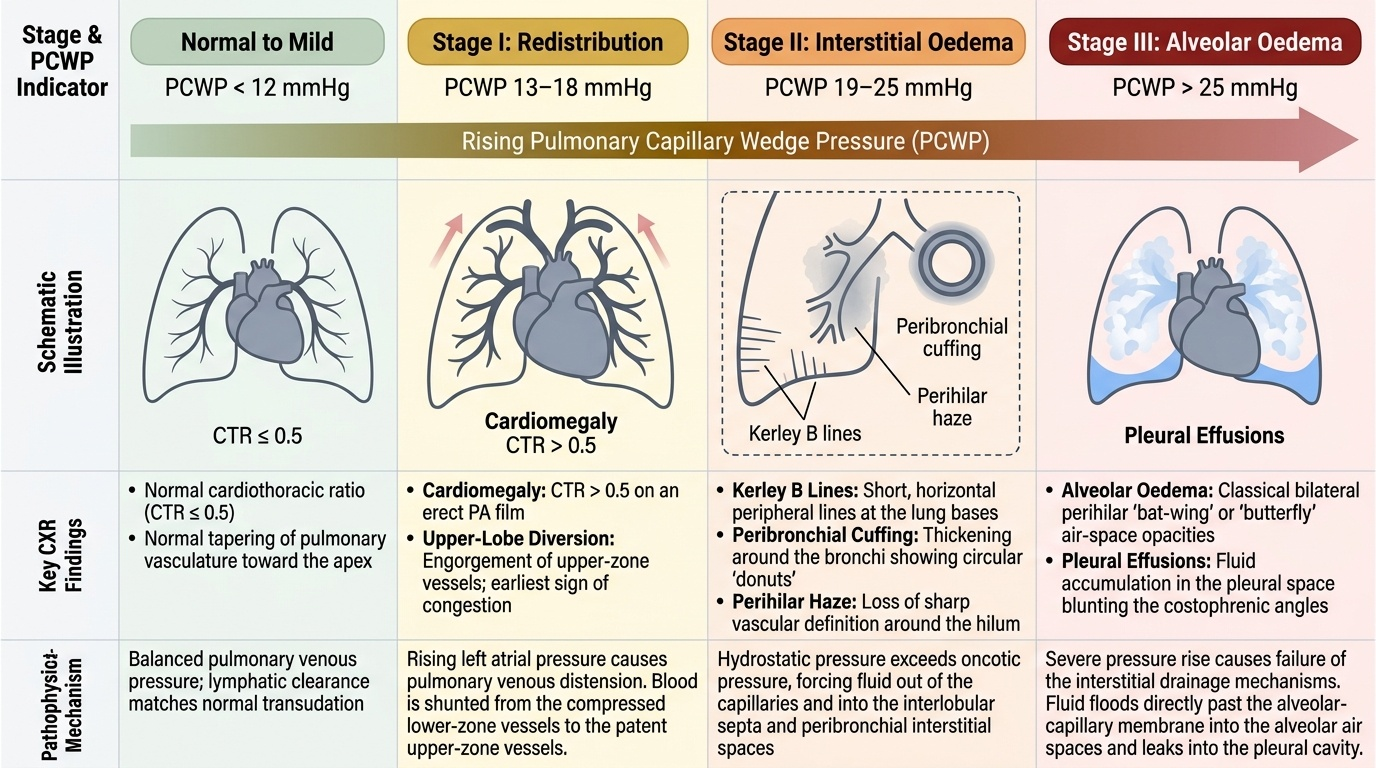
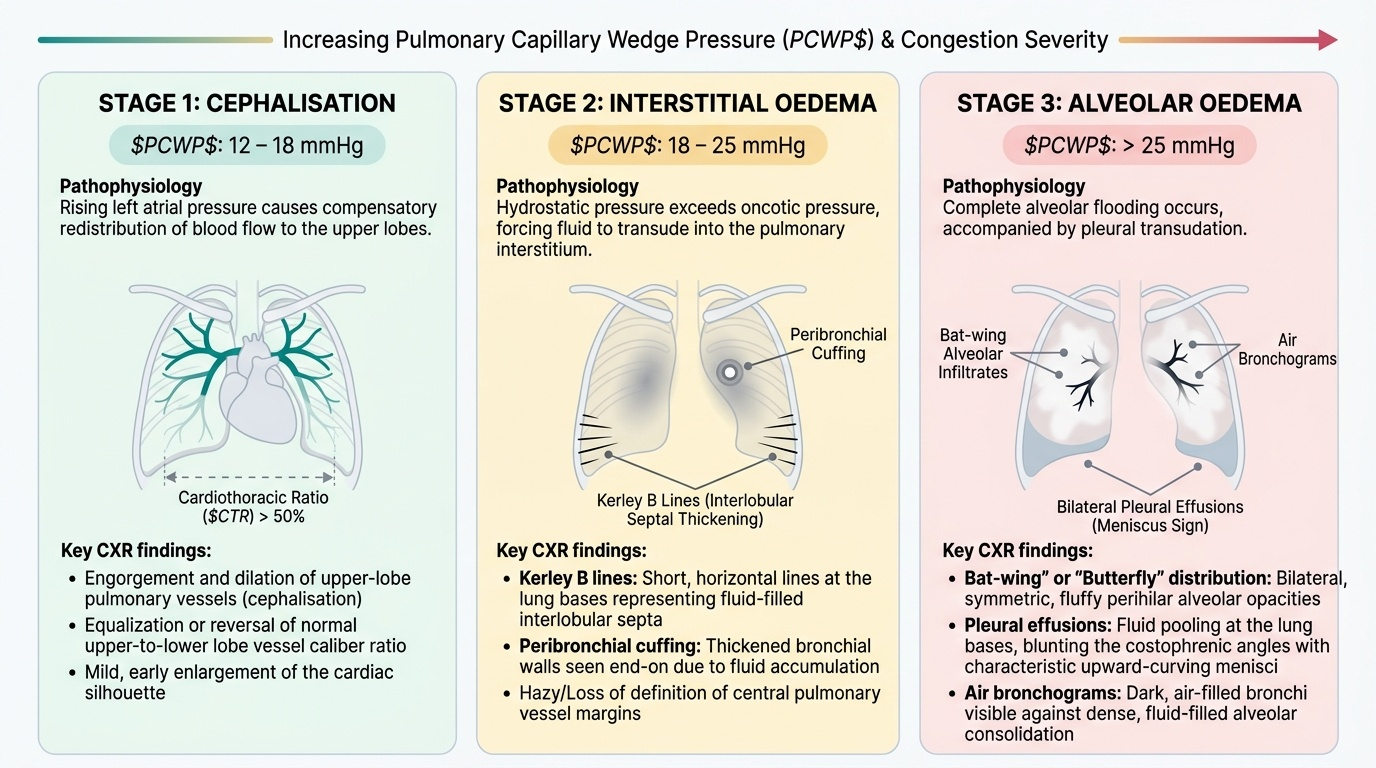
The chest-radiograph signs of heart failure are best understood not as a random list to memorise but as a staged sequence that maps directly onto rising pulmonary venous (capillary wedge) pressure — recognising this progression lets you estimate the severity of congestion from the film alone. As the failing left ventricle raises left atrial pressure, fluid is redistributed and then leaks in a predictable order: first the upper-lobe vessels engorge, then interstitial fluid appears, and finally the alveoli flood. Reading the radiograph as a record of this haemodynamic cascade, and pairing it with the echocardiographic measurement of pump function, gives a complete imaging picture of heart failure. Interpreting these findings in terms of their underlying mechanism is exactly the integrative competence that RD7.3 demands of the internal-medicine clinician.
Provided image
Chest-radiograph signs (in order of rising pulmonary venous pressure):
1. Cardiomegaly: a cardiothoracic ratio greater than 0.5 on an erect PA film — the structural marker of an enlarged or failing heart.
2. Upper-lobe blood diversion (cephalisation): the normally inconspicuous upper-zone vessels become as prominent as, or more prominent than, the lower-zone vessels as pressure rises — the earliest congestion sign.
3. Kerley B lines: short, horizontal, peripheral lines at the lung bases representing fluid in the interlobular septa (interstitial oedema).
4. Peribronchial cuffing and perihilar haze: thickening around the bronchi and loss of vascular definition, indicating interstitial fluid.
5. Alveolar (bat-wing / butterfly) oedema: bilateral perihilar air-space opacification as fluid floods the alveoli — the sign of severe acute pulmonary oedema.
6. Pleural effusions: often bilateral (or right-sided if unilateral), reflecting elevated venous pressure and fluid overload.
Echocardiographic parameters:
The echocardiogram quantifies the pump and characterises the structural cause:
- Left-ventricular ejection fraction (LVEF): the central measurement, classifying the patient into HFrEF (<40%), HFmrEF (41–49%) or HFpEF (≥50%).
- Chamber size and wall motion: a dilated, globally hypokinetic ventricle suggests dilated cardiomyopathy; a regional wall-motion abnormality suggests prior myocardial infarction.
- Valvular and diastolic assessment: significant valve lesions and indices of diastolic dysfunction and elevated filling pressures (important in HFpEF, where the EF is normal).
Lung ultrasound: multiple B-lines (vertical comet-tail artefacts) indicate interstitial pulmonary congestion and allow rapid bedside monitoring of decongestion.
Provided image
SELF-CHECK
On the chest radiograph of a patient with acute heart failure, you note that the upper-zone pulmonary vessels are more prominent than the lower-zone vessels. What does this sign represent, and where does it sit in the progression of congestion?
A. Alveolar oedema; it is the most severe and latest radiographic sign
B. Upper-lobe blood diversion (cephalisation); it is an early sign of rising pulmonary venous pressure
C. Kerley B lines; they represent fluid in the alveoli
D. Pleural effusion; it indicates the heart is not enlarged
Reveal Answer
Answer: B. Upper-lobe blood diversion (cephalisation); it is an early sign of rising pulmonary venous pressure
Prominence of the upper-zone vessels relative to the lower zones is upper-lobe blood diversion (cephalisation), one of the earliest radiographic signs of rising pulmonary venous (capillary wedge) pressure. As pressure rises further, interstitial signs appear (Kerley B lines, peribronchial cuffing) and finally alveolar (bat-wing) oedema floods the air spaces — the latest and most severe sign. Kerley B lines are interstitial (interlobular septal fluid), not alveolar, and a pleural effusion does not indicate normal heart size.