Page 7 of 14
RD7.5 | Imaging in Pediatric Urinary Tract Infection — SDL Guide
Learning Objectives
- Identify which children with a urinary tract infection require imaging and why, applying age- and risk-based protocols (NICE/ISPN).
- Justify the three-tool imaging strategy — ultrasound first-line, MCUG for vesicoureteric reflux, DMSA for cortical scarring — on the basis of what each answers and ALARA.
- Interpret the key findings: hydronephrosis and structural anomaly on ultrasound, the grades I–V of vesicoureteric reflux on MCUG, and photopenic cortical defects of pyelonephritis and scarring on DMSA.
- Integrate imaging findings into the management of a child with UTI, including decisions on antibiotic prophylaxis, surgical referral, and renal follow-up.
- Apply ALARA by leading with non-ionising ultrasound and reserving the ionising studies (MCUG, DMSA) for defined indications in a radiosensitive child.
INSTRUCTIONS
A urinary tract infection in a young child is never only an infection — it is a clue. In the vulnerable kidney of an infant, repeated or untreated infection can leave permanent scars, and behind a febrile UTI may lie a structural anomaly or vesicoureteric reflux that will keep the infections coming. Imaging in paediatric UTI exists to answer three separate questions — is the anatomy normal? is there reflux? has the cortex been damaged? — each with its own ideal tool. This module teaches you to select imaging by the child's age and risk, to interpret hydronephrosis, reflux grades and cortical scars, and to translate those findings into prophylaxis, referral and follow-up — all while protecting a radiosensitive child from unnecessary ionising studies.
References
- Sutton's Textbook of Radiology and Imaging, Chapter on Paediatric Uroradiology (textbook)
- Grainger & Allison's Diagnostic Radiology, Chapter on Imaging of the Paediatric Urinary Tract (textbook)
- NICE guideline on urinary tract infection in under 16s and ISPN/IAP paediatric UTI imaging protocols (guideline)
- AERB safety guidance and the Image Gently / ALARA principle for paediatric radiology (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 6-month-old girl is admitted with high fever and irritability, and a urine culture confirms a urinary tract infection. The fever settles on antibiotics within two days and the parents are keen to take her home. Is that the end of it? In a small infant, a febrile UTI is a warning light on the dashboard, not just a treated illness. Behind it may sit a kidney that is refluxing urine back up from the bladder, or a structural blockage, or a cortex already taking damage — and each repeat infection in such a kidney can carve a permanent scar that, decades later, contributes to hypertension or chronic kidney disease. The job of imaging here is to look beyond the cured fever and ask three questions: is the plumbing normal, does urine flow backwards, and has the kidney been hurt? Choosing the right test for each question — and sparing this radiosensitive child the tests she does not need — is the skill this module builds.
WHY THIS MATTERS
Urinary tract infection is one of the commonest serious bacterial infections of early childhood, and it is the gateway to detecting the conditions that threaten the developing kidney — vesicoureteric reflux (VUR), obstructive uropathy, and reflux nephropathy (renal scarring). The stakes are long-term: scarred kidneys contribute to childhood hypertension and chronic kidney disease in later life, so the imaging done after a UTI is genuinely preventive medicine. The NMC competency RD7.5 asks you to integrate imaging findings into the management of paediatric UTI — to know which child to image, which of three very different tools answers which question, and how a reflux grade or a cortical scar changes prophylaxis, referral and follow-up. Get the imaging strategy right and you protect the kidney; over-image and you expose a radiosensitive child to needless radiation and invasive tests; under-image and you miss a treatable cause of recurrent damage.
RECALL
Before reading further, recall the foundations this module builds on:
- Vesicoureteric reflux (from pathology): normally a valve-like ureterovesical junction prevents urine flowing back from the bladder to the ureters. When this mechanism is incompetent, urine refluxes upwards (VUR), carrying infection toward the kidney and predisposing to pyelonephritis and scarring.
- Ascending infection and pyelonephritis: most childhood UTIs are ascending; when infection reaches the renal parenchyma it causes acute pyelonephritis, and repeated episodes (especially with reflux) can leave permanent cortical scars — reflux nephropathy.
- Hydronephrosis: dilatation of the renal pelvis and calyces, seen on ultrasound; it may reflect obstruction, high-grade reflux, or a congenital anomaly.
- Paediatric radiation sensitivity (from RD-foundation): children are more radiosensitive with a longer latency for harm, so the ALARA / 'Image Gently' principle favours non-ionising ultrasound first and limits the ionising studies (MCUG with fluoroscopy, DMSA scintigraphy) to defined indications.
Clinical Scenario — The Infant with Fever and a Urinary Tract Infection
The clinical scenario that triggers uroradiology is the child — most importantly the infant or young child — with a confirmed urinary tract infection, and the first decision is not which scan to order but whether and why to image at all. Not every child with a UTI needs imaging, and the modern approach (NICE and ISPN/IAP protocols) is explicitly risk-stratified: imaging is targeted at the children most likely to harbour an underlying anomaly or to suffer renal damage, rather than applied reflexively to every positive culture. The factors that push a child toward imaging are younger age, a febrile (upper-tract) infection, an infection that behaves atypically, and recurrent infection — because these are the situations in which a structural cause or reflux is more likely and in which the immature kidney is most vulnerable to scarring. This stratification is itself an application of ALARA: it spares the low-risk older child with a simple lower-tract UTI from unnecessary, sometimes invasive, imaging.
The features that raise the priority for imaging include:
- Young age — infants and very young children with a febrile UTI are imaged more readily, because anomalies and reflux are commoner and the kidney is more vulnerable.
- Atypical UTI — seriously ill child, poor urine flow, an abdominal or bladder mass, raised creatinine, septicaemia, failure to respond to appropriate antibiotics within 48 hours, or infection with a non-E. coli organism.
- Recurrent UTI — repeated febrile or lower-tract infections, suggesting an underlying predisposing cause.
- Antenatally detected renal anomaly or a family history of reflux/renal disease.
For a single, typical, lower-tract UTI in an older child who responds promptly, extensive imaging is often not required. The clinician's task is therefore to place the child on this risk spectrum first, and only then to choose the appropriate combination of tools — leading, in almost every case, with ultrasound.
Imaging Strategy — Ultrasound First, MCUG for Reflux, DMSA for Scarring
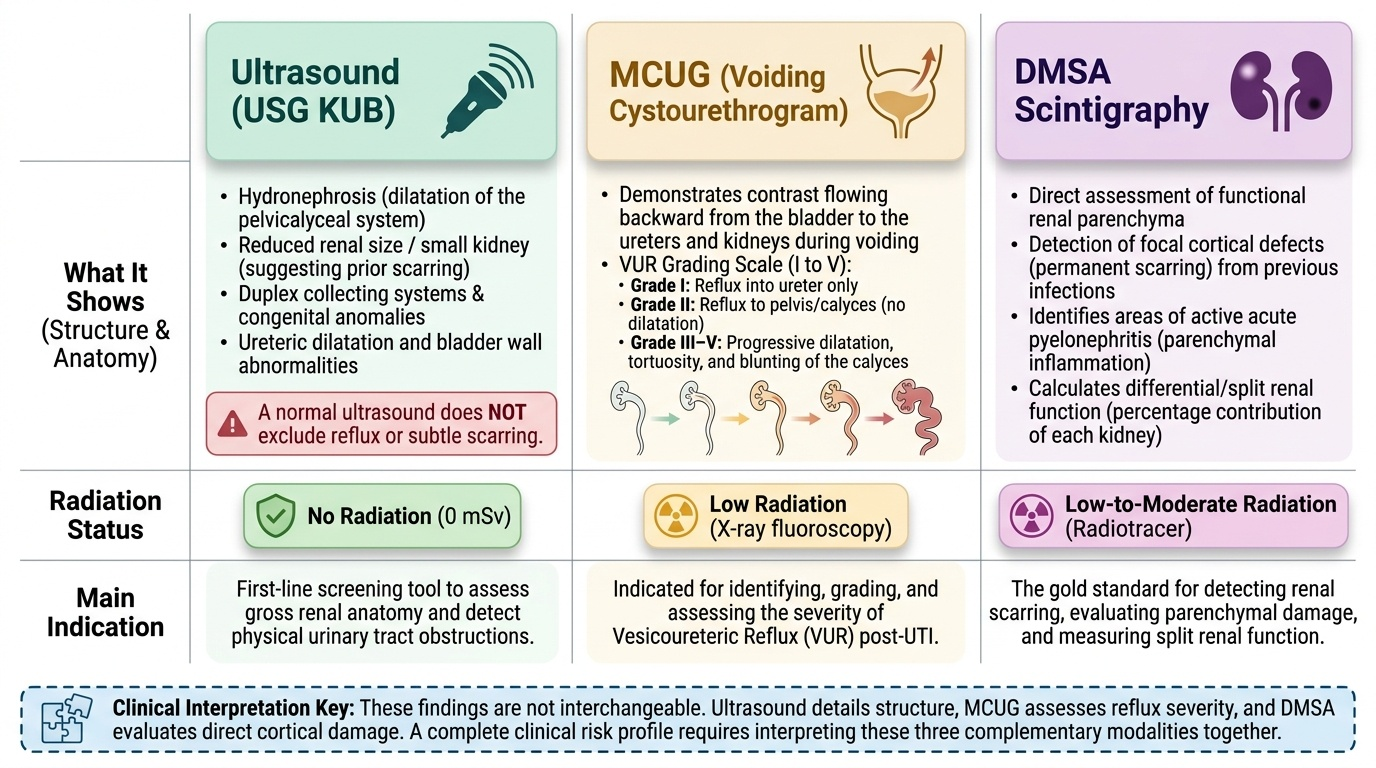
The paediatric UTI imaging strategy is best understood as three complementary tools, each answering a different question, deployed in an order that respects ALARA by leading with the non-ionising test. The art is to match the tool to the clinical question — anatomy, reflux, or cortical damage — rather than to order all three by default. Because two of the three involve ionising radiation (and one of those also requires bladder catheterisation), the strategy deliberately starts with ultrasound and reserves the others for defined indications, sparing the radiosensitive child unnecessary exposure and invasive procedures. Holding the 'one tool, one question' framework in mind is what makes the strategy logical rather than a checklist.
Ultrasound of the kidneys and bladder (USG KUB) — first-line, the anatomy tool. Ultrasound is non-ionising, widely available, needs no contrast or catheter, and is the first-line investigation in paediatric UTI. It assesses renal size and position, detects hydronephrosis, obstruction, duplex systems and other structural anomalies, shows the bladder, and can suggest scarring. It is the natural starting point and, for many children, the only imaging needed.
Micturating (voiding) cystourethrogram (MCUG/VCUG) — the reflux tool. MCUG fills the bladder with contrast through a catheter and images during voiding using fluoroscopy; it is the test that diagnoses and grades vesicoureteric reflux (VUR) and demonstrates the urethra (important for posterior urethral valves in boys). It involves both ionising radiation and catheterisation, so it is reserved for children with indications such as an abnormal ultrasound, atypical or recurrent UTI, or a high pre-test likelihood of reflux, typically in the younger age groups.
DMSA scintigraphy — the cortex tool. DMSA (dimercaptosuccinic acid) is a nuclear-medicine scan in which a radiotracer is taken up by functioning proximal-tubule cells, so areas of damaged cortex appear as photopenic (cold) defects. An early scan detects acute pyelonephritis, and a delayed scan (some months later) detects permanent cortical scarring. It uses ionising radiation and is reserved for assessing renal involvement or established scarring in selected children.
The order of use follows the ALARA logic: lead with ultrasound; add MCUG and/or DMSA only when the child's age and risk profile indicate them. This targeted, protocol-driven approach answers the necessary questions while protecting the child from the radiation and invasiveness of tests that would not change management.
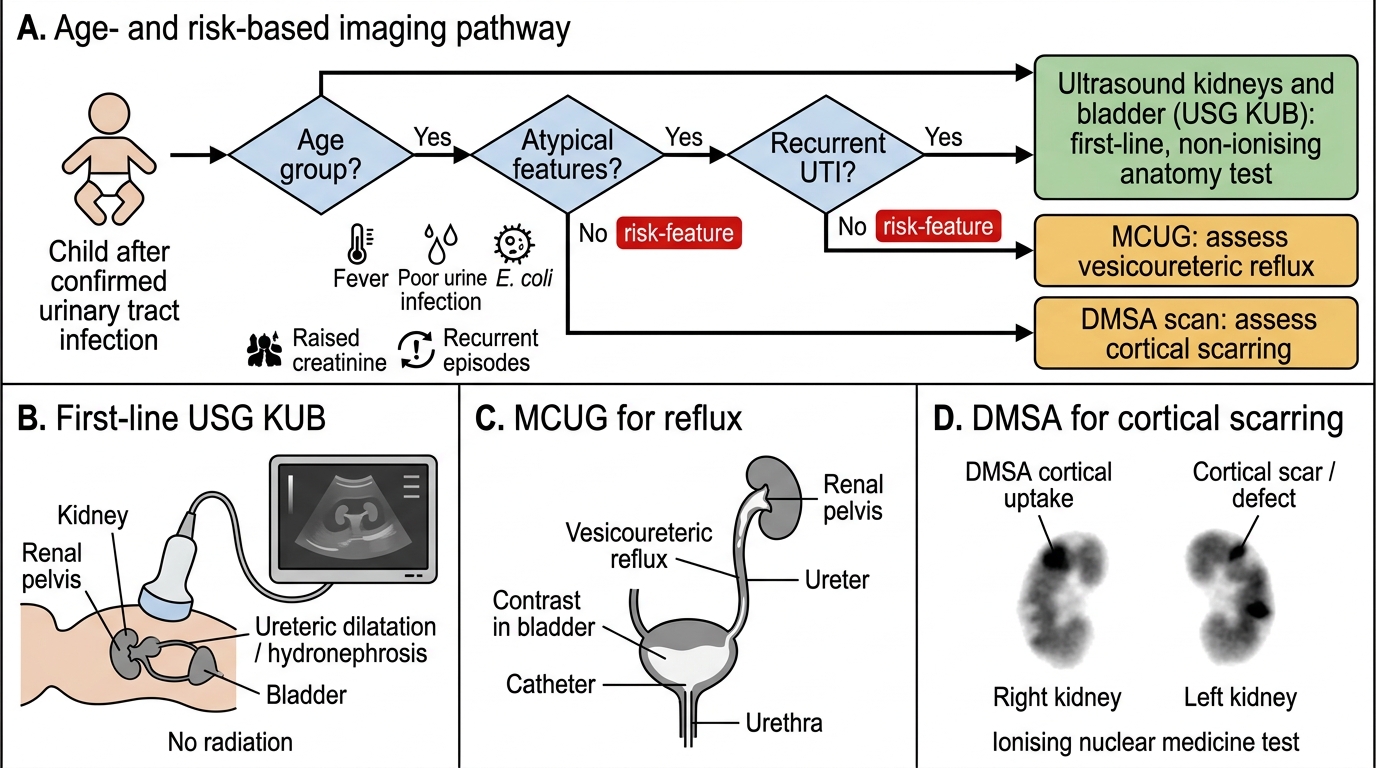
Imaging Pathway After Paediatric UTI
SELF-CHECK
A 9-month-old infant has had a first febrile urinary tract infection that responded promptly to antibiotics. Following age- and risk-based protocols, what is the most appropriate first-line imaging investigation?
A. Micturating cystourethrogram (MCUG) to grade vesicoureteric reflux immediately
B. Ultrasound of the kidneys and bladder (USG KUB), as the non-ionising first-line test to assess anatomy, hydronephrosis and structural anomaly
C. DMSA scan as the first investigation to detect any acute pyelonephritis
D. CT urogram to comprehensively assess the urinary tract in one study
Reveal Answer
Answer: B. Ultrasound of the kidneys and bladder (USG KUB), as the non-ionising first-line test to assess anatomy, hydronephrosis and structural anomaly
Ultrasound of the kidneys and bladder is the first-line investigation in paediatric UTI: it is non-ionising, needs no catheter or contrast, and assesses anatomy, hydronephrosis, obstruction and structural anomalies. MCUG (ionising + catheter, for reflux) and DMSA (ionising, for cortical involvement/scarring) are reserved for defined indications based on age and risk, not used first-line. A CT urogram is high-dose and not the appropriate first step in a child.
Imaging Findings and Their Interpretation — Hydronephrosis, Reflux Grades, Scars
Interpreting paediatric UTI imaging means reading each of the three tools for the specific question it answers and then assembling the answers into a picture of the child's risk. The findings are not interchangeable: ultrasound speaks to structure, the MCUG speaks to reflux and its severity, and DMSA speaks to whether the cortex itself has been damaged. Because management hinges on the severity of reflux and the presence of scarring, the ability to recognise and grade these findings — not merely to note that a test is 'abnormal' — is the interpretive core of this competency. Work through what each modality shows and what the finding means for the kidney.
Ultrasound (USG KUB) findings. Ultrasound demonstrates hydronephrosis (dilatation of the pelvicalyceal system), reduced renal size or a small kidney suggesting prior scarring, a duplex collecting system or other congenital anomaly, ureteric dilatation, bladder wall abnormality, and signs of obstruction. A normal ultrasound is reassuring about gross anatomy but does NOT exclude reflux or subtle scarring, which is why it is sometimes complemented by the other tools.
MCUG — grading vesicoureteric reflux (VUR). The MCUG demonstrates reflux of contrast from the bladder up the ureters and into the kidney during filling/voiding, and it is graded internationally from I to V:
- Grade I: reflux into the ureter only (no dilatation).
- Grade II: reflux up to the renal pelvis and calyces, without dilatation; calyces preserved.
- Grade III: mild–moderate dilatation of the ureter and pelvicalyceal system, with mild blunting of the calyceal fornices.
- Grade IV: moderate dilatation and tortuosity of the ureter with blunting of the calyces (loss of the sharp fornices) but preserved papillary impressions in some calyces.
- Grade V: gross dilatation and tortuosity of the ureter with severe calyceal blunting (loss of papillary impressions). Higher grades carry the greatest risk of scarring.
DMSA — cortical defects. On DMSA, damaged or non-functioning cortex fails to take up tracer and appears as a photopenic (cold) defect. An acute-phase scan shows defects of acute pyelonephritis; a delayed scan (typically several months later) distinguishes permanent cortical scarring from resolved acute change and quantifies differential renal function.
Provided image
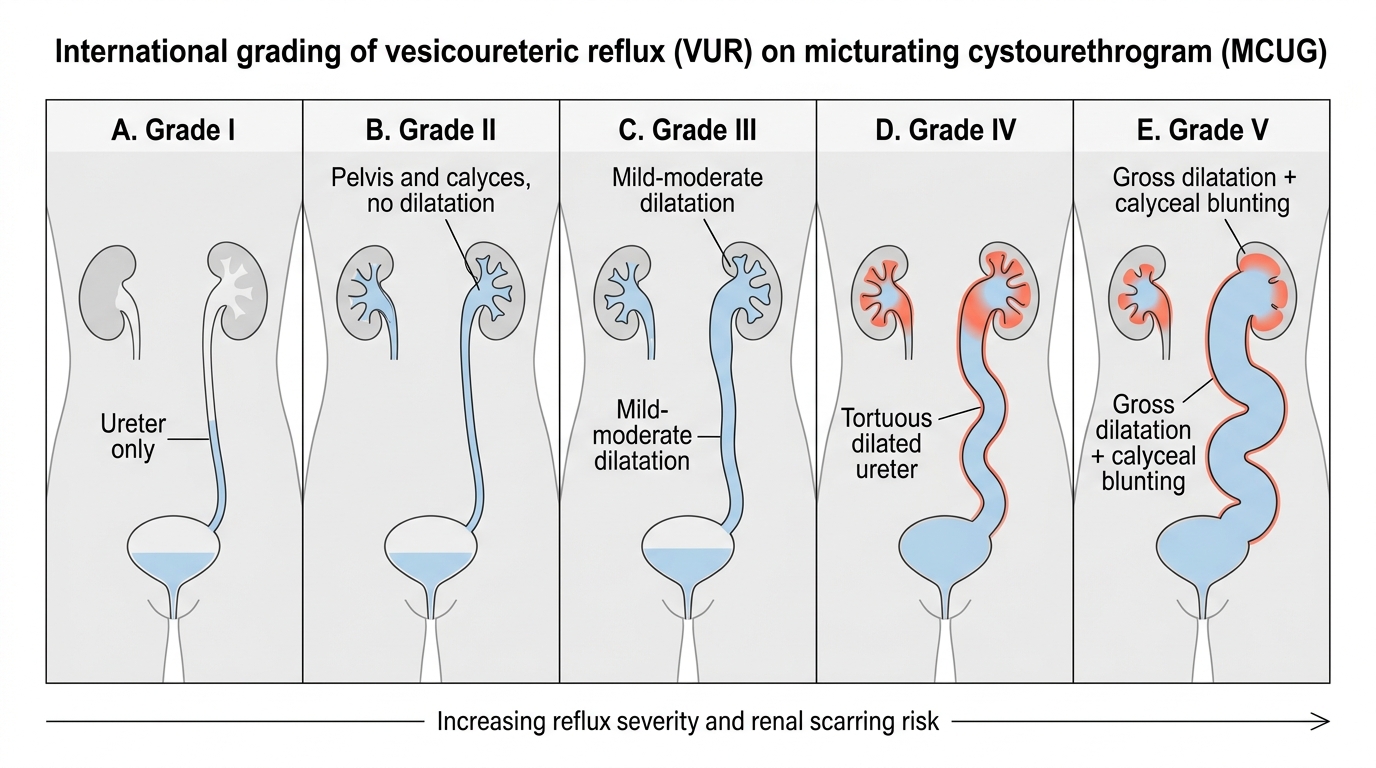
International Grading of Vesicoureteric Reflux on MCUG
SELF-CHECK
An MCUG in a child shows contrast refluxing up the ureter with gross dilatation and tortuosity of the ureter and severe blunting of the calyces with loss of the papillary impressions. How is this graded and what is its significance?
A. Grade I VUR; trivial, no clinical significance
B. Grade V VUR; the most severe grade, carrying the highest risk of renal scarring and most likely to need active management
C. Grade II VUR; reflux to the pelvis without dilatation
D. It indicates obstruction, not reflux, and should be staged separately
Reveal Answer
Answer: B. Grade V VUR; the most severe grade, carrying the highest risk of renal scarring and most likely to need active management
Gross ureteric dilatation and tortuosity with severe calyceal blunting (loss of papillary impressions) is grade V vesicoureteric reflux — the most severe grade. Grade I is reflux into the ureter only; grade II reaches the pelvis without dilatation. Higher grades (IV–V) carry the greatest risk of renal scarring and are most likely to warrant active management such as prophylaxis, close follow-up, or surgical referral. The MCUG demonstrates reflux (retrograde flow), distinct from obstruction.