Page 10 of 17
RD7.4 | Imaging in Intestinal Obstruction — SDL Guide
Learning Objectives
- Recognise the clinical presentation of intestinal obstruction and state the role of imaging in confirming and characterising it.
- Justify the abdominal X-ray as the first investigation and contrast-enhanced CT as the modality of choice for level and cause.
- Distinguish small-bowel from large-bowel obstruction on plain film by loop position, mucosal markings and calibre.
- Identify the imaging signs of closed-loop obstruction, ischaemia and perforation.
- Integrate described imaging findings into the surgical management of intestinal obstruction.
INSTRUCTIONS
Intestinal obstruction is a common surgical emergency in which bowel contents cannot pass, and the decisions that follow — operate now, or resuscitate and observe — turn on imaging. The clinical picture raises the suspicion, the plain abdominal X-ray confirms it cheaply and fast, and CT answers the questions that determine treatment: where is the obstruction, what is causing it, and is the bowel ischaemic? This module, aligned to competency RD7.4, trains you to read the small-bowel versus large-bowel pattern, to spot the danger signs of strangulation and perforation, and to integrate those findings into a surgical plan.
References
- Sutton's Textbook of Radiology, 6th edition, Chapter on the Acute Abdomen (textbook)
- Grainger & Allison's Diagnostic Radiology, 6th edition, Chapter on Bowel Obstruction (textbook)
- Bohner H et al. and Bologna guidelines for adhesive small bowel obstruction (WSES) (guideline)
- Bailey & Love's Short Practice of Surgery, Chapter on Intestinal Obstruction (clinical correlation) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 65-year-old woman with a previous hysterectomy comes to casualty with 2 days of colicky central abdominal pain, profuse vomiting, a distended abdomen and no flatus or stool. The surgical team suspects intestinal obstruction, and the question is immediate: what is the first investigation, and will this patient need an operation tonight? An erect and supine abdominal X-ray takes minutes and confirms dilated small-bowel loops with multiple air–fluid levels — but it cannot tell the team whether the trapped bowel is alive or dying. That distinction, between a simple adhesional obstruction that may settle with a nasogastric tube and a strangulating closed-loop that needs urgent surgery, is what the CT will answer. The imaging pathway you choose — plain film first, then CT — is the spine of safe decision-making in the obstructed abdomen.
WHY THIS MATTERS
Intestinal obstruction accounts for a large share of emergency surgical admissions, and adhesions from previous surgery are its commonest small-bowel cause in adults. As a final-year student and intern, you will repeatedly assess the distended, vomiting patient and you will be asked to interpret the first abdominal film and to decide whether a CT is needed. Competency RD7.4 requires you to integrate imaging findings into the management of intestinal obstruction — to recognise small- versus large-bowel patterns, to identify the level and cause, and above all to detect the signs of strangulation and perforation that convert a 'watch and wait' patient into an emergency laparotomy. This is applied radiology where reading the film correctly directly shortens the path to life-saving surgery, or safely avoids an unnecessary one.
RECALL
Before reading further, recall:
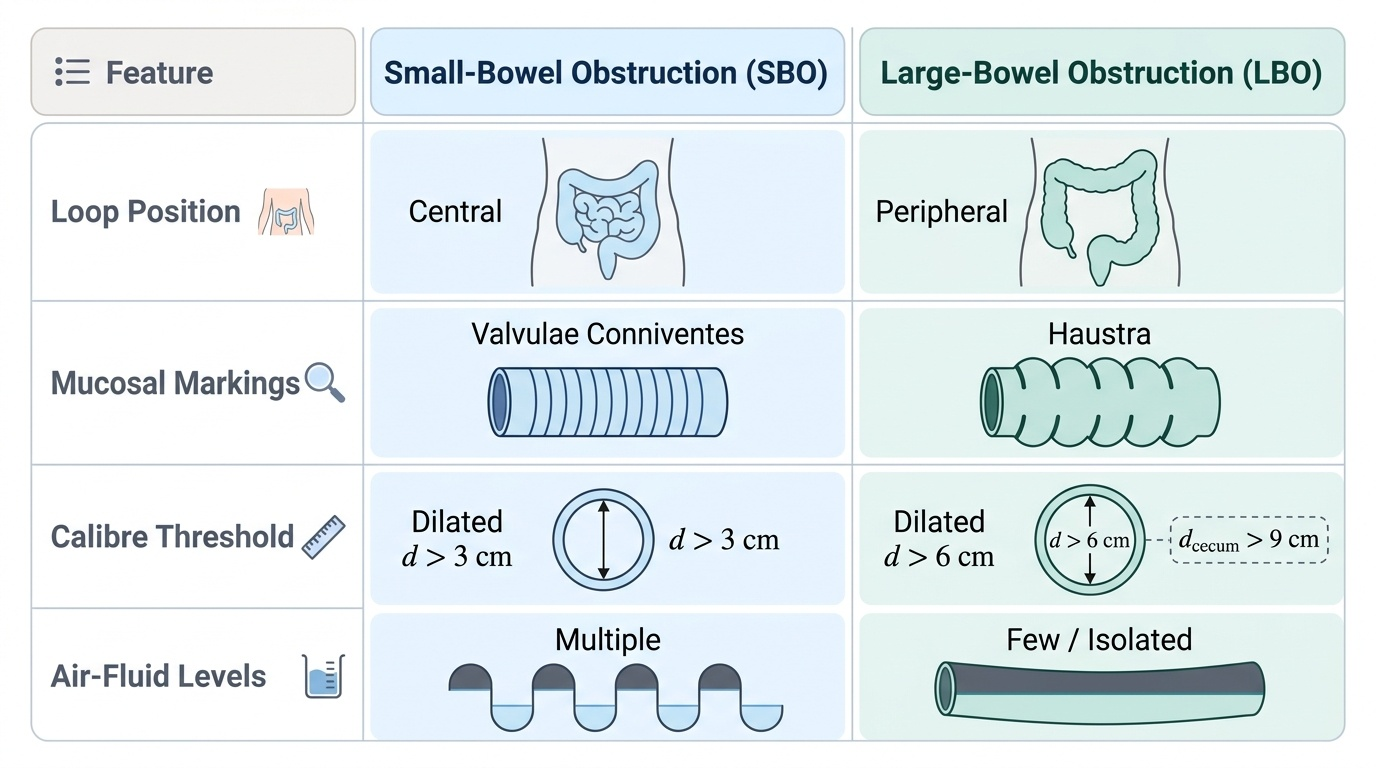
- Small- vs large-bowel mucosal anatomy (from AN): the small bowel has valvulae conniventes (plicae circulares) — folds that cross the full width of the lumen; the large bowel has haustra — sacculations whose folds (semilunar) do not cross the full lumen. This single anatomical difference is the basis of distinguishing small- from large-bowel obstruction on a plain film.
- Normal bowel calibre (from RD-foundation): the small bowel is normally up to about 3 cm in diameter, the colon up to about 6 cm, and the caecum up to about 9 cm; dilatation beyond these thresholds suggests obstruction.
- Closed-loop and strangulation (from the strangulated-hernia SDL): a segment obstructed at two points forms a closed loop that is intrinsically prone to ischaemia; ischaemic bowel does not enhance with intravenous contrast — the same principle applies wherever bowel is obstructed.
- Causes of obstruction (from Surgery): small bowel — adhesions (commonest), herniae, tumours, intussusception; large bowel — colorectal carcinoma (commonest), volvulus, diverticular stricture. Functional obstruction (paralytic ileus, pseudo-obstruction) has no mechanical block.
Clinical Scenario — The Obstructed Abdomen and the First Film
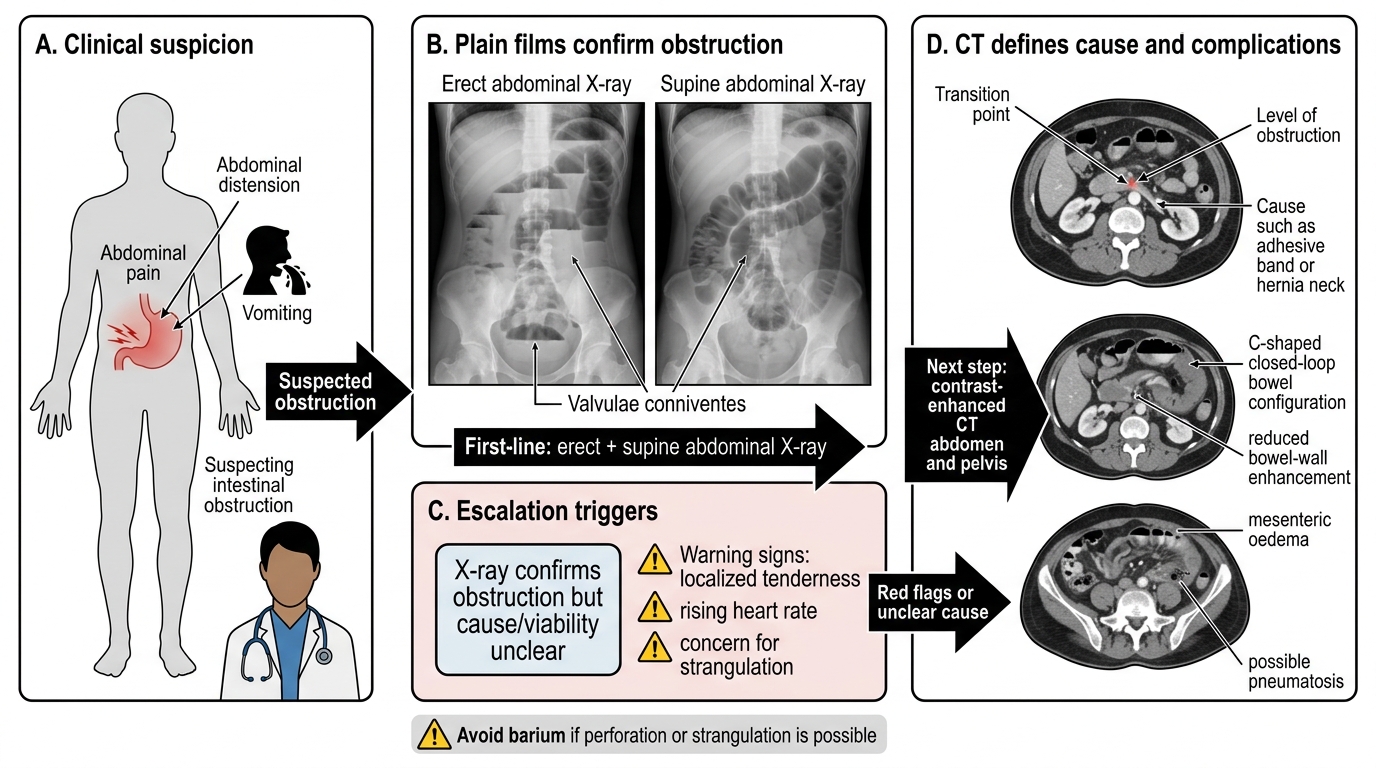
Intestinal obstruction announces itself with a recognisable clinical quartet, and the clinician's first task is to suspect it and order the right first investigation. The cardinal features are colicky abdominal pain, vomiting (early and bilious in proximal small-bowel obstruction, later and faeculent in distal or large-bowel obstruction), abdominal distension (more marked the more distal the block), and absolute constipation (no passage of flatus or stool, the hallmark of complete obstruction). The history often points to the cause — previous abdominal surgery suggests adhesions, a change in bowel habit with weight loss suggests a colorectal tumour, and a known hernia points to an obstructed hernia. On examination the abdomen is distended and tympanitic with active 'tinkling' bowel sounds early on; tenderness, guarding, fever and tachycardia raise the alarm for strangulation.
The role of imaging in this scenario is to confirm the obstruction, localise it (small versus large bowel, and the level), identify the cause, and — most importantly for management — detect complications (closed-loop, ischaemia, perforation). The first investigation is the plain abdominal X-ray, which is cheap, fast and available everywhere; it confirms the obstruction and gives the first clue to its level. It is, however, only the opening move: a plain film cannot reliably tell whether bowel is viable, and so a normal-appearing or merely 'obstructed' film does not end the assessment. The clinician must therefore read the patient and the film together:
- Features that demand urgent escalation and CT: localised tenderness, peritonism, fever, tachycardia, or a rising lactate — all suggesting strangulation or perforation.
- Features that suggest a simpler course: a soft, non-tender distended abdomen in a patient with prior surgery and a clinical picture of adhesional small-bowel obstruction, which may settle with conservative measures while being monitored.
The governing principle is that the plain film opens the assessment and the clinical picture decides its urgency, but the definitive characterisation — level, cause and viability — usually requires CT.
Imaging Strategy — Plain X-ray First, CT to Map Level and Cause
The imaging strategy in intestinal obstruction is a two-step sequence whose logic is the same speed-then-detail reasoning used throughout acute imaging: a fast, cheap film to confirm the problem, then a comprehensive study to map it. The first step answers 'is there an obstruction and roughly where?'; the second answers 'what is causing it, and is the bowel in danger?'. Understanding why each step exists prevents both the error of operating on the basis of a plain film alone and the error of delaying a CT in a patient who is showing signs of strangulation.
Erect and supine abdominal X-ray — first-line:
The traditional first investigation is the plain abdominal radiograph, classically taken supine (to show the distribution and calibre of dilated loops and the mucosal pattern) and erect (to demonstrate air–fluid levels and free subdiaphragmatic gas). It confirms obstruction, gives the first indication of small- versus large-bowel level, and can show free air indicating perforation. An erect chest X-ray is also valuable for detecting free gas under the diaphragm. Plain films are quick and universally available but are limited: they cannot reliably identify the cause or assess bowel viability, and they may be equivocal.
Contrast-enhanced CT abdomen/pelvis — modality of choice for characterisation:
CT is the modality of choice for the full characterisation of obstruction. It reliably identifies the level (the transition point between dilated proximal and collapsed distal bowel), the cause (adhesion, hernia, tumour, volvulus, intussusception), and — critically — the danger signs: a closed-loop configuration, and ischaemia shown by reduced or absent bowel-wall enhancement, wall thickening, mesenteric oedema and free fluid. Intravenous contrast is used precisely so that enhancement (and therefore viability) can be assessed. CT thus converts the plain film's 'there is an obstruction' into the actionable 'this level, this cause, and the bowel is/ is not ischaemic'.
A note on other studies: water-soluble contrast follow-through (e.g. Gastrografin) is sometimes used in adhesional small-bowel obstruction both to predict which patients will settle without surgery and for a mild therapeutic effect; ultrasound has a limited role but can show dilated, fluid-filled loops and free fluid.
Imaging Pathway for Suspected Intestinal Obstruction
SELF-CHECK
A patient with suspected intestinal obstruction has an abdominal X-ray confirming dilated small-bowel loops with air-fluid levels, but no clear cause is visible and the patient now has localised tenderness and a rising heart rate. What is the most appropriate next imaging step?
A. No further imaging; manage on the plain film findings alone
B. Contrast-enhanced CT abdomen and pelvis to identify the level and cause and to assess for closed-loop obstruction and ischaemia
C. Barium follow-through to outline the small bowel in detail
D. Repeat the plain abdominal X-ray every 6 hours until the cause appears
Reveal Answer
Answer: B. Contrast-enhanced CT abdomen and pelvis to identify the level and cause and to assess for closed-loop obstruction and ischaemia
The plain film confirms obstruction but cannot identify the cause or assess bowel viability; with localised tenderness and tachycardia raising concern for strangulation, a contrast-enhanced CT abdomen and pelvis is the modality of choice to define the level, the cause, and — using bowel-wall enhancement — whether there is a closed-loop or ischaemia. Barium is contraindicated where perforation is possible (it causes severe peritonitis), and repeating plain films delays the definitive assessment in a deteriorating patient.
Imaging Findings — Small Bowel vs Large Bowel, and Signs of Danger
Reading the obstructed abdomen begins with one decision that the plain film makes well: is this small-bowel or large-bowel obstruction? The distinction rests on three features — the position of the dilated loops, their mucosal markings, and their calibre — and it matters because the likely causes and the management differ between the two. After establishing the level, the clinician looks for the signs that indicate danger (closed-loop, strangulation, perforation), most of which are best seen on CT but some of which (free air, the coffee-bean of volvulus) are visible on plain film. This systematic reading — level first, then danger signs — is the applied core of interpreting obstruction, and it is a discipline worth practising on every film so that the pattern becomes second nature before the pressure of an acute admission.
Small-bowel obstruction (SBO) on plain film:
- Dilated loops lie centrally in the abdomen.
- The mucosal folds are valvulae conniventes, which cross the entire width of the lumen (a 'stack of coins' or 'ladder' pattern).
- Loops are dilated greater than ~3 cm.
- Multiple air–fluid levels on the erect film; little or no gas in the colon/rectum in complete obstruction.
Large-bowel obstruction (LBO) on plain film:
- Dilated loops lie peripherally (around the abdominal margin) and the colonic course (caecum, ascending, descending) may be recognisable.
- The mucosal markings are haustra, which do NOT cross the full width of the lumen.
- Calibre exceeds the normal limits — colon greater than ~6 cm, caecum greater than ~9 cm; a caecum approaching 9–12 cm is at high risk of perforation.
- A sigmoid volvulus gives a classic 'coffee-bean' or inverted-U loop arising from the pelvis.
Danger signs (mainly CT, some plain film):
- Free subdiaphragmatic gas on the erect chest/abdominal film indicates perforation.
- A closed-loop obstruction on CT (a C/U-shaped fluid-filled loop with converging mesenteric vessels) and signs of ischaemia — reduced or absent bowel-wall enhancement, wall thickening, mesenteric oedema and free fluid — are the warnings of strangulation.
- The transition point on CT (the junction of dilated and collapsed bowel) localises the obstruction and often reveals the cause.
- A competent ileocaecal valve in LBO produces a 'closed loop' between the valve and the obstruction, markedly raising the risk of caecal perforation — an important integration of anatomy and danger.
Provided image
SELF-CHECK
An abdominal X-ray shows several dilated, centrally placed bowel loops, each crossed by thin mucosal folds that span the full width of the lumen, measuring about 4 cm in diameter, with multiple air-fluid levels and no gas in the colon. What does this pattern indicate?
A. Large-bowel obstruction, because the loops are dilated beyond 3 cm
B. Small-bowel obstruction — central loops with valvulae conniventes crossing the full lumen, dilated >3 cm, with air-fluid levels and no distal colonic gas
C. Sigmoid volvulus arising from the pelvis
D. Normal bowel gas pattern
Reveal Answer
Answer: B. Small-bowel obstruction — central loops with valvulae conniventes crossing the full lumen, dilated >3 cm, with air-fluid levels and no distal colonic gas
Centrally placed loops with valvulae conniventes (folds crossing the FULL width of the lumen), dilated beyond about 3 cm, with multiple air-fluid levels and an absence of colonic gas, are characteristic of small-bowel obstruction. Large-bowel obstruction shows peripheral loops with haustra that do NOT cross the full lumen and different calibre thresholds (colon >6 cm, caecum >9 cm). A sigmoid volvulus produces a distinct coffee-bean loop from the pelvis, and this clearly abnormal dilatation is not a normal gas pattern.