Page 9 of 17
AS11.5-6 | Advanced Airway Indications and Mechanical Ventilation Settings — SDL Guide
CLINICAL SCENARIO
A 28-year-old motorcyclist is brought to the emergency department following a high-speed collision. He is unconscious, GCS 6, with a respiratory rate of 8 and SpO₂ 82% on a non-rebreather mask at 15 L/min. The trauma team leader calls for rapid sequence intubation. Within 90 seconds, an endotracheal tube is placed, cuff inflated, and connected to the mechanical ventilator. The respiratory therapist sets a tidal volume of 500 mL, respiratory rate of 14/min, PEEP 5 cmH₂O, and FiO₂ 0.6. Within five minutes SpO₂ rises to 99% and the team turns to the haemodynamic problem. Two hours later, the ICU doctor reviews the ventilator screen and adjusts the settings based on the arterial blood gas — PaCO₂ has risen to 58 mmHg and the plateau pressure is 32 cmH₂O. Each decision in this sequence — the indication to intubate, the ventilator settings, and the interpretation of the ABG — rests on a foundation of understanding that this module provides.
WHY THIS MATTERS
Advanced airway management — specifically, the indications for definitive airway placement and the principles of mechanical ventilation — is no longer confined to the anaesthesia and intensive care specialties. Every doctor in a referral hospital will encounter patients on mechanical ventilators; every emergency medicine trainee must be able to recognise when a patient needs intubation and initiate ventilation while waiting for anaesthesia or ICU support. The NMC 2024 CBME framework requires graduating students to enumerate the indications for advanced airway management (AS11.5) and to explain the principles and settings of mechanical ventilation (AS11.6). These are knowledge and understanding competencies — you are not expected to perform intubation independently at graduation, but you must be able to describe the steps in a simulated environment and to interpret the numbers on a ventilator screen. This module builds that foundational knowledge.
RECALL
Before proceeding, activate your knowledge from the preceding modules in this cluster. From the oxygen devices module (as11-oxygen-devices): recall the FiO₂ ranges of different delivery systems and the principle that a non-rebreather mask is the ceiling for spontaneously breathing patients — when the NRM is insufficient, mechanical ventilation replaces spontaneous effort. From the basic airway module (as11-basic-airway): recall the head-tilt chin-lift, jaw thrust, OPA, and NPA as the bridge to definitive airway placement. Also recall from Year-1 Physiology the key respiratory variables: tidal volume (VT, approximately 500 mL in a 70 kg adult), respiratory rate (RR, 12–16/min at rest), minute ventilation (VE = VT × RR, approximately 6–8 L/min), functional residual capacity (FRC), and the relationship between alveolar ventilation and PaCO₂. Understanding the ventilator settings requires you to hold these baseline values in mind.
Indications for Advanced Airway Management
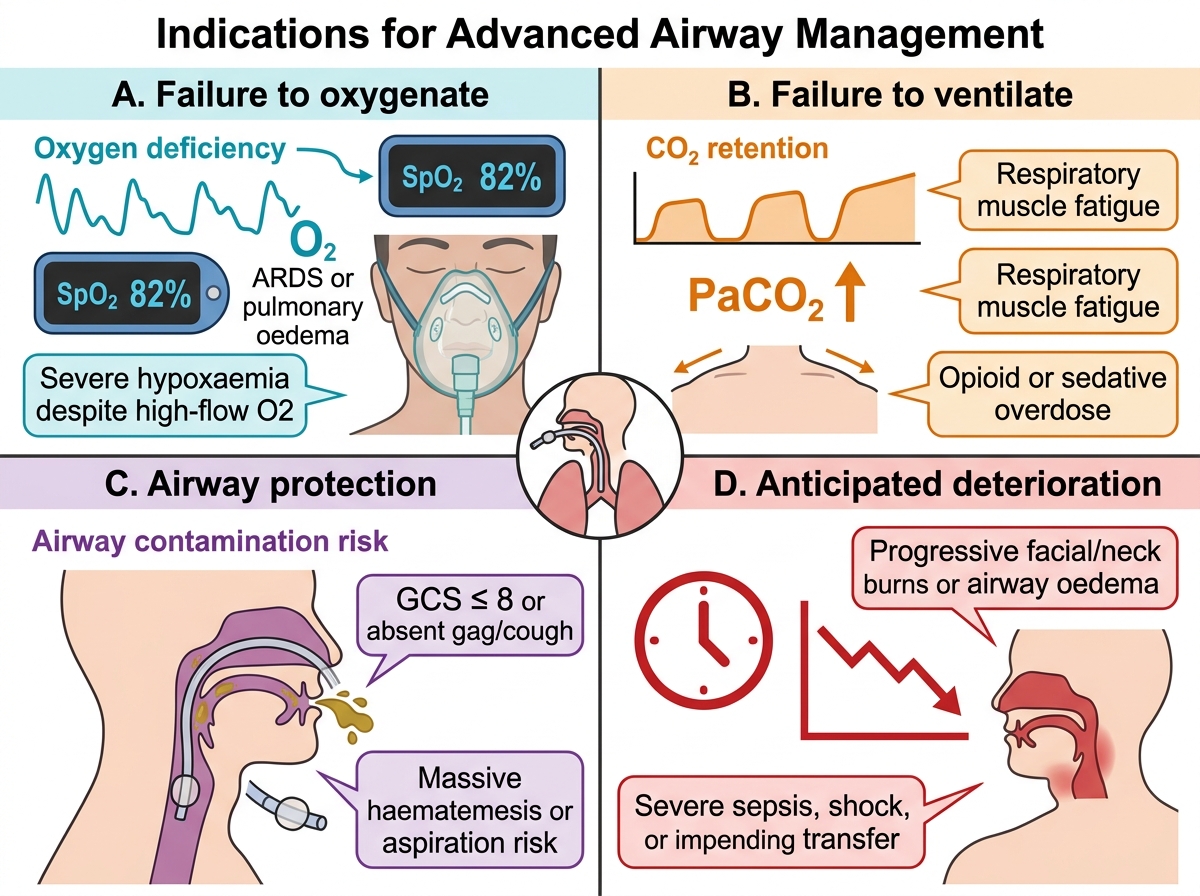
Advanced airway management encompasses the placement of a supraglottic airway device (such as a laryngeal mask airway) or a definitive airway (endotracheal tube or surgical airway) when basic manoeuvres and adjuncts are insufficient or inappropriate. The indications can be grouped into four categories, each reflecting a different failure mode of the unprotected airway.
The first and most urgent category is failure to oxygenate — the patient cannot maintain adequate SpO₂ (conventionally ≥90%) despite maximum non-invasive oxygen delivery (non-rebreather mask at 15 L/min or HFNC). This arises in severe pneumonia, ARDS, pulmonary oedema, massive pulmonary embolism, or any condition causing severe ventilation-perfusion mismatch or shunt. The second category is failure to ventilate — the patient cannot eliminate CO₂ adequately, causing progressive hypercapnia and respiratory acidosis. This occurs in neuromuscular disease (Guillain-Barré syndrome, myasthenic crisis), severe COPD exacerbation, chest trauma with flail chest, or excessive sedation. Hypercapnia itself is not a trigger for intubation unless it produces acidosis (pH <7.20–7.25) or is rising despite maximal non-invasive support.
The third category is airway protection — the patient cannot protect the airway from aspiration because of absent or severely impaired laryngeal reflexes. A GCS of 8 or below is the traditional threshold (the '8 = intubate' rule), though the quality of airway protection, not the GCS number alone, should guide the decision. The fourth category is anticipated deterioration or procedural need — the patient is not yet in extremis but is likely to deteriorate (severe trauma with haemorrhage, agitated severe head injury, impending airway oedema from burns, allergy, or angioedema) or requires airway control for a procedure (general anaesthesia).
Indications for Advanced Airway Management
Anatomy and Physiology Governing Endotracheal Intubation
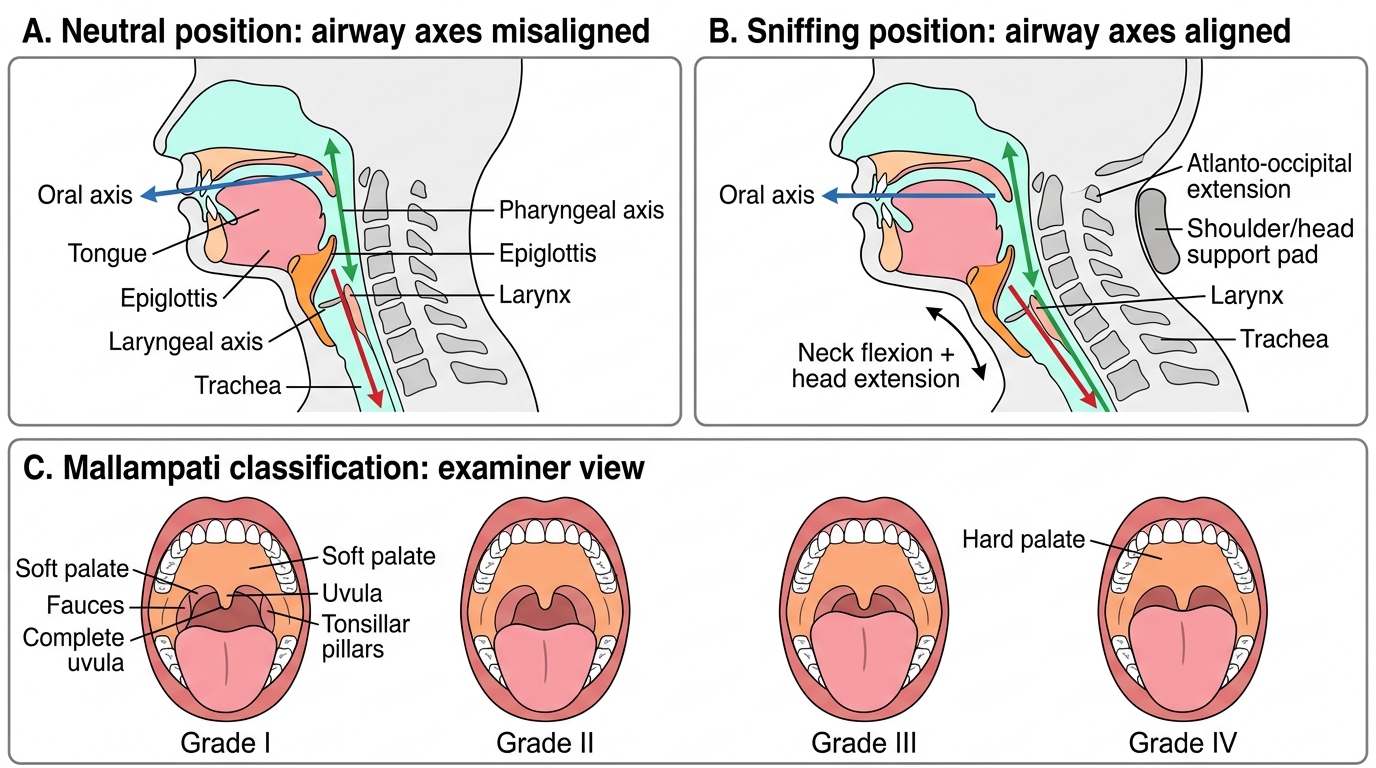
Endotracheal intubation involves passing a cuffed tube through the glottis and into the trachea under direct or video laryngoscopic vision. A precise understanding of the relevant anatomy is essential both to understand the procedure and to predict difficulty. The airway has a three-axis alignment challenge — the oral axis (mouth to pharynx), the pharyngeal axis (pharynx to larynx), and the laryngeal axis (larynx to trachea). Alignment of these three axes, classically achieved by placing the patient in the 'sniffing position' (head extension plus neck flexion by placing a pillow under the occiput), is what allows the laryngoscopist a line of sight from the mouth to the glottis.
The glottis (laryngeal inlet) is bounded anteriorly by the epiglottis, laterally by the aryepiglottic folds, and posteriorly by the arytenoid cartilages and the inter-arytenoid notch. The vocal cords are the anterior landmark. Successful intubation requires visualising the posterior commissure of the larynx (the arytenoids and inter-arytenoid notch) and passing the tube between the cords under vision.
The Mallampati classification grades the oropharyngeal view with the patient seated, mouth fully open, and tongue maximally protruded without phonation:
• Class I — soft palate, uvula, tonsillar pillars, and full fauces visible
• Class II — soft palate, uvula, and tonsillar pillars visible
• Class III — soft palate and base of uvula only
• Class IV — soft palate not visible
Mallampati III and IV predict difficult laryngoscopy. Other predictors of difficult intubation include limited mouth opening (<3 cm / 2 finger-breadths), short thyromental distance (<6 cm / 3 finger-breadths), limited neck extension, BMI >35, and a history of previous difficult intubation. The LEMON mnemonic (Look externally, Evaluate 3-3-2 rule, Mallampati, Obstruction/Obesity, Neck mobility) systematises the difficult airway assessment.
A critical anatomical distinction: the ASA classification (I–VI) grades systemic disease severity; the Mallampati score grades anticipated airway difficulty. They are entirely different scales assessing different parameters — do not conflate them.
Airway Axis Alignment and Mallampati Classification
Steps of Endotracheal Intubation: Overview for Demonstration
The NMC 2024 competency AS11.5 requires students to describe the steps and demonstrate in a simulated environment. The following is a stepwise description of orotracheal intubation under direct laryngoscopy, consistent with the approach described in Morgan & Mikhail's Clinical Anesthesiology and Ajay Yadav's Short Textbook of Anaesthesia. Students are expected to be able to narrate these steps and perform them on a manikin under supervision — not to perform unsupervised intubation in a clinical setting.
Pre-oxygenation (already covered in as11-oxygen-devices): Apply NRM at 15 L/min for 3–5 minutes to fill the FRC with oxygen, maximising safe apnoea time. For rapid sequence induction (RSI), this step cannot be abbreviated.
Drug administration: In RSI, an induction agent (e.g., propofol 1.5–2.5 mg/kg or ketamine 1–2 mg/kg) is given to produce unconsciousness, immediately followed by a muscle relaxant (suxamethonium 1–1.5 mg/kg for RSI, rocuronium for modified RSI). A second provider applies cricoid pressure (Sellick's manoeuvre) at induction to compress the oesophagus and prevent passive regurgitation, though the evidence base for this manoeuvre is debated.
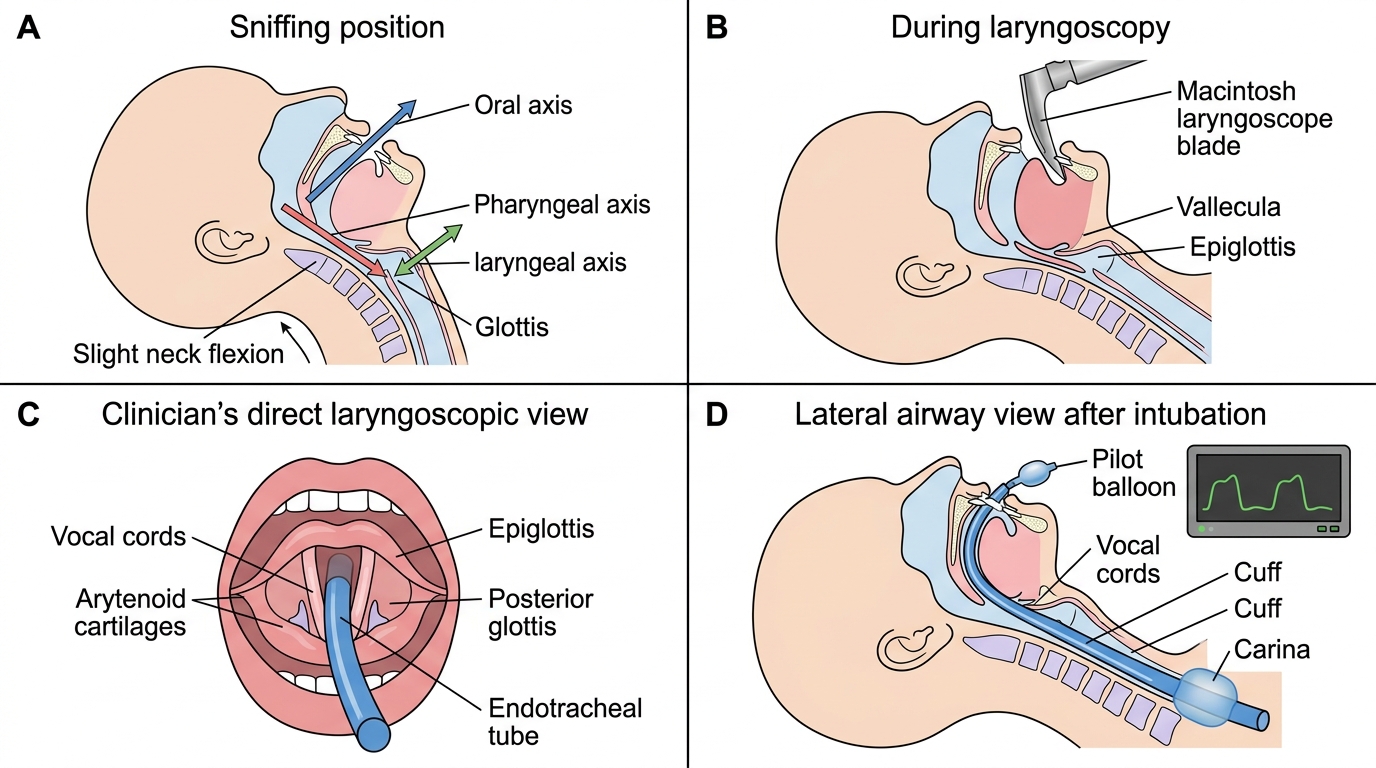
Laryngoscopy and tube placement: Place the patient in the sniffing position. Insert the laryngoscope blade into the right side of the mouth and sweep the tongue to the left. Advance the curved (Macintosh) blade into the vallecula (between the tongue base and epiglottis) and lift the laryngoscope in the direction of the handle — this lifts the epiglottis and exposes the glottis. Pass a cuffed tube (typically size 7.0–7.5 mm internal diameter for adult women, 7.5–8.0 mm for adult men) through the cords under direct vision until the cuff passes 2–3 cm below the vocal cords. Inflate the cuff (typically 5–10 mL of air) to achieve a sealing pressure.
Confirmation: Attach a BVM or ventilator circuit. Confirm placement by: (1) direct vision of tube passing cords; (2) capnography — the gold standard, showing a CO₂ waveform; (3) bilateral chest auscultation and absence of epigastric sounds; (4) bilateral chest rise; (5) chest X-ray to confirm tip position (2–5 cm above carina, approximately at the level of the carina on a portable AP CXR at T4–T6).
Securing the tube: Secure the ETT at the labelled depth (typically 21–23 cm at the teeth in adults) with tie or proprietary holder.
Steps of Orotracheal Intubation