Page 7 of 17
AS11.3-4 | Basic Airway Opening and Airway Adjunct Insertion — SDL Guide (Part 3)
Applied and Supervised Practice: Simulation and Clinical Integration
The NMC 2024 competency framework specifies that AS11.3 and AS11.4 must be demonstrated in a simulated environment — meaning that you should practise these techniques on a manikin before encountering a real patient. Simulation-based training for airway skills is not merely pedagogically preferred; it is ethically mandatory, because the potential for harm from an incorrectly performed jaw thrust in a trauma patient or an incorrectly sized OPA is immediate. Research in clinical education consistently demonstrates that manikin-based deliberate practice with structured feedback — including immediate correction of technique errors — produces significantly better retention and skill transfer than passive observation alone.
During your simulation session, practise each of the following in sequence, having a colleague or instructor observe and provide immediate feedback:
1. Head-tilt chin-lift: confirm head position, confirm use of bony chin, confirm airway is open by observing simulated chest rise
2. Jaw thrust: position both hands correctly at the mandibular angles, confirm anterior displacement without neck extension
3. OPA sizing: measure corner-of-mouth to angle-of-jaw on the manikin; select the appropriate size from the available range; insert with the inversion-and-rotation technique; confirm seated position
4. NPA sizing: measure tip-of-nose to tragus; lubricate; insert perpendicular to the face along the nasal floor; confirm movement of air through the tube
5. Combine OPA with bag-valve-mask: maintain chin lift while applying a one-person mask seal (E-C clamp technique) and compressing the bag
In the clinical setting, your supervised practice opportunities will arise in the recovery room (post-anaesthesia airway management), the emergency department resuscitation bay, and during anaesthesia induction exposure in the operating theatre. In each setting, always observe before you do, ask permission, and debrief with your supervising anaesthetist immediately after.
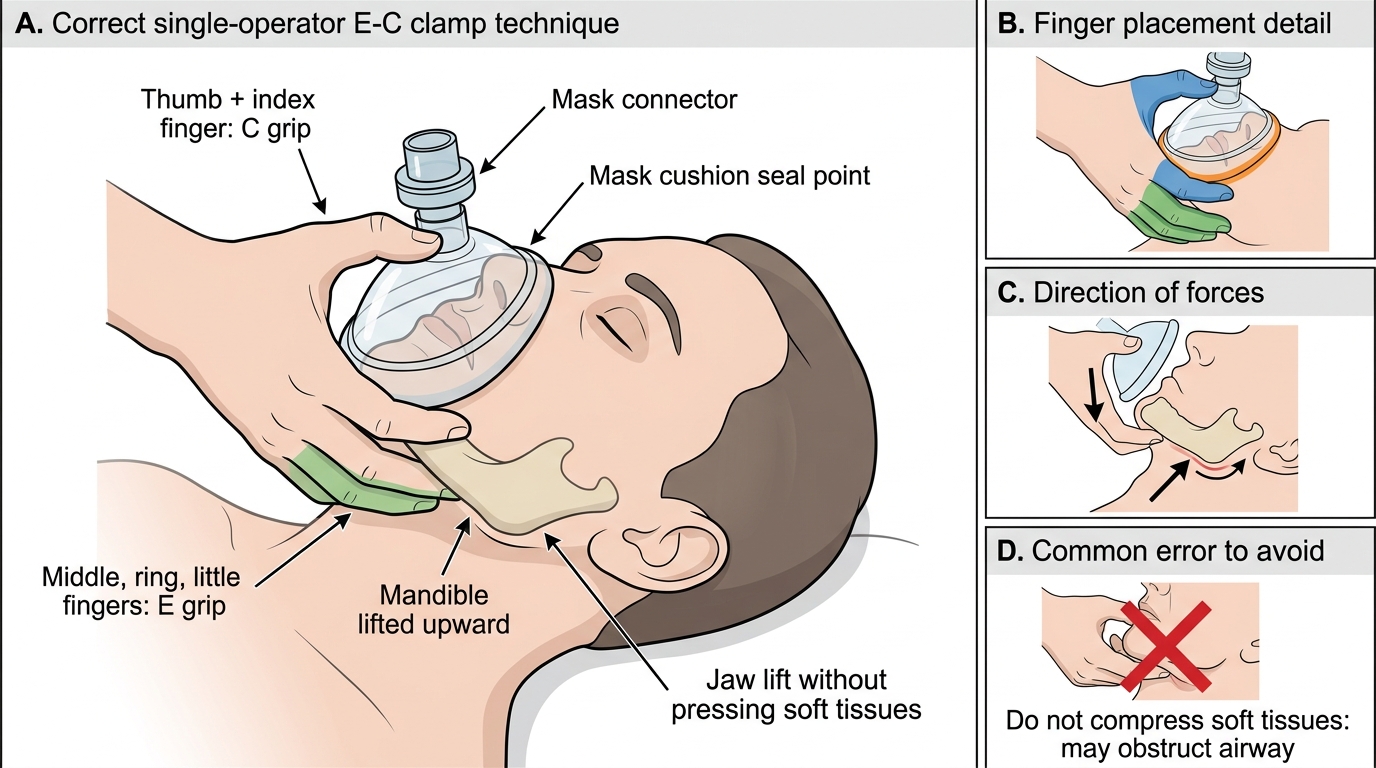
E-C Clamp Technique for Bag-Valve-Mask Ventilation
Self-Assessment: Integrating Technique, Indication, and Clinical Judgement
This self-assessment section consolidates the clinical, anatomical, and technical knowledge from this module into a decision-making framework that you can apply under pressure in real clinical settings. Competence in basic airway management requires three simultaneous capabilities: recognising the indication immediately when you encounter a patient with noisy, laboured, or absent breathing; selecting the right manoeuvre or adjunct for the specific clinical context, considering cervical spine status, level of consciousness, and oral anatomy; and executing the chosen technique correctly with immediate verification of its effectiveness. These three capabilities must eventually operate automatically and in parallel — the pause for deliberate reasoning that is normal and appropriate during learning becomes dangerous hesitation in a real airway emergency. The only way to build this automaticity is through deliberate practice, structured self-testing, and repeated exposure in simulation before clinical posting. Use the questions below as a structured self-test: attempt each question fully before reading ahead, and for every answer articulate the anatomical or physiological rationale, not just the conclusion.
Test yourself on the following decision points:
1. A post-ictal adult patient is snoring on his side in the emergency department. He responds to voice but not commands. His SpO₂ is 88%. Which airway adjunct is preferred — OPA or NPA? Why?
2. A trauma patient arrives after a road traffic accident with suspected cervical spine injury and gurgling breathing. Which airway manoeuvre is used? What is explicitly avoided?
3. You insert a size 100 mm Guedel airway in an adult male and the snoring continues. What went wrong? What do you check?
4. After inserting an NPA, you feel no airflow from the proximal end. What are the two most likely explanations, and what do you do for each?
5. A 3-year-old child needs an OPA. How does your insertion technique differ from the adult technique, and why?
For each question, state the answer, the anatomical or physiological rationale, and the immediate next step if your first intervention fails. This three-part response reflects the depth of understanding that the CBME framework requires — not just 'what' to do, but 'why' and 'what next'.
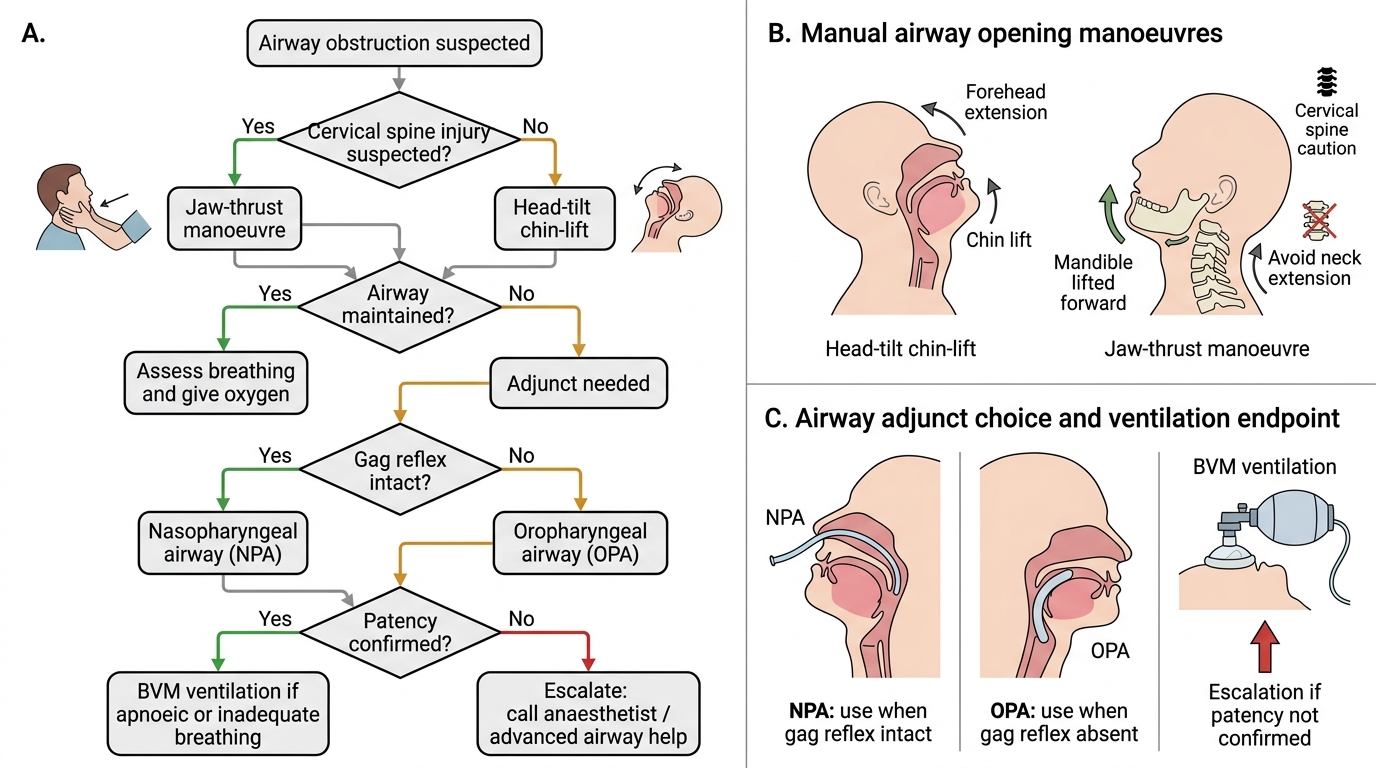
Basic Airway Management Decision Algorithm
SELF-CHECK
A 45-year-old woman who received intravenous midazolam for an endoscopic procedure is transferred to the recovery room and immediately becomes snoring and apnoeic. She has no known cervical spine injury. Which is the FIRST correct action?
A. Insert a nasopharyngeal airway immediately
B. Call the anaesthetist and wait for the difficult airway trolley
C. Perform a head-tilt chin-lift and assess for return of breathing
D. Insert a size 100 mm Guedel airway with the rotation technique
Reveal Answer
Answer: C. Perform a head-tilt chin-lift and assess for return of breathing
The first action for any airway obstruction without suspected cervical spine injury is the head-tilt chin-lift manoeuvre — it is immediate, requires no equipment, and is the standard first-line response (Morgan & Mikhail, Ajay Yadav). Only after confirming whether the manoeuvre restores breathing is an adjunct considered. Inserting an OPA or NPA as the first step skips the initial manual assessment. Calling for help is important but not the FIRST action — the clinician present must act immediately. In a midazolam-sedated patient with reduced level of consciousness, if the head-tilt chin-lift restores breathing, an NPA may then be inserted to maintain the airway (preferred over OPA if the patient has any preserved gag reflex).
CLINICAL PEARL
The gag reflex is your OPA/NPA decision gate. If a patient tolerates an OPA (does not gag or cough on it), the gag reflex is sufficiently obtunded and the OPA will work safely. If the patient gags or retches on OPA insertion, switch immediately to an NPA — the NPA bypasses the gag reflex trigger zone at the posterior tongue. Never persist with OPA insertion in a gagging patient; vomiting with a compromised airway is a life-threatening complication. A practical bedside test: try touching the posterior tongue gently with a gloved finger — if no gag, OPA is safe; if strong gag, use NPA.