Page 6 of 17
AS11.3-4 | Basic Airway Opening and Airway Adjunct Insertion — SDL Guide (Part 2)
Oropharyngeal Airway (Guedel): Selection, Insertion, and Verification
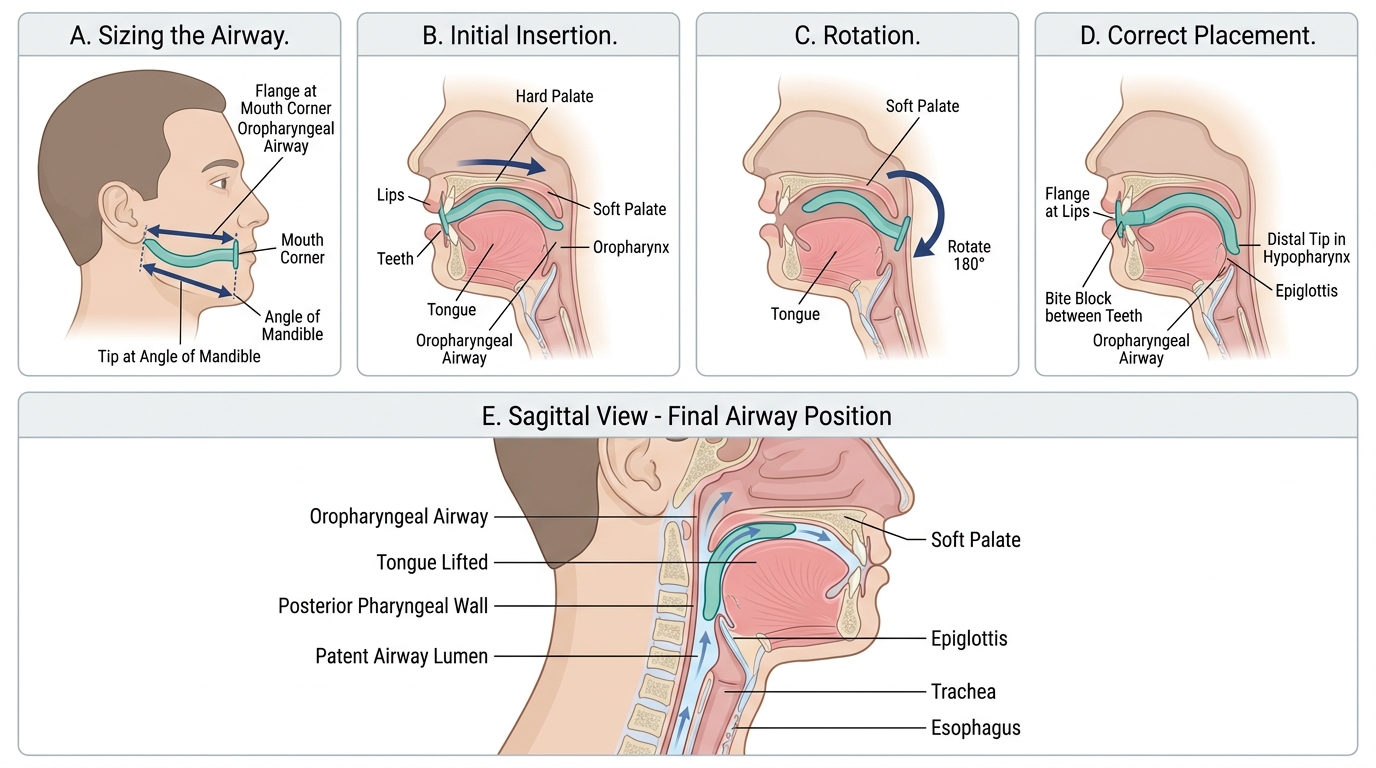
The oropharyngeal airway (OPA), also called the Guedel airway, is a curved rigid plastic airway adjunct that holds the tongue away from the posterior pharyngeal wall by passing over the tongue through the mouth. It has a flange at the proximal end (which rests against the teeth or lips), a bite block in the mid-portion (preventing occlusion if the patient bites down), and a curved distal portion whose tip rests in the hypopharynx behind the tongue base.
Sizing — the correct size is critical. An OPA that is too small will push the tongue back further and worsen obstruction; one that is too large will depress the epiglottis onto the laryngeal inlet, causing complete obstruction. The correct size is estimated by measuring the distance from the centre of the patient's mouth (or the angle of the mouth) to the angle of the jaw (earlobe in some references). In adults, sizes are typically 80–100 mm (small), 90 mm (medium female), 100 mm (medium male), and 110 mm (large male). Always confirm by visually matching the airway to the patient's anatomy before insertion.
Insertion technique (adult): open the patient's mouth using a crossed-fingers technique (thumb on upper teeth, index finger on lower teeth, crossed and spread apart); insert the OPA with the curve pointing towards the palate (concave side upward, i.e., inverted); advance it until it reaches the junction of the hard and soft palate; then rotate the airway through 180° so the concave side now faces the tongue and the tip slides over the tongue into the hypopharynx. An alternative technique, particularly in children (where rotation risks trauma to the soft palate), is to use a tongue depressor to hold the tongue down while inserting the airway in the anatomical position (concave side toward the tongue) from the outset — the rotation method is NOT used in children.
Contraindications and complications:
• Contraindicated in the conscious or semi-conscious patient with an intact gag reflex — will stimulate vomiting and laryngospasm
• Dental injury if inserted without proper technique
• Mucosal trauma during insertion if too forceful
• Pressure necrosis on the tongue or lip if left in situ for prolonged periods
Adult Oropharyngeal Airway Insertion
Nasopharyngeal Airway: Selection, Insertion, and Advantages
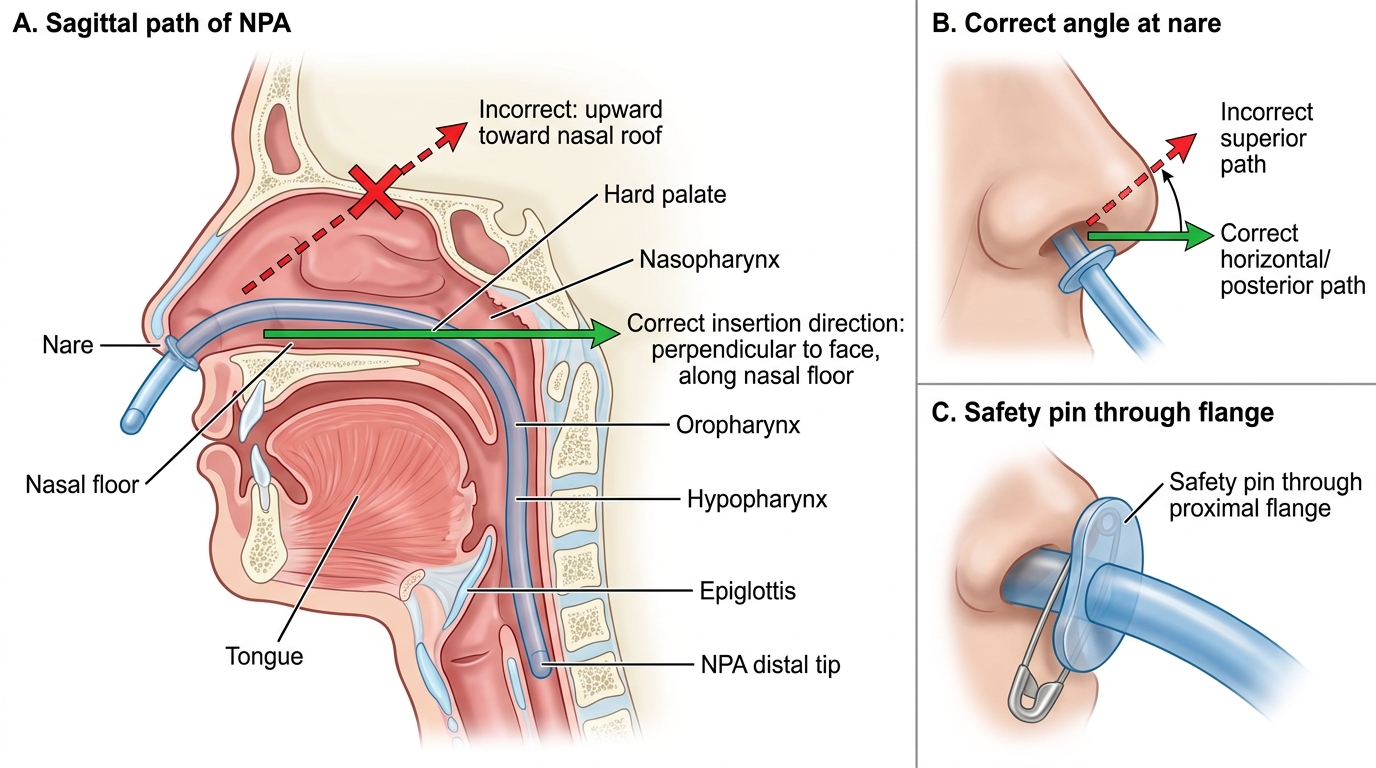
The nasopharyngeal airway (NPA) is a soft, flexible rubber or plastic tube inserted through a nare and passed along the floor of the nasal passage to sit with its tip in the hypopharynx, just above the epiglottis. Unlike the OPA, the NPA bypasses the oral cavity and can be used in patients who are semi-conscious or who have an intact gag reflex — it does not stimulate the gag reflex significantly and is far better tolerated in the lightly sedated or post-ictal patient.
Sizing — the correct NPA size is estimated by measuring the distance from the tip of the nose to the tragus of the ear (this approximates the length of the nasopharyngeal airway path). The internal diameter should be the largest that fits comfortably into the nostril without blanching the skin. In adults, sizes 6–7 mm are typical for women, 7–8 mm for men. Size is typically printed on the tube as internal diameter in millimetres.
Insertion technique: select the right nostril if possible (usually larger), or the left if the right is obstructed; lubricate the tube generously with water-soluble lubricant or lignocaine gel (reduces trauma and the sensation that promotes sneezing); insert the tube perpendicular to the face (NOT angled upward toward the vertex — this is the commonest error and leads to insertion into the middle turbinate); advance steadily with a slight rotating motion along the floor of the nasal passage; if resistance is met at the turbinates, try gentle rotation — if firm resistance persists, withdraw and try the other nostril; advance until the flange (or safety pin fixed through the proximal end to prevent the tube disappearing into the nostril) rests against the nare. Confirm correct placement by feeling air movement through the tube with spontaneous breathing.
Advantages over OPA:
• Tolerated in semi-conscious patients with intact gag reflex
• Can be used when mouth opening is limited (trismus, jaw fracture, angioedema)
• Easier to maintain in an agitated patient
Contraindications:
• Suspected basal skull fracture (blood or CSF from nares, Battle's sign, peri-orbital bruising) — risk of intracranial placement
• Bleeding diathesis or anticoagulation — high risk of epistaxis
• Known nasal polyps or significant nasal obstruction
Nasopharyngeal Airway Insertion Technique
Monitoring and Confirming Airway Patency
Inserting an airway adjunct is only the first step — confirming that the airway is patent and the patient is ventilating adequately is equally important, and failure to monitor after adjunct placement is a documented cause of preventable harm. An improperly sized OPA can worsen obstruction rather than relieve it; an NPA inserted too shallowly rests above the obstruction and achieves nothing; and even a correctly placed adjunct can become displaced if the patient moves. The key monitoring parameters after any basic airway intervention are both clinical and instrumental. They must be assessed immediately after the intervention, not minutes later, and checked again every 1–2 minutes thereafter until a definitive airway is secured or the patient regains consciousness with intact protective reflexes. The importance of a structured post-intervention assessment cannot be overstated: many documented cases of preventable airway deterioration occur not during the initial intervention but in the minutes immediately after, when the clinician has stepped back assuming the problem is resolved.
Clinical confirmation of airway patency:
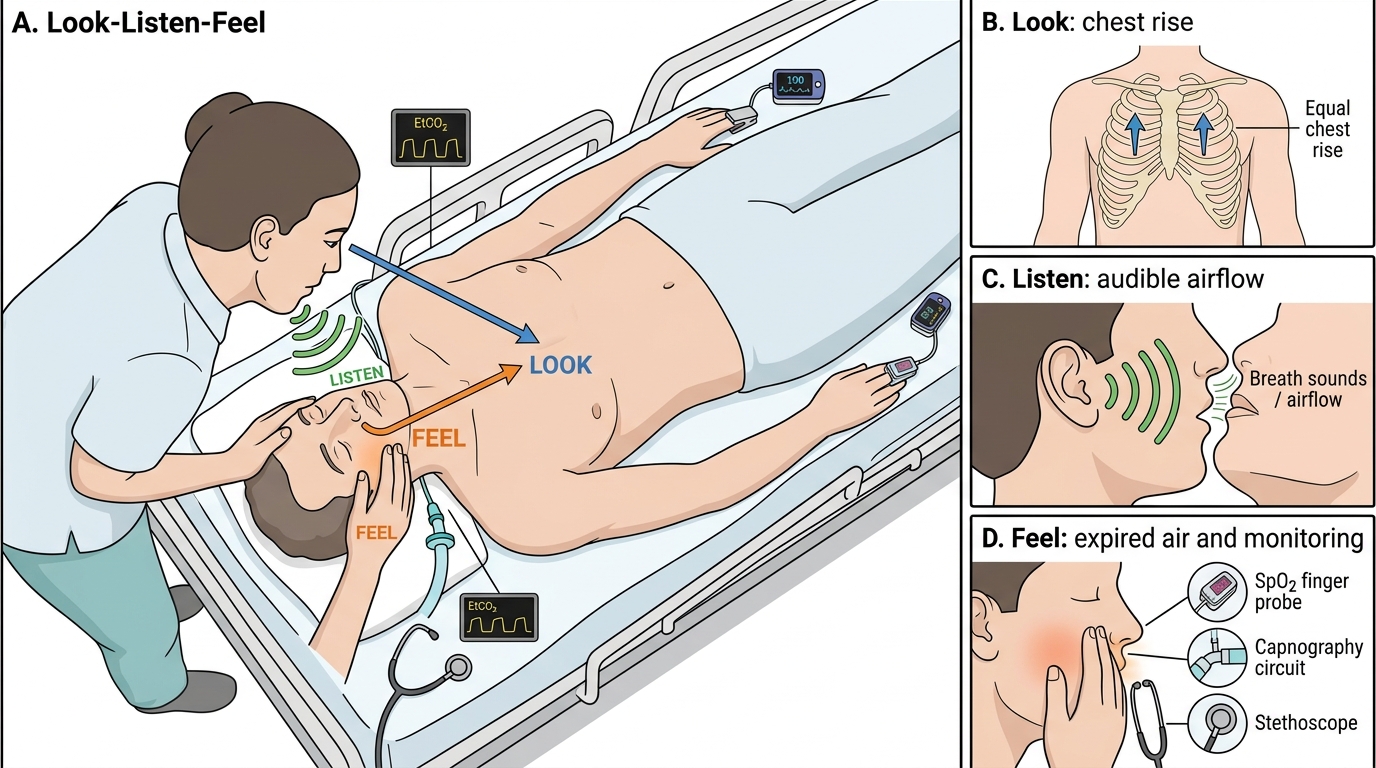
• Look — is the chest rising and falling symmetrically with each breath? Paradoxical or asymmetrical movement suggests the airway is still obstructed or there is a pneumothorax.
• Listen — is there any residual snoring, gurgling, or stridor? Complete silence with no chest movement indicates apnoea or complete obstruction. Quiet, regular air entry sounds (heard with or without stethoscope over the neck) indicate patency.
• Feel — place the back of the hand near the mouth and nose; feel for warm, moist expired air with each exhalation. If an NPA is in situ, feel for air movement from the proximal opening.
Instrumental monitoring:
• Pulse oximetry (SpO₂) — the most important single monitor; trend of SpO₂ over 60–90 seconds after airway opening indicates effectiveness
• End-tidal CO₂ (EtCO₂) via capnography — confirms ventilation definitively; a waveform indicates CO₂ is being exhaled (the airway is patent and the lungs are ventilating). Particularly valuable if the patient is being ventilated via BVM.
• Respiratory rate — observe over 60 seconds
When to escalate: If basic manoeuvres and adjuncts fail to maintain SpO₂ ≥90% or the patient cannot protect their airway (pooling secretions, repeated vomiting), the next step is bag-valve-mask ventilation followed by definitive airway placement (supraglottic airway device or tracheal intubation). Basic airway skills are a bridge, not a destination — escalate promptly if they are insufficient.
Look-Listen-Feel Airway Assessment