Page 11 of 17
AS11.5-6 | Advanced Airway Indications and Mechanical Ventilation Settings — SDL Guide (Part 3)
Applied and Supervised Practice: Simulation and Ventilator Familiarisation
The AS11.5 and AS11.6 competencies specify simulation as the context for demonstrating advanced airway management and ventilation principles — you are not expected to independently intubate patients or programme ventilators without supervision, but you must be able to perform these tasks on a manikin and to explain the reasoning behind each decision to your supervising clinician. The simulation environment serves a dual purpose: it is where you build the mental schemata that allow rapid, accurate action when you encounter these scenarios as a houseman or junior resident, and it is also where errors are caught and corrected safely — before a real patient is harmed. Research in clinical education shows that students who receive structured simulation practice with immediate corrective feedback on intubation and ventilation skills are substantially better prepared for their first supervised clinical exposure than those who have only observed. Use the checklists below as your simulation preparation guide — work through each item in the skills lab before your anaesthesia or ICU clinical posting, and note any item you cannot perform confidently as a target for focused revision.
For the intubation simulation (AS11.5), ensure you can:
1. State all four indications for intubation fluently and give a clinical example for each
2. List the five confirmation methods for ETT placement in order of reliability (capnography first)
3. Perform laryngoscopy on a manikin, identifying the epiglottis, vallecula, and vocal cords
4. Describe Mallampati grading from a clinical photograph
5. Explain Sellick's manoeuvre and state the current evidence debate around it
For the mechanical ventilation simulation (AS11.6), ensure you can:
1. State the initial VT (6–8 mL/kg IBW), calculate IBW for a 175 cm male, and select the starting VT
2. Set RR, PEEP, and FiO₂ for a trauma patient with bilateral lung contusions
3. Interpret a mock ABG result (PaCO₂ 62, pH 7.28, PaO₂ 76 on FiO₂ 0.5) and state which ventilator parameter to adjust
4. Identify what plateau pressure of 36 cmH₂O means and what action to take
5. Distinguish between peak pressure and plateau pressure on a ventilator screen and explain what each reflects
In your clinical exposures in the anaesthesia theatre and ICU, observe every ventilator screen you encounter. Try to read the settings before the consultant explains them, then listen to the rationale. This active preparatory practice is the single most effective way to build the clinical pattern recognition that converts knowledge into competence.
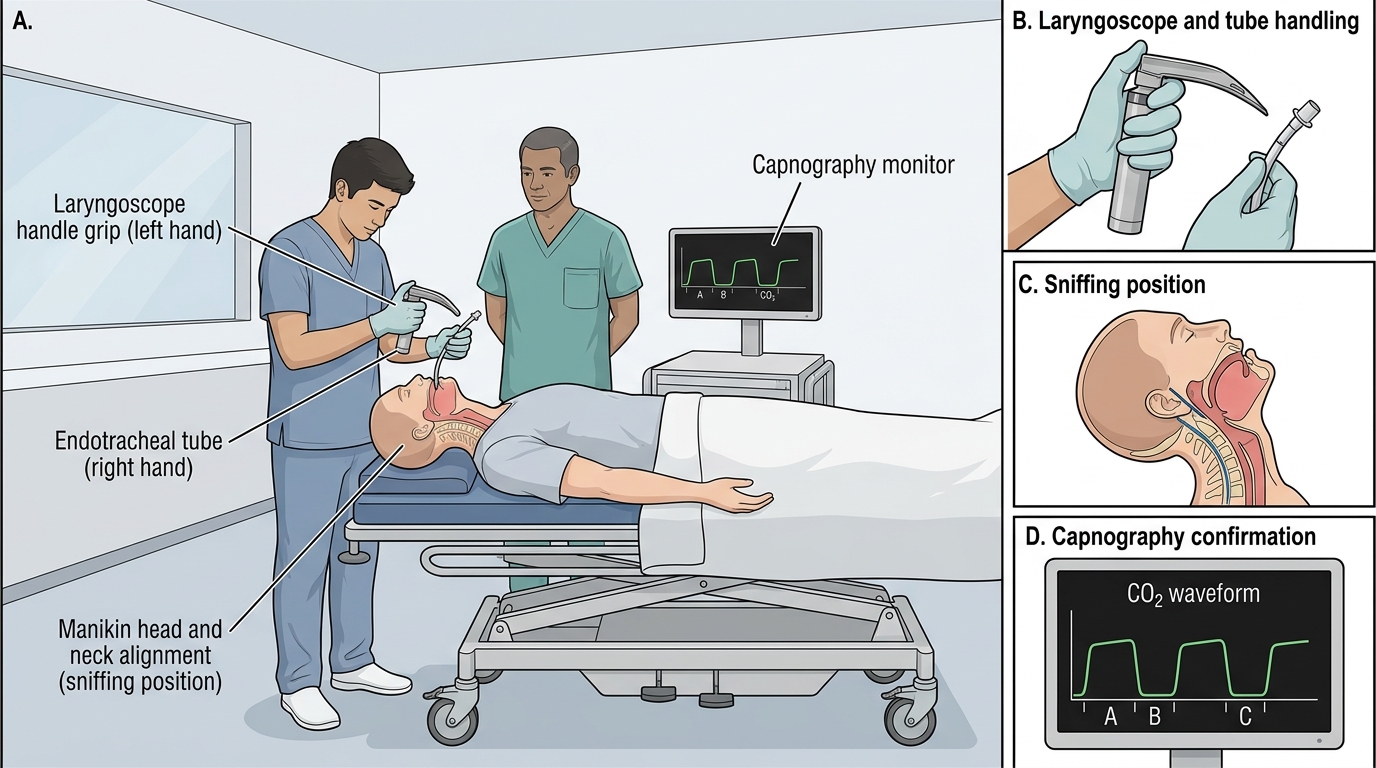
Direct Laryngoscopy: Technique and Confirmation
Self-Assessment: Advanced Airway and Ventilation Decision-Making
This self-assessment section is designed to test your integration of advanced airway indications, ventilator parameters, and ABG-guided management into a clinical reasoning framework. By the end of this module you should be able to: enumerate the four indications for intubation; describe the steps of RSI; set initial ventilator parameters for a new intubation; interpret an ABG and adjust the ventilator accordingly; and recognise a dangerous plateau pressure and take corrective action. These are the knowledge and understanding components of AS11.5 and AS11.6, and they will be tested in written examinations, OSCEs, and clinical vivas. Work through the questions below before checking the explanations, and for each one articulate the full chain of reasoning — the physiological principle, the clinical implication, and the management action — rather than just recalling the answer.
Consolidation questions:
1. A 70 kg (IBW) man is intubated for GCS 6 following a head injury. What VT do you set? What RR gives a starting minute ventilation of approximately 7 L/min?
2. An ABG 30 minutes after intubation shows PaCO₂ 65 mmHg, pH 7.24, PaO₂ 88 mmHg on FiO₂ 0.5. What is the primary problem? Which ventilator parameter do you adjust, and in which direction?
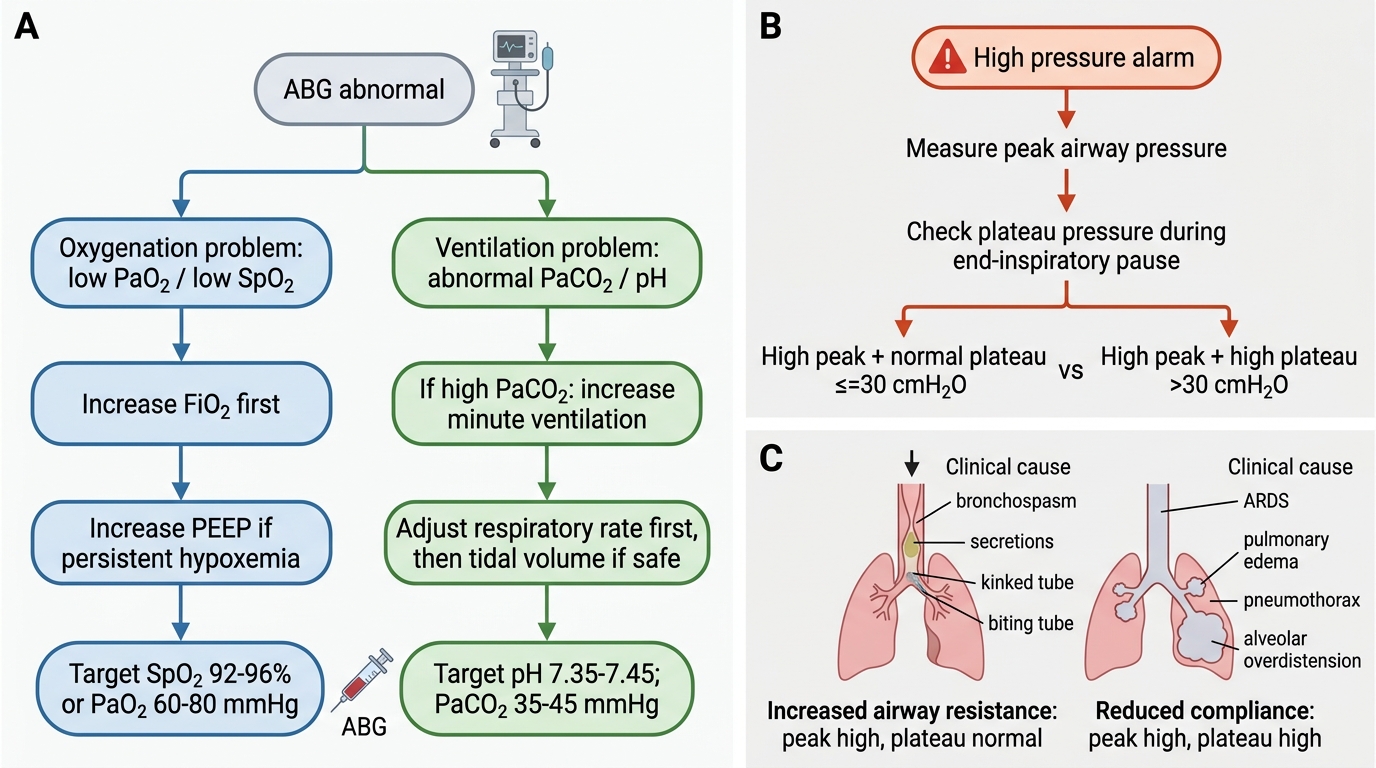
3. The ventilator alarm shows a peak inspiratory pressure of 42 cmH₂O. The plateau pressure is 28 cmH₂O. What does this combination tell you about the cause?
4. Why is IBW — not actual weight — used to calculate tidal volume? What error results from using actual weight in a patient who weighs 110 kg and has an IBW of 70 kg?
5. A patient with ARDS on PEEP 10 cmH₂O has SpO₂ 88% and PaO₂ 58 mmHg on FiO₂ 0.7. What are the two options for improving oxygenation, and which should you adjust first?
For question 3, the distinction between elevated peak pressure (airway resistance problem: bronchospasm, secretions, biting) and elevated plateau pressure (compliance problem: pneumothorax, ARDS, fluid overload) is a high-yield exam and clinical viva point — know it precisely.
Decision Tree for Ventilated Patient Management
SELF-CHECK
A mechanically ventilated patient has a peak airway pressure of 40 cmH₂O and a plateau pressure of 22 cmH₂O. What is the most likely cause of the elevated peak pressure?
A. Reduced lung compliance from ARDS
B. Increased airway resistance (e.g., bronchospasm or secretion plug)
C. Pneumothorax causing tension
D. Ventilator-induced lung injury with alveolar overdistension
Reveal Answer
Answer: B. Increased airway resistance (e.g., bronchospasm or secretion plug)
The plateau pressure (measured during an end-inspiratory pause — no flow) reflects alveolar distending pressure and is therefore a measure of respiratory compliance. The peak pressure includes both the compliance and resistance components. When peak pressure is high but plateau pressure is normal (≤30 cmH₂O), the elevated peak is caused by increased airway resistance — the gas is meeting resistance getting to the alveoli, but once it arrives the alveoli are not overdistended. Common causes: bronchospasm, secretion plug, kinked or compressed tube, or the patient biting the tube. Reduced compliance from ARDS or pneumothorax would raise both peak AND plateau pressure. Ventilator-induced lung injury is a consequence of high plateau pressure, not a cause of isolated peak pressure elevation.
CLINICAL PEARL
IBW for VT calculation is non-negotiable. A 110 kg patient with an IBW of 70 kg and a lung size appropriate for 70 kg will sustain ventilator-induced lung injury if you set VT based on actual weight (8 mL × 110 = 880 mL rather than 8 × 70 = 560 mL). The ARMA trial (ARDS Network 2000) demonstrated a 22% absolute mortality reduction with 6 mL/kg IBW versus 12 mL/kg — the most dramatic survival benefit ever shown in critical care ventilation. Memorise the IBW formulae and calculate before you set the ventilator, every time.