Page 4 of 14
RD3.2 | ALARA Practice and AERB Regulatory Principles — SDL Guide
Learning Objectives
- State the three fundamental principles of radiation protection — justification, optimisation (ALARA) and dose limitation — and to whom each applies.
- Explain the ALARA principle and apply the three practical protection tools: time, distance and shielding.
- Use the inverse-square law to predict how distance reduces radiation dose.
- Identify the AERB as India's statutory radiation regulator under the Atomic Energy Act 1962 and describe its key functions.
- Distinguish the AERB from the advisory ICRP and from the US NRC, and state the relevant occupational and public dose limits.
INSTRUCTIONS
The previous module established that ionising radiation is hazardous and how that hazard is measured. This module is about control — how we keep that hazard as low as possible and who enforces the rules. It introduces the ALARA principle and the wider radiation-protection framework, the three everyday tools (time, distance, shielding) that put ALARA into practice, and the Atomic Energy Regulatory Board (AERB), India's statutory radiation regulator. These are the practical and regulatory skills that competency RD3.2 demands of every clinician working in or referring to a radiology service, and they are a recurring source of examination error when the Indian regulator is confused with international bodies.
References
- Sutton's Textbook of Radiology and Imaging, 7th edition, Chapter 1 (Physics and Radiation Protection) (textbook)
- Grainger & Allison's Diagnostic Radiology, 7th edition, Chapter on Radiation Protection (textbook)
- Atomic Energy Regulatory Board (AERB) Safety Code for Medical Diagnostic X-ray Equipment and Installations (AERB/RF-MED/SC-3), India (guideline)
- ICRP Publication 103 (2007 Recommendations of the International Commission on Radiological Protection) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Picture two interns observing the same fluoroscopy-guided reduction of a fractured wrist. The first stands at the patient's side throughout, leaning in for a better view, with no apron. The second puts on a lead apron and thyroid shield, takes one good look, then steps back two metres behind the operator and watches the monitor. Both see the procedure. Months later, if you compared their dosimeter records, the second intern's accumulated dose would be a tiny fraction of the first's — not by luck, but by deliberately applying three simple levers: spending less time near the beam, keeping greater distance from it, and putting shielding between body and source. This is not abstract physics; it is the everyday practice of radiation protection, and it has a name — ALARA. Behind ALARA sits a national regulator, the AERB, whose rules make these protections mandatory rather than optional. This module turns the hazard you learned about into a set of controls you can actually use.
WHY THIS MATTERS
Competency RD3.2 asks you to be knowledgeable about the best practices — time, distance and shielding — and the provisions that keep X-ray exposure As Low As Reasonably Achievable (ALARA) in clinical practice, and about the general principles to be followed under AERB regulatory guidelines. This is a practical competency with direct consequences: it protects you and your colleagues across a career of cumulative exposure, it protects your patients from unnecessary dose, and it keeps your institution on the right side of the law. Every doctor who orders an X-ray, stands in during a portable film, assists at fluoroscopy, or runs a clinic with an imaging unit is touched by these rules. Examiners reliably test two things here: the correct application of the time–distance–shielding triad (including the inverse-square law), and the identity of the Indian regulator (the AERB — not the ICRP or the US NRC). Getting both right marks you out as a clinician who treats radiation safety as a working discipline rather than a textbook curiosity.
RECALL
Before continuing, recall the foundations laid in the previous SDL and your basic physics:
- Stochastic effects have no threshold: because radiation-induced cancer is assumed to carry some risk at any dose (the linear-no-threshold model), there is no 'safe' dose to aim for — only a 'reasonably achievable minimum'. This is the scientific reason ALARA exists.
- Effective dose is measured in millisieverts (mSv): the biologically weighted dose unit against which limits are set.
- The inverse-square law: for a point source, intensity falls in proportion to the square of the distance (I ∝ 1/d²). Recall this from Year-1 physics — it is the engine behind 'distance' as a protection tool.
- Lead attenuates X-rays strongly: its high atomic number makes it an efficient absorber, which is why aprons and barriers are made of (or lined with) lead.
- Patient vs worker: a patient receives dose for their own diagnostic benefit; a worker receives dose only as an occupational by-product. This distinction matters for which protection principle applies.
A quick refresher on the inverse-square law in particular will make the 'distance' section below intuitive rather than memorised.
Orientation — From Knowing the Hazard to Controlling It
Understanding that ionising radiation carries a no-threshold stochastic risk creates an immediate practical problem: if there is no dose that is provably safe, how should a health service decide how much radiation is acceptable? The answer cannot be 'zero', because that would mean abandoning X-rays and CT altogether and losing their enormous diagnostic benefit. Nor can it be 'whatever is convenient', because that ignores the cumulative harm. Radiation protection resolves this tension with a disciplined middle path: permit radiation only where it does net good, then drive the resulting dose down to the lowest level that is reasonably achievable. This is the conceptual leap from the previous module's knowledge of the hazard to this module's control of the hazard, and it is the reasoning that every protection rule ultimately serves.
Controlling radiation operates at two complementary levels that you should keep distinct:
- A principled framework — a small set of universal principles (justification, optimisation/ALARA, dose limitation) that define what radiation protection is trying to achieve.
- Practical tools and regulation — the concrete day-to-day methods (time, distance, shielding) that put the principles into action, and a regulator (the AERB in India) that makes the whole system legally enforceable rather than merely advisory.
Keeping these two levels in mind prevents a common confusion: ALARA is a principle (a goal), whereas time, distance and shielding are the methods by which the principle is met. The rest of this module fills in both levels.
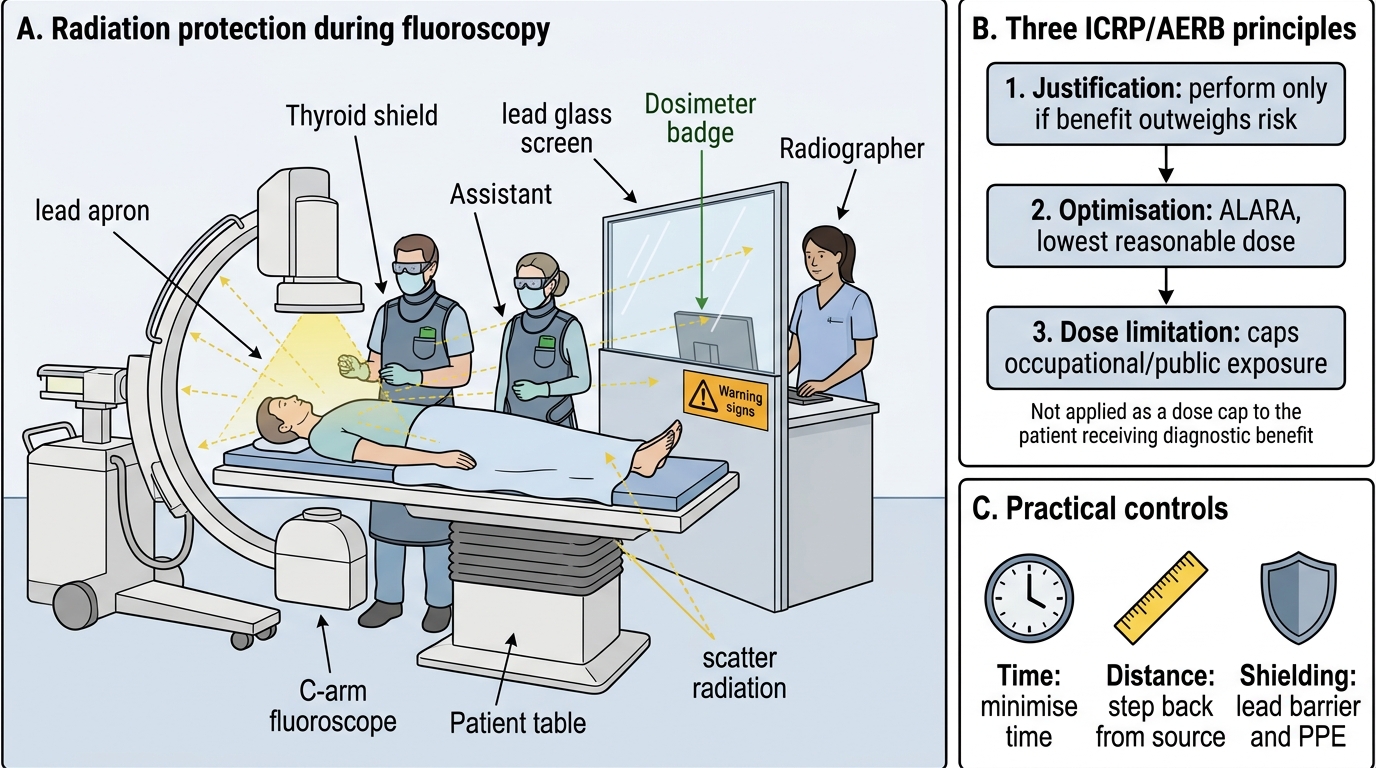
Radiation Protection in Fluoroscopy Practice
The Radiation-Protection Framework — Three Principles and the AERB
Radiation protection rests on three fundamental principles, formulated by the International Commission on Radiological Protection (ICRP) and adopted into Indian regulation by the AERB. They form a deliberate logical sequence — first decide whether to expose the person at all, then, having decided to expose, minimise the actual exposure, and finally cap the cumulative total for those who receive radiation as a by-product rather than a benefit. Holding the three principles apart, and knowing exactly to whom each one applies, is the conceptual core of this competency and a frequent point of confusion in examinations, because one of the three deliberately does NOT apply to patients receiving their own diagnostic studies. Working through them in order also mirrors the real decision path a clinician and a department follow whenever an ionising investigation is contemplated, which is why the sequence is worth committing to memory rather than the bare names alone.
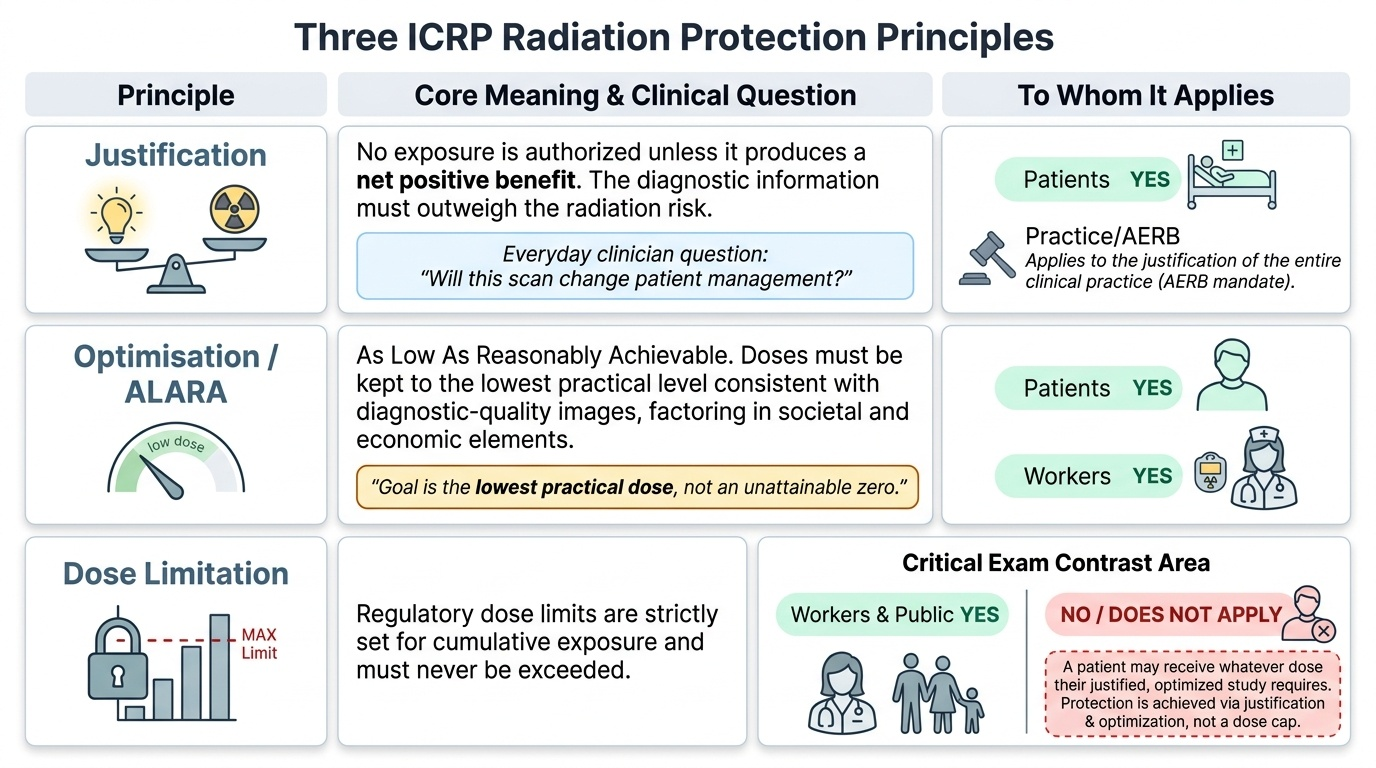
The three principles are:
- Justification: no exposure should be authorised unless it produces a net benefit — the diagnostic information must be worth more than the radiation detriment. For an ordering clinician this is the everyday question 'will this scan change management?'.
- Optimisation (the ALARA principle): once justified, the exposure must be kept As Low As Reasonably Achievable, economic and societal factors being taken into account. 'Reasonably achievable' is the key qualifier — it accepts that the goal is the lowest practical dose consistent with a diagnostic-quality image, not an unattainable zero. ALARA applies to both patients and workers.
- Dose limitation: regulatory dose limits are set for occupationally exposed workers and the public, and must not be exceeded. Critically, dose limits do NOT apply to the patient's own diagnostic exposure — a patient may receive whatever dose their justified, optimised investigation requires. Patient protection is achieved by justification and optimisation, not by a dose cap.
In India these principles are given legal force by the Atomic Energy Regulatory Board (AERB), constituted in 1983 under the Atomic Energy Act 1962. The AERB is the country's statutory radiation regulator. Its functions relevant to diagnostic imaging include:
- Licensing and registration of all X-ray and CT installations (now through the online eLORA system), so that no facility may operate an X-ray machine without registration.
- Laying down safety codes and standards for equipment, installation layout and shielding.
- Setting dose reference levels and requiring periodic quality-assurance testing by qualified medical physicists / RSOs (Radiological Safety Officers).
- Enforcement — inspection and the power to suspend non-compliant facilities.
It is essential not to confuse the AERB with two bodies often mentioned alongside it: the ICRP is an international advisory commission that recommends principles and limits but has no regulatory authority in India; the US Nuclear Regulatory Commission (NRC) is the American regulator and has no jurisdiction here. For India, the regulator is the AERB.
Provided image
SELF-CHECK
A radiology resident states that 'AERB dose limits cap how much radiation a patient may receive from a justified CT scan'. Which correction is accurate?
A. The statement is correct — patient diagnostic doses are capped by AERB dose limits
B. Dose limits apply to occupational workers and the public, NOT to a patient's own diagnostic exposure; the patient is protected by justification and optimisation (ALARA) instead
C. Dose limits apply only to patients, never to workers
D. There are no dose limits in India because the AERB only issues advisory recommendations
Reveal Answer
Answer: B. Dose limits apply to occupational workers and the public, NOT to a patient's own diagnostic exposure; the patient is protected by justification and optimisation (ALARA) instead
Regulatory dose limits apply to occupationally exposed workers and to members of the public — NOT to a patient's own diagnostic exposure. A patient may receive whatever dose their justified and optimised investigation requires; patient protection is achieved through the justification and optimisation (ALARA) principles, not a dose cap. The AERB is a statutory regulator (it issues binding rules, not merely advice — that is the ICRP's role). Limits are not patient-only; workers and the public are precisely whom they protect.
How ALARA Works in Practice — Time, Distance and Shielding
The ALARA principle would be empty without concrete methods to achieve it, and there are exactly three practical levers, traditionally taught together as the radiation-protection triad: time, distance and shielding. These three apply directly to staff protecting themselves and, in adapted forms, to protecting patients as well. Understanding the simple physics that sits behind each lever is what lets you apply them intelligently rather than ritually — particularly the inverse-square law, which makes distance by far the most powerful and the cheapest of the three controls. Mastering this triad is the practical heart of competency RD3.2 and is precisely the difference between a clinician who merely owns a lead apron and one who actually minimises the dose they and their patients receive. None of the three is optional or interchangeable: each addresses a different part of how dose accumulates, so a complete protection strategy always deploys all three together rather than relying on a single favourite measure.
The three tools are:
- Time: dose accumulates with the duration of exposure, so minimising time near the source minimises dose. In fluoroscopy this means keeping screening time short, using pulsed rather than continuous fluoroscopy, using last-image-hold, and never leaving the beam on while looking away. Fewer and shorter exposures also means avoiding unnecessary repeat films.
- Distance: this is the most effective and the cheapest lever, because radiation from a point source obeys the inverse-square law — intensity falls in proportion to the square of the distance (I ∝ 1/d²). The practical consequence is striking: doubling your distance from the source quarters your dose; tripling it cuts the dose to one-ninth. Simply stepping back a metre or two during an exposure dramatically reduces a worker's dose, which is why staff stand well back (or behind a barrier) during acquisitions.
- Shielding: placing an attenuating barrier between the body and the source. Practical shielding includes lead aprons (typically 0.25–0.5 mm lead equivalent; 0.5 mm where exposure is higher), thyroid shields, lead glasses to protect the radiosensitive lens, gonadal shields where they do not obscure the region of interest, and fixed structural barriers — lead-lined walls, lead-glass control-room windows and mobile lead screens. Shielding is essential where time and distance alone cannot bring dose low enough, such as during prolonged interventional work.
A crucial nuance for patients: the most important 'time and distance' control on the patient's dose is good technique by the operator — correct collimation (restricting the beam to the area of interest), appropriate exposure factors, and avoiding repeats — rather than the patient moving away, which is impossible during their own examination. Shielding sensitive patient organs (e.g. gonadal or, historically, abdominal shielding in pregnancy) supplements this where appropriate.
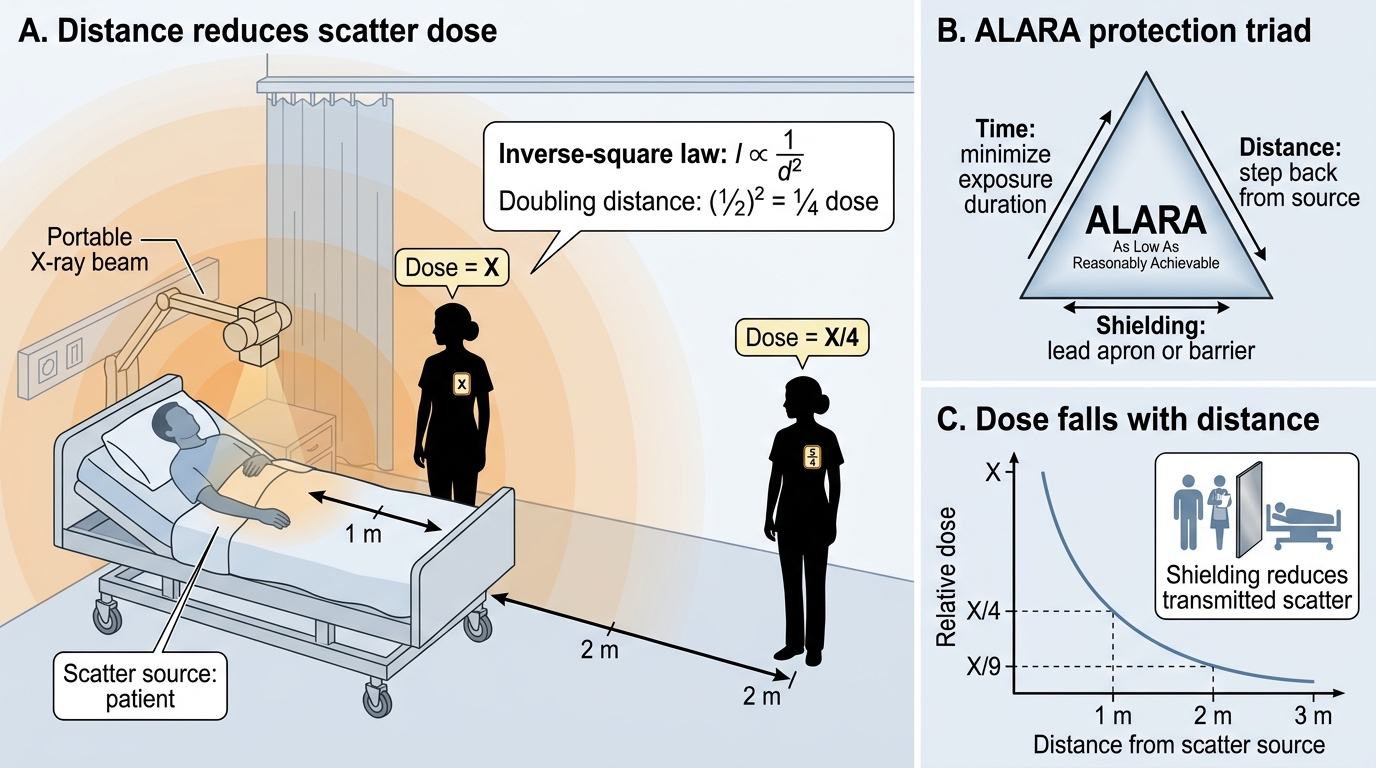
ALARA Triad and Inverse-Square Dose Reduction
SELF-CHECK
During a portable chest X-ray on the ward, a nurse needs to remain to support an unstable patient. The X-ray dose at 1 metre from the patient (the scatter source) is measured as X. If she instead stands at 2 metres, approximately what dose would she receive, by the inverse-square law?
A. Half of X (X/2)
B. One-quarter of X (X/4)
C. One-eighth of X (X/8)
D. The same as X — distance does not affect scatter dose
Reveal Answer
Answer: B. One-quarter of X (X/4)
By the inverse-square law, intensity falls in proportion to the square of the distance (I ∝ 1/d²). Doubling the distance from 1 m to 2 m reduces the dose to (1/2)² = one-quarter of X. This is why 'distance' is the most powerful and cheapest protection lever — simply stepping back dramatically lowers dose. Halving (X/2) would be a linear, not inverse-square, relationship and is wrong; X/8 would correspond to a larger distance increase; and distance certainly does affect scatter dose.