Page 10 of 17
RD7.3 | Imaging in Liver Parenchymal Disease — SDL Guide
Learning Objectives
- Recognise the clinical situations (deranged liver function, suspected fatty liver, chronic liver disease, surveillance) that prompt liver parenchymal imaging.
- Justify ultrasonography as the first-line modality and outline the roles of transient elastography, multiphasic CT and MRI.
- Describe the ultrasound appearances of fatty liver, cirrhosis and portal hypertension, and the imaging features of hepatocellular carcinoma.
- Integrate imaging findings into the management of liver parenchymal disease, including the 6-monthly surveillance protocol for hepatocellular carcinoma in cirrhosis.
- Apply contrast-safety principles (iodinated contrast and gadolinium cautions in renal impairment) to the selection of cross-sectional liver imaging.
INSTRUCTIONS
Diffuse liver parenchymal disease — from simple fatty liver through cirrhosis and portal hypertension to hepatocellular carcinoma — is extremely common and largely silent until late. Imaging is central to detecting it, staging it, surveilling for cancer and guiding treatment, and ultrasonography is almost always the entry point. As a final-year student and future clinician, you will request and interpret liver ultrasound constantly, and you must understand when to escalate to elastography, CT or MRI. This module teaches you the imaging strategy for liver parenchymal disease, the key appearances on each modality, and how those findings drive management — the applied focus of competency RD7.3.
References
- Sutton's Textbook of Radiology, 6th edition, Chapter on the Liver and Biliary System (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter on the Liver: Diffuse Disease and Tumours (textbook)
- EASL Clinical Practice Guidelines on the Management of Hepatocellular Carcinoma (guideline)
- AASLD Practice Guidance on HCC Surveillance and the LI-RADS reporting system (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 52-year-old man with type 2 diabetes and a high body-mass index attends a routine clinic. His liver enzymes are mildly raised and the consultant orders an abdominal ultrasound. The report comes back: 'bright liver, increased echogenicity, loss of hepatorenal contrast — consistent with fatty liver.' To the casual reader this seems a benign, almost incidental finding. But this single ultrasound has opened a door onto a disease spectrum that can progress silently from fatty liver to steatohepatitis, to cirrhosis, to hepatocellular carcinoma — and the imaging pathway chosen from here determines whether that progression is caught early or missed. Ultrasound is the inexpensive, radiation-free workhorse that detects the problem; elastography quantifies the fibrosis; and multiphasic CT or MRI characterises any worrying nodule and underpins cancer surveillance. Knowing how to read the first ultrasound, and what to do next, is the difference between vigilant follow-up and a late, incurable diagnosis.
WHY THIS MATTERS
Chronic liver disease is a major and growing cause of morbidity and mortality, driven by viral hepatitis, alcohol, and the rising tide of metabolic (non-alcoholic) fatty liver disease that accompanies diabetes and obesity. Most of this disease is asymptomatic until complications appear, so imaging carries the burden of early detection and ongoing surveillance. The NMC competency RD7.3 requires you to integrate imaging findings into the management of liver parenchymal disease in the internal medicine setting — a genuinely everyday task. Deranged liver function tests almost always trigger an ultrasound; a diagnosis of cirrhosis mandates a structured surveillance programme for hepatocellular carcinoma; and new symptoms in a known liver patient demand imaging interpretation. Understanding which modality to use, what its findings mean, and how they change management is core internal-medicine and family-practice competence, not a niche radiological skill — and getting the surveillance pathway right directly saves lives by catching curable cancers early.
RECALL
Before reading further, recall the following foundations from your earlier years:
- Hepatic architecture and dual blood supply (from anatomy/physiology): the liver receives a dual blood supply — roughly 75% from the portal vein and 25% from the hepatic artery. This dual supply is the basis of multiphasic (arterial, portal-venous, delayed) contrast imaging, which exploits the different timing of enhancement to characterise lesions such as hepatocellular carcinoma.
- Cirrhosis (from pathology): the end stage of chronic liver injury, characterised by diffuse fibrosis and regenerative nodules that distort the normal architecture — the structural change that produces the nodular surface and coarse echotexture seen on imaging.
- Portal hypertension (from pathology/IM): increased resistance to portal flow (most often from cirrhosis) raises portal venous pressure, opening portosystemic collaterals (oesophageal varices, recanalised umbilical vein), causing splenomegaly and ascites.
- Echogenicity (from radiology basics): on ultrasound, tissues that reflect more sound appear brighter (hyperechoic) and those that reflect less appear darker (hypoechoic). Normal liver is slightly more echogenic than the adjacent renal cortex; fat increases echogenicity, which is why a fatty liver becomes conspicuously 'bright'.
Clinical Scenario — When Liver Imaging Is Requested
Liver parenchymal imaging is requested to answer a small set of recurring clinical questions, and identifying which question is being asked is the first step in choosing the right study. Because diffuse liver disease is usually silent, imaging is frequently the first investigation that reveals it — most often an ultrasound prompted by an abnormal blood test rather than by symptoms. The clinician needs imaging to answer questions such as: is the liver fatty, is it cirrhotic, is there portal hypertension, and (in a patient with established cirrhosis) is there a new focal lesion that could be a cancer? Each of these questions maps onto a particular modality and a particular protocol, and recognising the clinical trigger ensures that the patient enters the correct imaging pathway rather than receiving a scattergun set of tests. This mapping of clinical scenario to imaging question is exactly the reasoning competency RD7.3 expects in the internal-medicine department.
The clinical situations that commonly prompt liver parenchymal imaging include:
- Deranged liver function tests: an incidental or investigated rise in transaminases or other liver enzymes, the commonest trigger for a first ultrasound.
- Suspected fatty liver disease: a patient with metabolic risk factors (obesity, type 2 diabetes, dyslipidaemia) or alcohol use.
- Known or suspected chronic liver disease / cirrhosis: assessment of the parenchyma, the spleen, and the portal system for evidence of advanced disease and portal hypertension.
- Surveillance in established cirrhosis: structured screening for hepatocellular carcinoma.
- New symptoms or signs in a liver patient: ascites, jaundice, abdominal pain, or weight loss requiring characterisation.
The reason ultrasonography is the entry point for almost all of these is that it is widely available, inexpensive, uses no ionising radiation, requires no contrast, and provides real-time assessment of the liver parenchyma, the spleen, the gallbladder and biliary tree, and — with Doppler — the direction and velocity of portal flow. It answers the screening questions directly and tells the clinician whether escalation to elastography, CT or MRI is needed. Understanding that the imaging journey almost always begins with ultrasound, and is then directed by its findings, is the foundation of a rational strategy for liver parenchymal disease.
Imaging Strategy — Ultrasound First, Then Elastography, CT and MRI
The imaging strategy for liver parenchymal disease is a staged escalation in which a single first-line modality screens and triages, and more specialised modalities are added only to answer the questions that ultrasound cannot fully resolve. Ultrasonography detects diffuse disease and most complications; elastography quantifies fibrosis non-invasively; and multiphasic CT and MRI characterise focal lesions and underpin cancer diagnosis and staging. This hierarchy keeps cost, radiation and contrast exposure proportionate to the clinical need, while ensuring that a worrying finding is always followed by the appropriate definitive test. Reasoning through this escalation — knowing when ultrasound is sufficient and when to move on — is the strategic competence at the heart of RD7.3 for hepatobiliary imaging.
Ultrasonography (USG) — first-line:
Ultrasound is the default first investigation for diffuse liver disease and the recommended tool for cancer surveillance. It is inexpensive, radiation-free, contrast-free, portable and real-time. It assesses parenchymal echogenicity (steatosis), surface contour and echotexture (cirrhosis), the spleen and ascites (portal hypertension), and — with Doppler — the patency, direction and velocity of portal and hepatic venous flow.
Transient elastography (FibroScan) and shear-wave elastography — fibrosis quantification:
These techniques measure liver stiffness as a non-invasive surrogate for fibrosis, allowing the degree of fibrosis to be staged and monitored without the need for biopsy in many patients. They are particularly valuable in fatty liver disease and chronic viral hepatitis to identify those progressing toward cirrhosis.
Multiphasic contrast CT and MRI — characterisation and surveillance:
When ultrasound finds a focal lesion or when complications/cancer must be characterised, multiphasic imaging exploits the liver's dual blood supply by scanning in arterial, portal-venous and delayed phases. Hepatocellular carcinoma characteristically shows arterial-phase hyperenhancement with washout on the portal-venous/delayed phases — the basis of the LI-RADS diagnostic criteria. MRI adds superior soft-tissue contrast and tissue characterisation. Contrast safety must be respected: iodinated contrast (CT) is generally avoided when the eGFR is below 30 mL/min/1.73m², and gadolinium (MRI) is used with caution in severe renal impairment.
HCC surveillance protocol:
In patients with cirrhosis, the recommended surveillance is abdominal ultrasound every 6 months, with or without serum alpha-fetoprotein (AFP) — a structured programme designed to detect tumours while they are small and potentially curable.
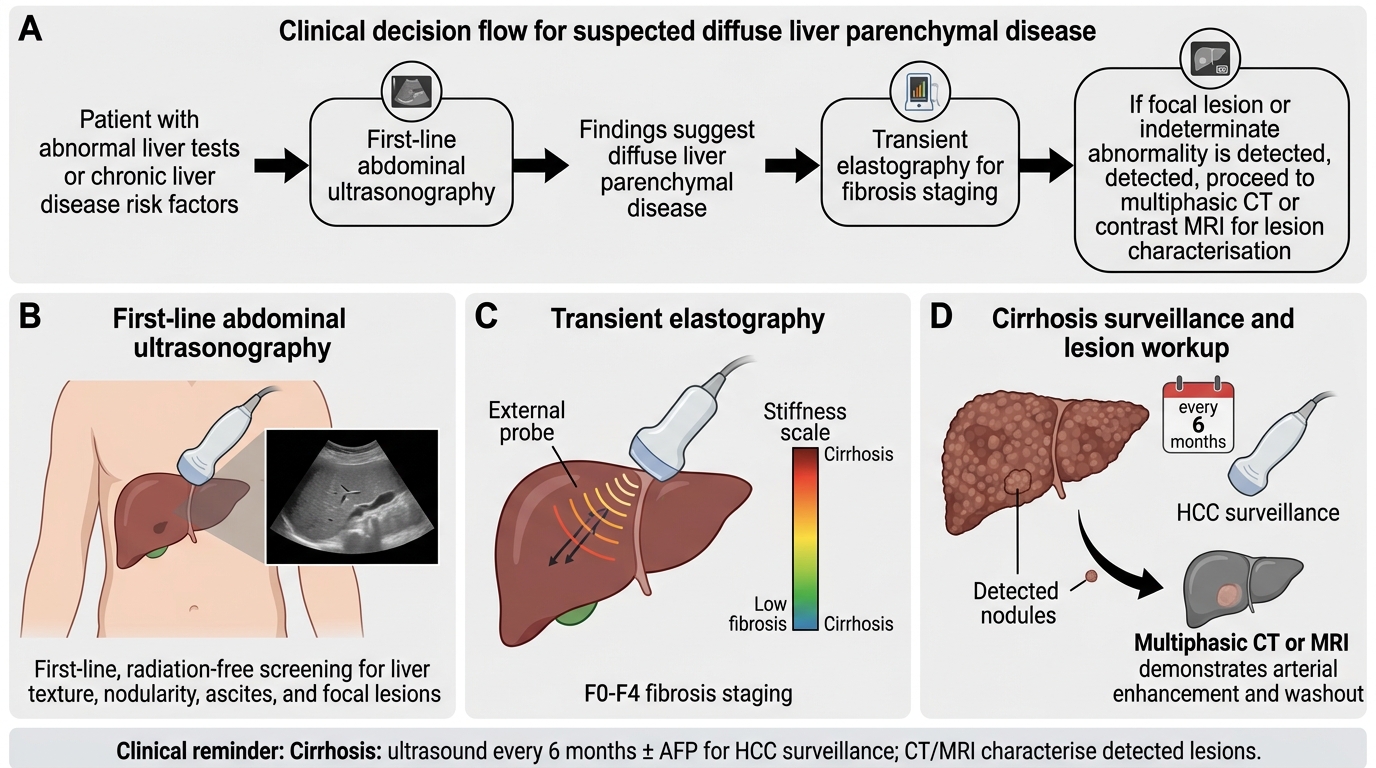
Imaging Pathway for Diffuse Liver Parenchymal Disease
SELF-CHECK
A 58-year-old man with compensated cirrhosis attends for routine follow-up. He has no new symptoms. According to standard guidance, what is the recommended imaging surveillance for hepatocellular carcinoma?
A. Annual multiphasic CT of the abdomen with iodinated contrast
B. Abdominal ultrasound every 6 months, with or without serum alpha-fetoprotein
C. Transient elastography every 3 months as the surveillance test
D. MRI of the liver only if he develops jaundice or weight loss
Reveal Answer
Answer: B. Abdominal ultrasound every 6 months, with or without serum alpha-fetoprotein
Standard guidance (AASLD/EASL) recommends surveillance for hepatocellular carcinoma in patients with cirrhosis using abdominal ultrasound every 6 months, with or without serum alpha-fetoprotein (AFP). Ultrasound is chosen because it is inexpensive, radiation-free and contrast-free, making it suitable for repeated long-term screening. Multiphasic CT and MRI are reserved for characterising lesions detected on surveillance, not for routine 6-monthly screening; transient elastography stages fibrosis but is not the cancer-surveillance test; and waiting for symptoms defeats the purpose of surveillance, which is to catch small curable tumours.
Imaging Findings — Fatty Liver, Cirrhosis and Portal Hypertension
Recognising the characteristic imaging appearances across the spectrum of liver parenchymal disease is a core interpretive skill, because each stage of the disease produces distinctive ultrasound signatures that follow directly from the underlying pathology. Fatty infiltration changes the way the liver reflects sound; established cirrhosis distorts its surface and internal texture; and portal hypertension produces a constellation of secondary signs in the spleen, the peritoneal cavity and the venous collaterals. Reading these appearances as the visible expression of the pathological process — rather than as isolated buzzwords — lets you interpret a report critically and anticipate the next step. Understanding why fat makes the liver bright, why fibrosis makes it nodular and coarse, and why portal hypertension enlarges the spleen and opens collaterals is exactly the integrative competence RD7.3 demands.
Provided image
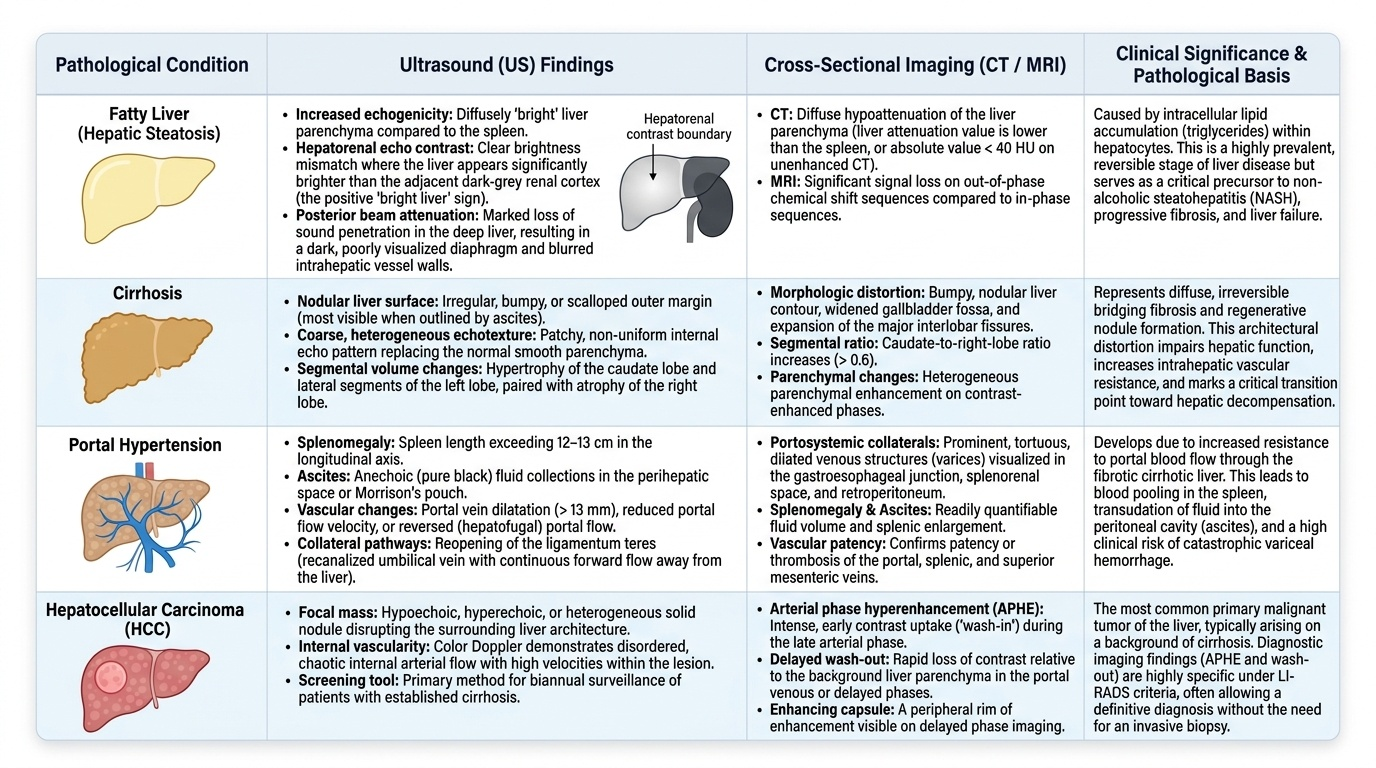
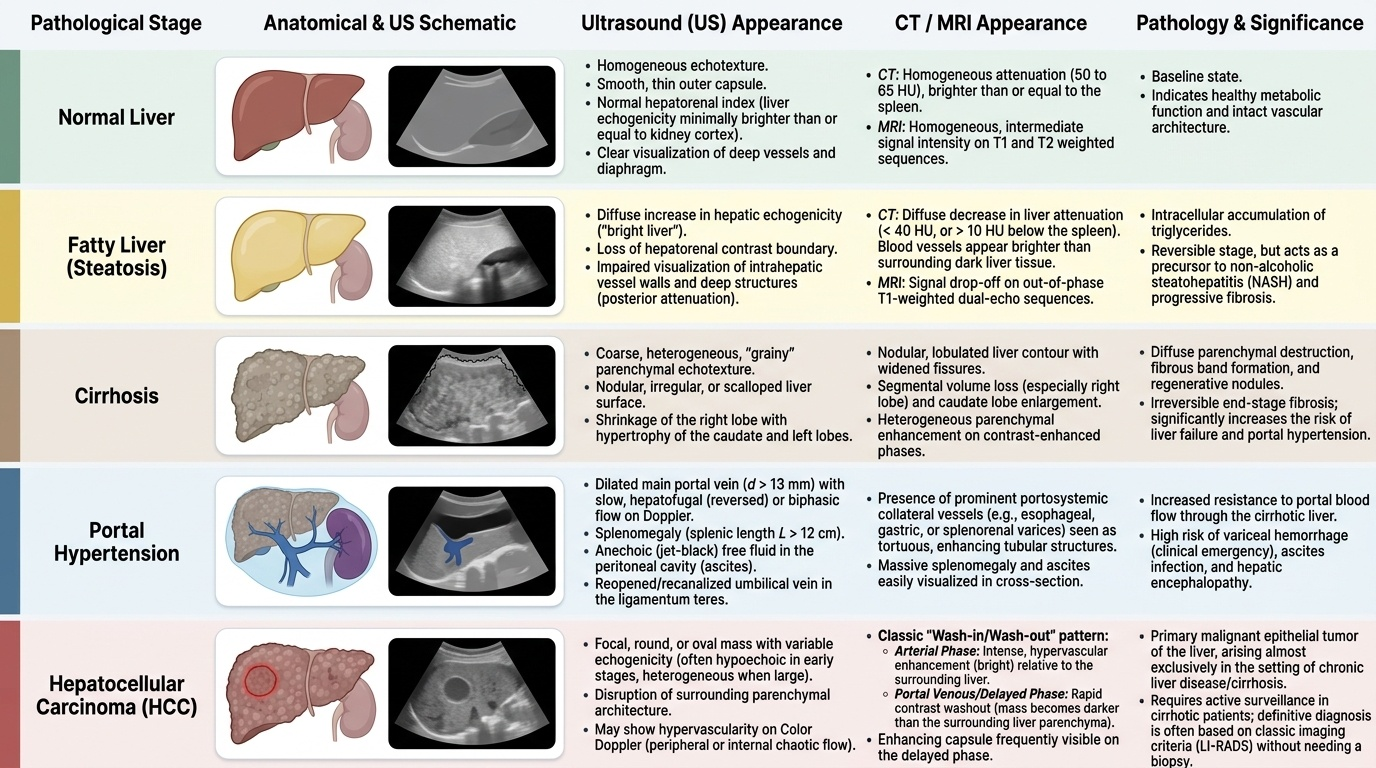
Fatty liver (hepatic steatosis) — ultrasound:
- Increased parenchymal echogenicity — the liver becomes diffusely 'bright' as fat increases sound reflection.
- Loss of the normal hepatorenal echo contrast — the liver appears brighter than the adjacent right renal cortex (the hepatorenal or 'bright liver' sign).
- Posterior beam attenuation with poor visualisation of the deep liver and diaphragm, and blurring of the intrahepatic vessel walls.
Cirrhosis — ultrasound:
- Nodular (irregular) liver surface — the visible result of regenerative nodules and fibrosis.
- Coarse, heterogeneous echotexture of the parenchyma.
- Segmental volume change — classically caudate-lobe hypertrophy with right-lobe atrophy, altering the overall liver shape.
Portal hypertension — ultrasound and Doppler:
- Splenomegaly and ascites (free fluid).
- Portosystemic collaterals, including a recanalised (patent) paraumbilical vein and splenorenal collaterals.
- Portal vein changes: dilatation of the main portal vein, reduced velocity, and in advanced disease reversed (hepatofugal) flow on Doppler.
Hepatocellular carcinoma (HCC) — focal lesion on a background of chronic liver disease:
- On ultrasound, a focal mass that may be hypo-, iso- or hyperechoic; any new nodule in a cirrhotic liver requires characterisation.
- On multiphasic CT/MRI, the hallmark is arterial-phase hyperenhancement followed by washout in the portal-venous/delayed phases — the basis of the imaging diagnosis without biopsy in the right clinical setting.
Provided image
SELF-CHECK
An ultrasound of a patient with metabolic risk factors shows a diffusely 'bright' liver that is more echogenic than the adjacent right renal cortex, with posterior beam attenuation. What is the most likely diagnosis and the basis of the appearance?
A. Cirrhosis; the brightness reflects regenerative nodules
B. Fatty liver (hepatic steatosis); fat increases parenchymal echogenicity and causes loss of the normal hepatorenal echo contrast
C. Portal hypertension; the brightness is due to splenomegaly
D. Hepatocellular carcinoma; the brightness is a focal arterial-enhancing mass
Reveal Answer
Answer: B. Fatty liver (hepatic steatosis); fat increases parenchymal echogenicity and causes loss of the normal hepatorenal echo contrast
A diffusely bright (hyperechoic) liver that is more echogenic than the right renal cortex, with posterior beam attenuation, is the classic ultrasound appearance of fatty liver (hepatic steatosis). Fat increases the reflection of sound, raising parenchymal echogenicity and abolishing the normal hepatorenal echo contrast (the 'bright liver' sign). Cirrhosis is characterised by a nodular surface and coarse echotexture rather than diffuse brightness; portal hypertension produces splenomegaly, ascites and collaterals; and HCC is a focal mass, not a diffuse change in echogenicity.