Page 10 of 17
RD7.6 | Breast Cancer Screening and Imaging in Management — SDL Guide
Learning Objectives
- State the role of mammography as the screening modality for breast cancer and the rationale for screening the asymptomatic woman.
- Choose the appropriate imaging modality by indication — mammography for screening, ultrasound for dense breasts/young women/pregnancy, and MRI for high-risk screening and staging.
- Explain the principle of triple assessment and how imaging fits within it.
- Describe the mammographic and ultrasound features that distinguish benign from malignant breast lesions and interpret the BI-RADS categories.
- Integrate the imaging findings (including the BI-RADS category) into the management pathway — biopsy, staging and treatment planning.
INSTRUCTIONS
Breast cancer is the commonest cancer in women in India and worldwide, and imaging sits at the centre of both its early detection and its management. As a final-year student you must understand why mammography is the screening test, when ultrasound or MRI is the better choice, what the BI-RADS category on a report means, and how the triple assessment combines clinical examination, imaging and pathology into a safe diagnosis. The competency RD7.6 asks you to integrate provided imaging findings into the screening and management of breast cancer patients — a skill you will use in surgery, family medicine and women's health. This module builds the reasoning that turns a breast imaging report into the next correct clinical step.
References
- Sutton's Textbook of Radiology and Imaging, 7th edition, Chapter on Breast Imaging (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter on the Breast (textbook)
- ACR BI-RADS Atlas (Breast Imaging Reporting and Data System), 5th edition (guideline)
- Bailey & Love's Short Practice of Surgery, Chapter on the Breast (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two women attend the breast clinic on the same morning. The first is 52, entirely well, and has come because she received a letter inviting her for routine breast screening; she has no symptoms and feels nothing abnormal. The second is 34 and has found a firm lump in her breast that she is frightened about. They have the same organ and overlapping fears, yet the right first imaging test for each is different — and getting that choice right matters enormously. Order the wrong test and you either miss an early cancer in the well woman or subject the young woman to an insensitive, anxiety-provoking study. Behind both encounters lies a single, learnable logic: which modality answers the question being asked, how its findings are reported in the standard BI-RADS language, and how that report becomes the next step in care.
WHY THIS MATTERS
Breast cancer is the most frequently diagnosed cancer in women, and its prognosis depends heavily on the stage at detection — early, screen-detected cancers carry a far better outlook than advanced symptomatic ones. Imaging is the backbone of early detection through screening mammography and of accurate diagnosis and staging once disease is suspected. The NMC competency RD7.6 requires you to integrate provided imaging findings into the screening for breast cancer and the management of breast cancer patients. This is directly applicable knowledge: you will counsel women about screening, assess breast lumps, read BI-RADS reports, and explain why a particular test was chosen. Understanding the modality choices, the BI-RADS system and the triple assessment is essential clinical competence in surgery, gynaecology and primary care, and it is consistently examined.
RECALL
Before reading further, recall:
- Breast anatomy and lymphatic drainage (from AN): the breast is composed of glandular lobules and ducts in a fibrofatty stroma; most cancers arise from the terminal duct-lobular unit. Lymphatic drainage is predominantly to the axillary nodes (and partly internal mammary nodes), which is why the axilla is central to staging.
- The concept of screening (from CM/PSM): screening detects disease in asymptomatic people before symptoms appear, aiming to reduce mortality through earlier treatment; it must use a sufficiently sensitive, acceptable, safe test in an appropriate population, and it carries recognised harms (false positives, overdiagnosis) that are weighed against benefit.
- Breast density: younger women have denser, more glandular breasts that appear white on a mammogram; because cancers are also white, mammographic sensitivity falls in dense breasts — the reason ultrasound is preferred in young women and dense breasts.
- Radiation safety (RD principle): mammography uses a low dose of ionising radiation; in young women, pregnancy and lactation, ultrasound (no ionising radiation) is preferred where it answers the question, in keeping with justification and ALARA.
Clinical Scenario — Screening the Well Woman and Assessing the Breast Lump
There are two distinct clinical scenarios in which breast imaging is requested, and distinguishing them is the first step in choosing the right test. The first is screening: imaging the asymptomatic, well woman to detect a cancer before it produces symptoms, with the goal of reducing breast-cancer mortality through earlier treatment. The second is the symptomatic presentation: a woman with a breast complaint — most often a lump, but also nipple discharge, skin or nipple change, or breast pain — in whom imaging is part of diagnosing the cause. The imaging question, and therefore the appropriate modality, differs between these two scenarios, and confusing them leads to the wrong test being ordered. Recognising which scenario you are in frames every subsequent decision in this module.
The two scenarios in more detail:
- Asymptomatic screening: offered to women in defined age ranges (programme-dependent — commonly around 50-69 in many national programmes, and from about 40 in others), using mammography as the screening test. The aim is to find small, impalpable cancers, often manifest only as microcalcifications, before they are clinically apparent.
- Symptomatic assessment (the breast lump and other symptoms): evaluated by triple assessment — clinical examination, imaging, and pathology (core biopsy or fine-needle aspiration cytology) — with the imaging modality chosen by age and breast density (mammography ± ultrasound in older women; ultrasound first in young women).
A crucial overarching principle binds both scenarios: imaging supports, but does not replace, the integrated clinical-pathological assessment. A normal mammogram does NOT exclude cancer in a woman with a clinically suspicious lump — this is why triple assessment exists, and why a discordant result (e.g. benign imaging but a worrying lump) is always pursued further rather than dismissed. Holding this principle prevents the dangerous error of false reassurance from a single negative test.
Imaging Strategy — Mammography for Screening, Ultrasound and MRI by Indication
The imaging strategy for the breast is built around matching the modality to the clinical indication and to the woman's age and breast density, while applying the radiation-safety principles that govern all of radiology. Each modality has a defined primary role, and choosing correctly between them is the practical substance of competency RD7.6. Mammography is the screening tool and the workhorse for older breasts; ultrasound characterises lesions and is the modality of choice where breast tissue is dense or radiation must be avoided; MRI offers the highest sensitivity for selected high-risk and staging situations. Understanding the rationale behind each choice — not just memorising a list — is what lets you justify the test you order and interpret the test you are handed.
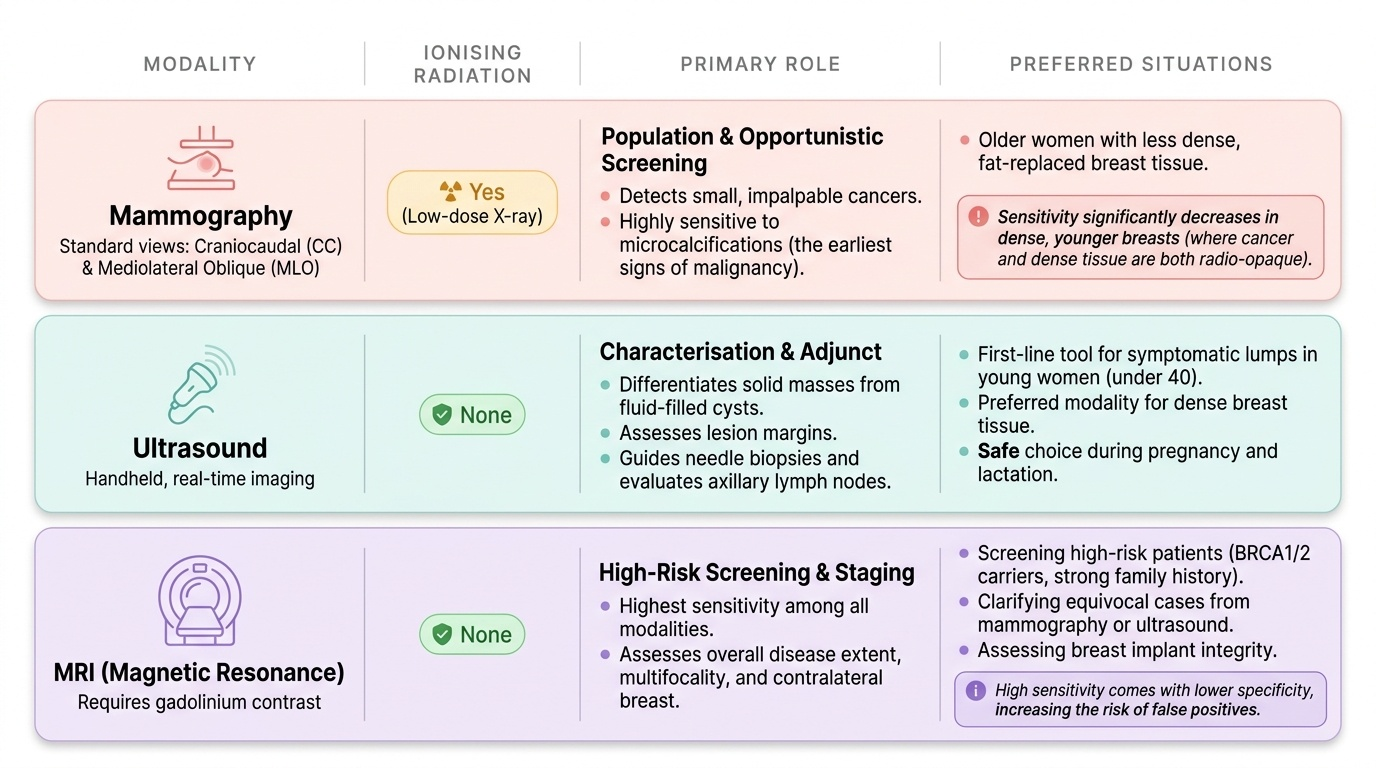
Mammography — the screening modality:
Mammography is a low-dose X-ray of the compressed breast, taken in standard views (craniocaudal and mediolateral oblique). It is the modality used for population and opportunistic screening because it can detect small impalpable cancers and, in particular, microcalcifications that may be the earliest sign of malignancy. Its sensitivity falls in dense (typically younger) breasts, where cancer and dense tissue are both radio-opaque.
Ultrasound — the adjunct and the modality of choice in specific groups:
Ultrasound uses no ionising radiation and excels at characterising a focal lesion as solid or cystic and at assessing its margins. It is the first-line imaging for a breast lump in a young woman (under about 40), the preferred modality in dense breasts, and the modality of choice in pregnancy and lactation. It is also used to guide needle biopsy and to assess the axillary nodes.
MRI — high sensitivity for selected indications:
Breast MRI (with gadolinium contrast) is the most sensitive modality and is used for screening high-risk women (e.g. BRCA1/BRCA2 mutation carriers and those with a strong family history), for assessing disease extent/staging (multifocality, the contralateral breast), for equivocal cases, and for implant assessment. It uses no ionising radiation but does use gadolinium, and its high sensitivity comes with lower specificity (false positives), so it is targeted rather than routine.
Triple assessment is the framework that integrates these: clinical examination + imaging + pathology (core biopsy or FNAC). A symptomatic lesion is assessed by all three, and concordance between them gives a reliable diagnosis; discordance is always pursued.
Modalities for staging, not primary detection: CT, bone scan and PET-CT are used to stage advanced disease (looking for distant metastases — lung, liver, bone), not to detect the primary tumour. Choosing CT to 'look at the breast' is incorrect.
Provided image
SELF-CHECK
A 33-year-old woman presents with a discrete, mobile breast lump. There is no family history of breast cancer. What is the most appropriate FIRST imaging modality, and why?
A. Mammography, because it is always the most sensitive breast imaging test regardless of age
B. Ultrasound, because in a young woman the breast tissue is dense (lowering mammographic sensitivity) and ultrasound, using no ionising radiation, reliably characterises a lump as solid or cystic
C. MRI, as the routine first test for any breast lump
D. CT of the chest, to look at the breast tissue in cross-section
Reveal Answer
Answer: B. Ultrasound, because in a young woman the breast tissue is dense (lowering mammographic sensitivity) and ultrasound, using no ionising radiation, reliably characterises a lump as solid or cystic
In a woman under about 40, breast tissue is dense, which reduces the sensitivity of mammography (cancer and dense tissue are both radio-opaque). Ultrasound is therefore the first-line imaging for a breast lump in a young woman: it uses no ionising radiation and reliably characterises the lesion as solid or cystic and assesses its margins, and it can guide biopsy. Mammography may be added if findings are suspicious; MRI is for high-risk screening/staging, and CT is for staging metastatic disease, not detecting the primary.
Expected Imaging Findings — Microcalcifications, Masses and the BI-RADS Language
Reading breast imaging means recognising the features that separate benign from malignant lesions and understanding the standardised language — BI-RADS — in which they are reported. The findings themselves are intuitive once the principle is grasped: benign lesions tend to look well-organised and contained, while malignant lesions tend to look infiltrative and disordered, because cancer invades surrounding tissue rather than respecting boundaries. Equally important is the BI-RADS system, because a breast report does not merely describe an appearance — it assigns an assessment category that carries an explicit management recommendation, and you must be able to translate that category into the next step. Reading the descriptive features and the BI-RADS category together is the interpretive skill RD7.6 builds.
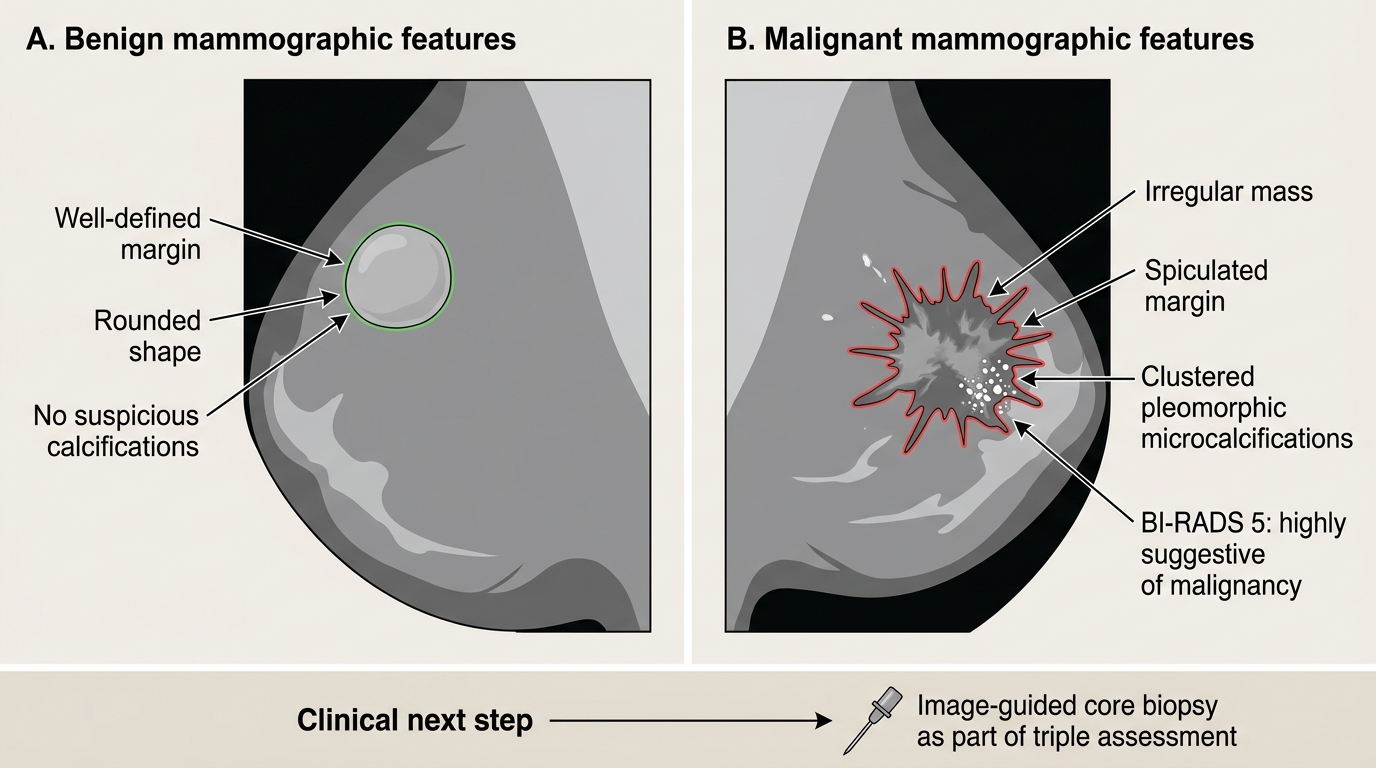
Mammographic features:
- Suspicious (malignant) features: an irregular or spiculated mass (radiating margins), architectural distortion, and clustered pleomorphic (varying shape/size) microcalcifications — fine, branching or granular calcifications in a segmental or linear distribution are particularly worrying for ductal carcinoma.
- Benign features: a well-defined, rounded or oval mass with smooth margins; coarse 'popcorn' calcification (a fibroadenoma); large rim or 'eggshell' calcification.
Ultrasound features:
- Suspicious: an irregular hypoechoic mass, taller-than-wide shape, angular or spiculated margins, and posterior acoustic shadowing.
- Benign: a smoothly marginated, wider-than-tall lesion; an anechoic cyst with posterior acoustic enhancement (a simple cyst).
The BI-RADS categories (Breast Imaging Reporting and Data System) standardise the report and its management implication:
- 0 — Incomplete: needs additional imaging or comparison.
- 1 — Negative: normal.
- 2 — Benign: definitely benign finding.
- 3 — Probably benign: very low malignancy risk; short-interval follow-up.
- 4 — Suspicious: biopsy should be considered.
- 5 — Highly suggestive of malignancy: biopsy and appropriate action.
- 6 — Known biopsy-proven malignancy: used while planning treatment.
The power of BI-RADS is that it converts a descriptive impression into a defined action, making communication between radiologist, surgeon and oncologist unambiguous.
Benign versus Malignant Mammographic Features
SELF-CHECK
A screening mammogram in a 55-year-old woman is reported as showing an irregular spiculated mass with associated clustered pleomorphic microcalcifications, assessed as BI-RADS 5. What does this mean and what is the appropriate next step?
A. BI-RADS 5 means a benign finding; routine recall in 3 years is sufficient
B. BI-RADS 5 means highly suggestive of malignancy; tissue diagnosis by image-guided core biopsy (as part of triple assessment) is the next step
C. BI-RADS 5 means the study is incomplete; only additional imaging views are needed
D. BI-RADS 5 means probably benign; short-interval follow-up imaging in 6 months is appropriate
Reveal Answer
Answer: B. BI-RADS 5 means highly suggestive of malignancy; tissue diagnosis by image-guided core biopsy (as part of triple assessment) is the next step
BI-RADS 5 means 'highly suggestive of malignancy'. The mammographic features described (irregular spiculated mass with clustered pleomorphic microcalcifications) are classic malignant features. The next step is a tissue diagnosis — image-guided core biopsy — as the pathology limb of the triple assessment, followed by staging and multidisciplinary treatment planning. BI-RADS 0 = incomplete; BI-RADS 2 = benign; BI-RADS 3 = probably benign (short-interval follow-up). Mistranslating the category would dangerously delay diagnosis.