Page 1 of 17
RD7.1 | Imaging in PCOD — SDL Guide
Learning Objectives
- State the clinical indications for pelvic imaging in a young woman with suspected polycystic ovary disease (PCOD/PCOS).
- Justify transvaginal ultrasound as the first-line imaging modality and explain when transabdominal ultrasound or MRI is preferred.
- Describe the expected ultrasound appearance of a polycystic ovary, including the current follicle-number and ovarian-volume thresholds for polycystic ovarian morphology.
- Explain that the ultrasound finding is only one of the three Rotterdam criteria and integrate it correctly into the diagnosis.
- Integrate the provided imaging findings into the diagnosis and management plan, including exclusion of mimics and the role of imaging in follow-up.
INSTRUCTIONS
Polycystic ovary disease is one of the commonest endocrine disorders of reproductive-age women and a frequent reason for referral with menstrual irregularity, hirsutism, acne or subfertility. As a final-year student you will repeatedly encounter the question 'does this woman have PCOD, and does the scan confirm it?' This module teaches you to choose the right imaging test, to read the ultrasound report intelligently, and — most importantly — to understand that the scan is supportive evidence within a clinical-biochemical framework, not a stand-alone diagnosis. Getting this right prevents both over-diagnosis (labelling a normal multifollicular ovary as PCOD) and under-recognition of a treatable metabolic and reproductive condition.
References
- Sutton's Textbook of Radiology and Imaging, 7th edition, Chapter on Gynaecological Imaging (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter on the Female Pelvis (textbook)
- International Evidence-Based Guideline for the Assessment and Management of Polycystic Ovary Syndrome, 2018 (Monash/ESHRE/ASRM) (guideline)
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group, 2003 criteria (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old college student is brought to the gynaecology outpatient clinic by her mother. Her periods, regular until two years ago, now come only once every two to three months; she has troublesome acne along her jawline and increasing facial hair that she shaves twice a week. The clinician suspects polycystic ovary disease and writes 'USG pelvis — ?PCOD' on the request form. But which ultrasound — transabdominal or transvaginal? Will a scan alone confirm the diagnosis? And if the report comes back saying 'both ovaries show multiple peripheral follicles', does that settle the matter? The answers to these questions decide whether this young woman is correctly diagnosed and counselled about a lifelong metabolic-reproductive condition, or wrongly labelled on the basis of an ovarian appearance that can be entirely normal in someone her age.
WHY THIS MATTERS
Polycystic ovary disease (PCOD), more precisely termed polycystic ovary syndrome (PCOS), affects an estimated 8-13% of reproductive-age women and is a leading cause of anovulatory subfertility, menstrual disturbance and hyperandrogenism. It also carries long-term risks of insulin resistance, type 2 diabetes, dyslipidaemia and endometrial hyperplasia. The NMC competency RD7.1 requires you to integrate provided imaging findings into the management of gynaecological conditions including PCOD — and PCOD is the condition where imaging is most often misused. Understanding exactly what the ultrasound can and cannot tell you, and where it sits within the diagnostic criteria, is a practical skill you will use in every gynaecology and family-medicine posting. The cost of getting it wrong is real: an over-called scan leads to an incorrect lifelong label, while ignoring the metabolic dimension misses preventable disease.
RECALL
Before reading further, recall:
- Ovarian follicular physiology (from PY/OG): each menstrual cycle a cohort of antral follicles is recruited; one becomes dominant and ovulates while the rest undergo atresia. A small number of 2-9 mm antral follicles is therefore NORMAL on any ovary, and a young woman early in her cycle can show many — this is the 'multifollicular' (not polycystic) ovary.
- The hypothalamic-pituitary-ovarian (HPO) axis: GnRH drives pituitary LH and FSH; in PCOS, an elevated LH:FSH ratio and increased ovarian androgen production disrupt orderly follicle selection, so follicles arrest at the small antral stage and accumulate.
- Hyperandrogenism: excess androgens (raised free testosterone, raised LH-driven theca-cell androgen output) produce hirsutism, acne and oligo/anovulation — the clinical and biochemical limbs of the diagnosis.
- Ultrasound basics: ultrasound uses no ionising radiation, so it is the imaging workhorse of gynaecology, especially in young women and pregnancy. A transvaginal probe sits close to the ovaries and uses a high frequency, giving far better spatial resolution than a transabdominal probe imaging through the abdominal wall and a full bladder.
Clinical Scenario — The Young Woman with Oligomenorrhoea and Hyperandrogenism
The clinical scenario that brings imaging into play in PCOD is consistent and recognisable: a reproductive-age woman presents with some combination of irregular or infrequent periods (oligomenorrhoea or amenorrhoea), features of androgen excess (hirsutism, acne, male-pattern hair thinning), and often difficulty conceiving or unexplained weight gain. The clinician's task is not simply to confirm a suspicion but to work through a structured diagnostic framework, because several of these features are non-specific and overlap with other conditions. Imaging enters this pathway to answer one focused question: does the ovary show the polycystic morphology that, alongside the clinical and biochemical features, supports a diagnosis of PCOS? It is essential to understand from the outset that the scan is requested to provide one piece of evidence, not to make the diagnosis on its own — a point that governs how the request is framed and how the report is interpreted.
The Rotterdam criteria (2003 ESHRE/ASRM consensus) are the framework into which the imaging fits. PCOS is diagnosed when ANY TWO of the following three features are present, after exclusion of other causes:
- Oligo-ovulation or anovulation (clinically, oligomenorrhoea or amenorrhoea).
- Clinical and/or biochemical hyperandrogenism (hirsutism, acne; or raised free testosterone / free androgen index).
- Polycystic ovarian morphology (PCOM) on ultrasound.
Because only two of the three are required, a woman who has both oligomenorrhoea and biochemical hyperandrogenism already meets the criteria — the ultrasound is then confirmatory rather than decisive. Conversely, ultrasound morphology alone, without clinical or biochemical features, does NOT diagnose PCOS. Before labelling any patient, the clinician must also exclude conditions that mimic PCOS, such as thyroid dysfunction, hyperprolactinaemia, non-classical congenital adrenal hyperplasia, and androgen-secreting tumours — a workup that combines history, examination, biochemistry and, when indicated, imaging.
Imaging Strategy — Why Transvaginal Ultrasound First, and Where It Fits in Rotterdam
The imaging strategy for suspected PCOD is governed by two principles that run through all of obstetric and gynaecological radiology: prefer ultrasound because it uses no ionising radiation and is safe in young women of childbearing potential, and choose the approach (transvaginal versus transabdominal) that gives the resolution the clinical question demands. Counting small antral follicles and measuring ovarian volume require fine spatial resolution, so the modality decision is not arbitrary — it directly determines whether the scan can reliably apply the diagnostic thresholds. A scan performed with the wrong technique can either miss true polycystic morphology or falsely suggest it, which is why understanding the strategy matters as much as understanding the findings.
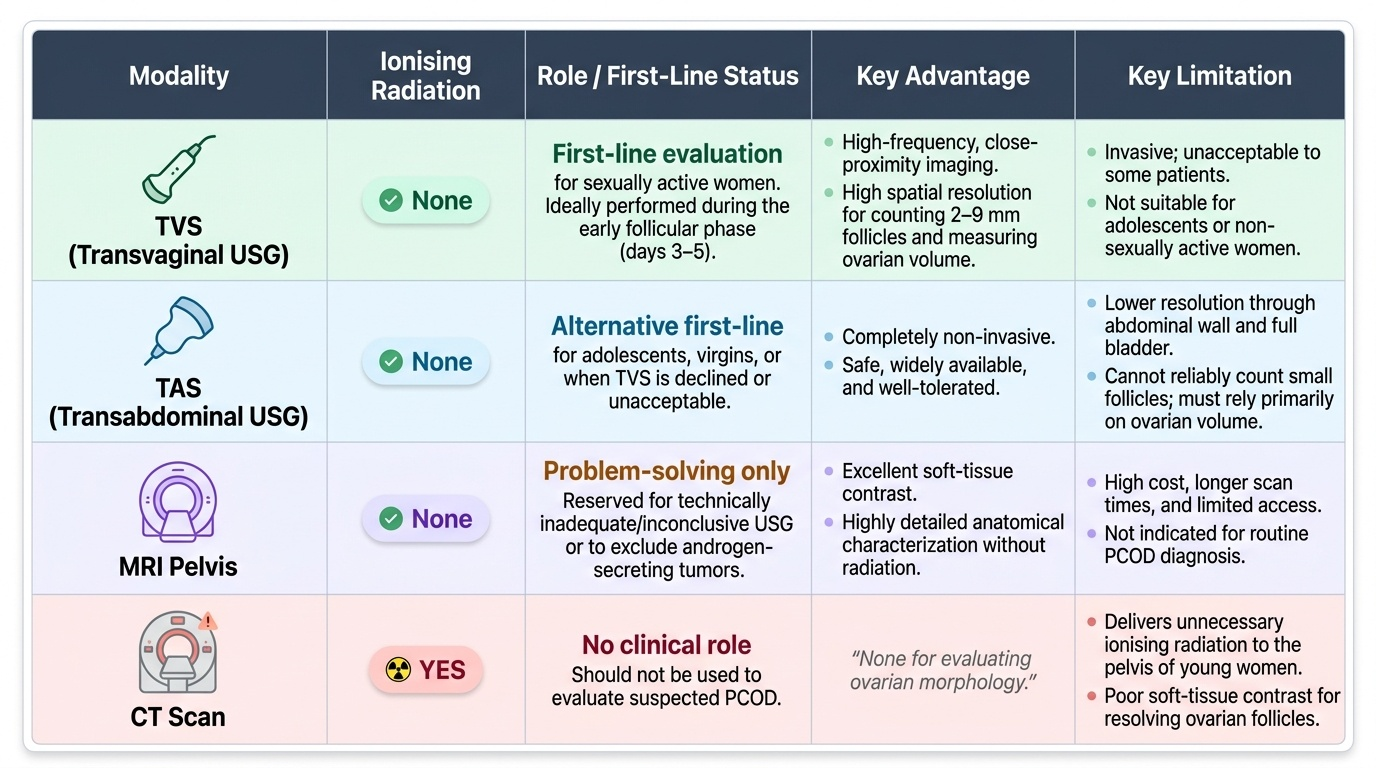
Transvaginal ultrasound (TVS) — first-line in sexually active women:
The high-frequency endovaginal probe lies close to the ovaries, giving the resolution needed to count 2-9 mm follicles accurately and to measure ovarian volume reliably. It is the preferred modality whenever it is acceptable to the patient and she is sexually active. It is ideally performed in the early follicular phase (days 3-5) when a dominant follicle or corpus luteum is least likely to confound the count and volume.
Transabdominal ultrasound (TAS) — for adolescents, virgins, or when TVS is declined:
TAS images the pelvis through the abdominal wall and a full bladder. Its resolution is lower, so small follicles may not be counted reliably; in this situation ovarian volume, not follicle number, is the usable criterion. TAS is the appropriate choice in adolescents, in women who are not sexually active, and whenever TVS is unacceptable.
MRI pelvis — problem-solving only:
MRI is reserved for cases where ultrasound is technically inadequate or inconclusive, or where an androgen-secreting ovarian or adrenal tumour must be excluded in a woman with marked or rapidly progressive virilisation. It uses no ionising radiation and gives excellent soft-tissue contrast, but it is not a routine PCOD test.
CT — essentially no role: CT delivers ionising radiation to the pelvis and ovaries of a young woman and offers no advantage for assessing ovarian morphology; it should not be used to evaluate suspected PCOD.
Crucially, the imaging finding is only ONE of the three Rotterdam criteria. The 2018 International Guideline went further and advised that ultrasound morphology should NOT be used to diagnose PCOS within 8 years of menarche, because multifollicular ovaries are physiologically common in adolescence — in that group the diagnosis rests on the clinical and biochemical criteria.
Provided image
SELF-CHECK
A 19-year-old woman who is not sexually active is referred with oligomenorrhoea and hirsutism. The clinician wants pelvic imaging to assess for polycystic ovarian morphology. What is the most appropriate first imaging approach, and what is the main caveat?
A. Transvaginal ultrasound, because it is always the most accurate test regardless of age or sexual activity
B. Transabdominal ultrasound, accepting that its lower resolution means ovarian volume rather than follicle count is the reliable criterion
C. CT pelvis, to get the highest-resolution cross-sectional images of the ovaries
D. MRI pelvis as the routine first-line test for all adolescents with suspected PCOD
Reveal Answer
Answer: B. Transabdominal ultrasound, accepting that its lower resolution means ovarian volume rather than follicle count is the reliable criterion
In a young woman who is not sexually active, transabdominal ultrasound is the appropriate approach because transvaginal scanning is not suitable. Its lower spatial resolution means small follicles cannot be counted reliably, so ovarian volume (>10 mL) becomes the usable morphological criterion. CT delivers unnecessary ionising radiation and gives no advantage; MRI is a problem-solving tool, not routine first-line. Note also that ultrasound morphology should not be used to diagnose PCOS within 8 years of menarche, so the clinical and biochemical features carry the diagnosis in adolescents.
Expected Imaging Findings — Polycystic Ovarian Morphology and What to Measure
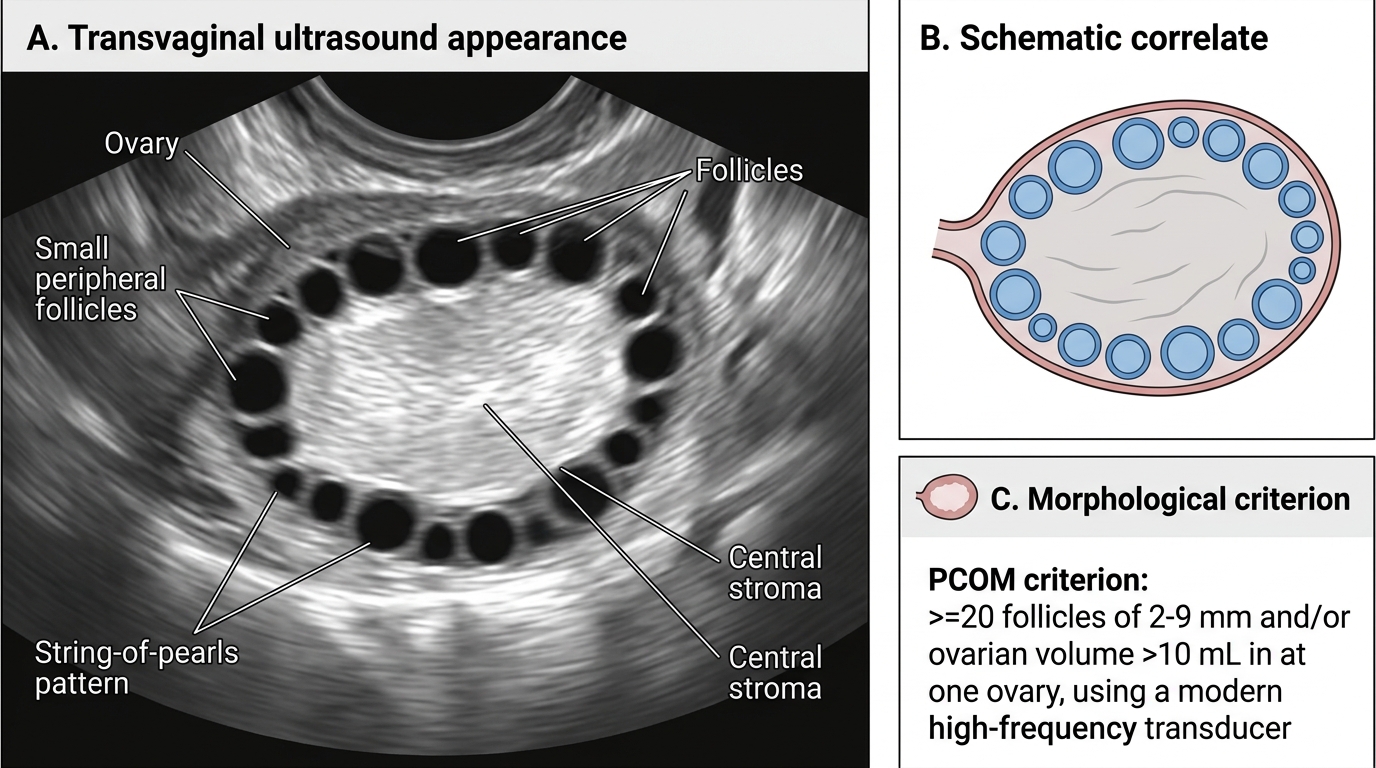
When you read or are handed an ultrasound report in suspected PCOD, you must know precisely what constitutes polycystic ovarian morphology, because the thresholds are specific and have been revised as transducer technology has improved. The classic description is of an ovary containing numerous small follicles of uniform size arranged around the periphery, giving a 'string of pearls' appearance, with an enlarged ovary and increased echogenic central stroma. However, this qualitative picture must be backed by the correct quantitative criteria, and applying an outdated or wrong threshold is one of the commonest causes of over-diagnosis. The morphological criteria are assessed on a single ovary — if EITHER ovary meets the threshold, the morphological criterion is satisfied — and ideally on a scan free of a dominant follicle, corpus luteum or cyst, which would distort the volume measurement.
The defining features of polycystic ovarian morphology (PCOM) are:
- Follicle number per ovary (FNPO): using modern high-frequency transducers (≥8 MHz, as in current transvaginal probes), the threshold is ≥20 follicles measuring 2-9 mm in at least one ovary (2018 International Guideline). With older or lower-frequency equipment the original 2003 Rotterdam threshold of ≥12 follicles of 2-9 mm per ovary is used. Always interpret the count against the equipment used.
- Ovarian volume: an ovarian volume >10 mL in either ovary (calculated as 0.523 × length × width × height) satisfies the morphological criterion. This is the criterion of choice when follicles cannot be counted reliably, as on transabdominal scanning.
- 'String of pearls' distribution: peripheral arrangement of small uniform follicles around increased central stroma — a descriptive, supportive feature rather than a measured threshold.
Key pitfalls in interpretation:
- A multifollicular ovary (normal in adolescents and early-follicular-phase scans) has fewer, more variably sized follicles distributed throughout the ovary, with normal volume — it is NOT PCOM.
- The presence of a dominant follicle, corpus luteum or cyst means the volume measurement is unreliable; the scan should be repeated in the early follicular phase if morphology is the deciding factor.
- Increased stromal echogenicity is subjective and is no longer used as a stand-alone quantitative criterion.
Polycystic Ovary on Transvaginal Ultrasound
SELF-CHECK
A transvaginal ultrasound performed with a modern high-frequency probe in the early follicular phase reports the right ovary containing 24 follicles of 2-9 mm and an ovarian volume of 12 mL, with a peripheral 'string of pearls' distribution. The left ovary is normal. Does this satisfy the morphological criterion for polycystic ovarian morphology?
A. No — both ovaries must meet the threshold for the morphological criterion to be satisfied
B. Yes — with a high-frequency transducer, ≥20 follicles of 2-9 mm and/or ovarian volume >10 mL in at least one ovary satisfies the criterion
C. No — the threshold for follicle number is ≥40 on a modern probe
D. Yes, but only because the stroma is described as echogenic; follicle number is not a criterion
Reveal Answer
Answer: B. Yes — with a high-frequency transducer, ≥20 follicles of 2-9 mm and/or ovarian volume >10 mL in at least one ovary satisfies the criterion
Using a modern high-frequency transducer, polycystic ovarian morphology is satisfied by ≥20 follicles of 2-9 mm AND/OR an ovarian volume >10 mL in at least ONE ovary (2018 International Guideline). Only one ovary needs to meet the threshold. Here the right ovary has 24 follicles and a volume of 12 mL, so the morphological criterion is met. The threshold is ≥20 (not 40) with high-frequency equipment; the older Rotterdam threshold of ≥12 applies only with lower-frequency probes. Stromal echogenicity is supportive, not a stand-alone quantitative criterion.