Page 4 of 15
AS3.2-3 | Pre-anaesthetic History, Medication Review and Clinical Examination Documentation — SDL Guide
CLINICAL SCENARIO
You are the on-call anaesthesiology resident asked to review a 48-year-old woman on the surgical ward at 10 pm. She is listed first on tomorrow's elective list for a laparoscopic cholecystectomy. Her ward notes mention 'hypertension, on some tablets, no known allergies.' That is all the information you have. You have 30 minutes to take a complete pre-anaesthetic history, review her medications, perform a focused clinical examination, and produce a written anaesthetic assessment that will safely guide the team tomorrow morning. This module teaches you exactly how to do that — systematically, efficiently, and without missing the clinical details that could make the difference between a smooth anaesthetic and an intraoperative emergency.
WHY THIS MATTERS
The pre-anaesthetic history and clinical examination are the anaesthesiologist's primary diagnostic tools. Unlike a cardiologist who can rely on echocardiography or a physician who has weeks to investigate a new finding, the anaesthesiologist must synthesise a complete risk picture — often in a single focused encounter the evening before surgery. The quality of the history, medication review, and clinical documentation directly determines the safety of every decision made in the operating room: the choice of induction agent, the airway management strategy, the monitoring level, and the plan for postoperative pain and recovery. For a final-year MBBS student, mastering this structured assessment builds the clinical communication and documentation skills that underpin safe practice across every surgical specialty.
References: Morgan & Mikhail's Clinical Anesthesiology; Ajay Yadav's Short Textbook of Anaesthesia; ASA Practice Advisory for Preanesthesia Evaluation (2012, reaffirmed 2019).
RECALL
Before proceeding, recall: (1) the seven domains of a complete medical history — presenting complaint, history of presenting illness, past medical history, drug history and allergies, family history, social history, and systems review; (2) the purpose of the anaesthetic preoperative evaluation — identifying and optimising risk before the patient enters the operating room; (3) the basic structure of the cardiovascular and respiratory examinations as taught in clinical methods; (4) the concept of informed consent — the patient must understand what anaesthesia involves, its risks, and the alternatives before agreeing to proceed.
Clinical Indication and Relevance of the Pre-anaesthetic Assessment
The pre-anaesthetic assessment is a structured clinical encounter performed before any anaesthetic procedure, with the explicit purpose of creating a personalised, risk-stratified plan for a specific patient undergoing a specific procedure. It is not a generic medical clerking — every question asked and every examination finding recorded must be interpreted in the context of what anaesthesia will do to this patient.
The indication for a thorough pre-anaesthetic assessment applies to every patient, regardless of the procedure's perceived simplicity. Even a short procedure under local anaesthesia can become an emergency requiring airway management or resuscitation. The assessment is the anaesthesiologist's only opportunity to identify and act on conditions that would otherwise cause harm during or after anaesthesia.
The clinical relevance of the pre-anaesthetic history is twofold. First, it identifies anaesthetic-relevant risk factors — conditions that directly affect the choice of anaesthetic technique, drug selection, monitoring level, and postoperative disposition. Second, it establishes communication and consent — the patient receives clear information about what to expect, what to do on the day of surgery (fasting, medications), and what risks are relevant to their individual situation. This communication is both ethically required and practically protective: patients who understand their anaesthetic plan have better outcomes and fewer complaints.
The pre-anaesthetic assessment is documented as a formal anaesthetic pre-assessment record — a structured written note that becomes part of the patient's medical record, informs all operating theatre staff, and serves as a medicolegal record if a complication occurs. In most hospitals, this note includes the ASA classification, airway assessment findings, relevant comorbidities, medication plan, fasting instruction, and the proposed anaesthetic technique.
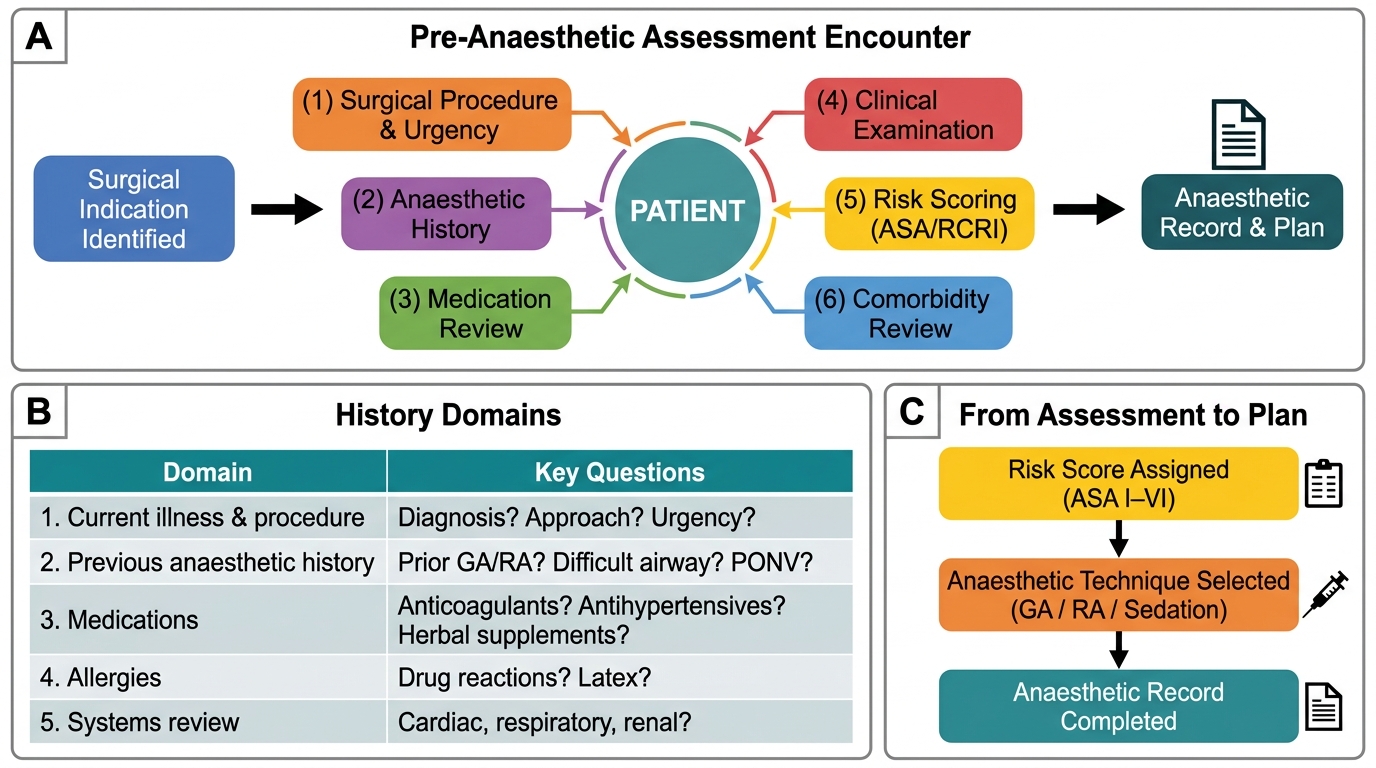
The Pre-Anaesthetic Assessment Encounter: Flow, Domains, and Output
Structured Pre-anaesthetic History: Domains and Key Questions
The pre-anaesthetic history has a specific structure that differs from a general medical clerking in its emphasis on anaesthetic-relevant information. Each domain serves a defined purpose in generating the anaesthetic plan.
Domain 1: Current illness and planned procedure. What is the surgical diagnosis? What operation is planned, by which approach (open or laparoscopic)? Is this elective, urgent, or emergency? The urgency determines how much time is available for optimisation. The planned procedure determines the physiological demands and the likely blood loss, duration, and postoperative pain burden.
Domain 2: Previous anaesthetic history. This is the most anaesthesia-specific domain of the history. Ask: Have you had a general or regional anaesthetic before? If yes, was there any problem? Specifically ask about: difficult intubation or airway management (the patient may have been told 'your airway was difficult'), postoperative nausea and vomiting (PONV), prolonged recovery or 'waking up very slowly', awareness under anaesthesia, and any adverse reactions to anaesthetic drugs. A family history of anaesthetic problems must also be elicited — this screens for malignant hyperthermia (autosomal dominant, triggered by volatile agents and suxamethonium; presents with hyperthermia, muscle rigidity, tachycardia, rhabdomyolysis, and is treated with dantrolene) and pseudocholinesterase deficiency (hereditary; causes prolonged neuromuscular blockade with suxamethonium — 'suxamethonium apnoea').
Domain 3: Past medical and surgical history. Document all medical conditions, particularly: cardiac disease (ischaemic heart disease, heart failure, arrhythmias, valvular disease, hypertension with its control and end-organ effects); respiratory disease (asthma — what triggers it, current medications, last hospital admission or ICU stay; COPD — severity, home oxygen use; obstructive sleep apnoea — diagnosed, on CPAP?); diabetes mellitus (type, current control, HbA1c, microvascular complications affecting gastroparesis, autonomic neuropathy); renal disease (eGFR, dialysis); hepatic disease (cirrhosis affects drug metabolism and coagulation); neurological conditions (stroke, seizures — important before spinal anaesthesia or regional blocks near the neuraxis); and previous surgical history (abdominal adhesions affect laparoscopic access; previous cervical spine surgery affects positioning and airway management; previous back surgery affects spinal or epidural placement).
Domain 4: Drug history and allergies. This is the domain most likely to be incomplete and most consequential if it is. Take a systematic drug history: ask specifically about every oral tablet, inhaler, patch, injection, eye drop, and herbal supplement. The patient often does not mention medications they consider 'not important.' Key drugs requiring specific anaesthetic management:
- Antihypertensives: ACE inhibitors and ARBs may be held on the morning of surgery (risk of intraoperative hypotension); beta-blockers must be continued (abrupt withdrawal causes rebound tachycardia and ischaemia)
- Anticoagulants (warfarin, DOACs) and antiplatelets (aspirin, clopidogrel, ticagrelor): require a hold or bridge plan
- Diabetes medications: oral hypoglycaemics withheld morning of surgery; insulin dose adjusted
- MAO inhibitors (phenelzine, tranylcypromine): risk of hypertensive crisis with vasopressors (tyramine reaction) and serotonin syndrome with pethidine — historically held 2 weeks preoperatively
- Steroids: patients on long-term steroids have hypothalamic-pituitary-adrenal suppression and may need supplementary hydrocortisone ('steroid cover') perioperatively
- Lithium: can prolong neuromuscular blockade; continue but check renal function
- Herbal supplements: St John's Wort induces CYP enzymes; garlic, ginkgo, and ginseng affect platelet function
Allergies must be documented with the specific drug, the reaction, and the severity (true anaphylaxis with bronchospasm and cardiovascular collapse versus rash or nausea — these are clinically different and require different management). A latex allergy requires latex-free equipment throughout the procedure.
Domain 5: Systems review. A brief directed systems review confirms the history is complete:
- Cardiovascular: chest pain, dyspnoea (at rest, on exertion — how many flights of stairs?), orthopnoea (number of pillows), paroxysmal nocturnal dyspnoea, palpitations, syncope, ankle swelling
- Respiratory: wheeze, cough (productive?), sputum, nocturnal symptoms, snoring, witnessed apnoea, daytime somnolence
- Gastrointestinal: gastro-oesophageal reflux (increases aspiration risk — patients may need rapid sequence induction), nausea and vomiting history, last oral intake (fasting status)
- Musculoskeletal: cervical spine mobility (affects positioning and airway), jaw mobility, arthritis affecting positioning
- Neurological: neurological deficits, neuropathy (relevant before regional anaesthesia — document baseline function)
Domain 6: Social history. Smoking (pack-years — >20 pack-years increases postoperative pulmonary complication risk; advise cessation, though even 8 weeks before surgery improves outcomes); alcohol (heavy use increases tolerance to sedatives and volatile agents; 2 or more units per day should prompt questioning about dependence and liver function); recreational drugs (cocaine — risk of cardiac arrhythmia under anaesthesia; cannabis — cross-reaction with some anaesthetic pathways).
Domain 7: Functional capacity. Formally assess in METs. 'Can you walk on level ground at a normal pace for 2 blocks without stopping? Can you climb one flight of stairs? Do you do any regular exercise?' Functional capacity less than 4 METs indicates increased perioperative cardiac risk for major surgery.
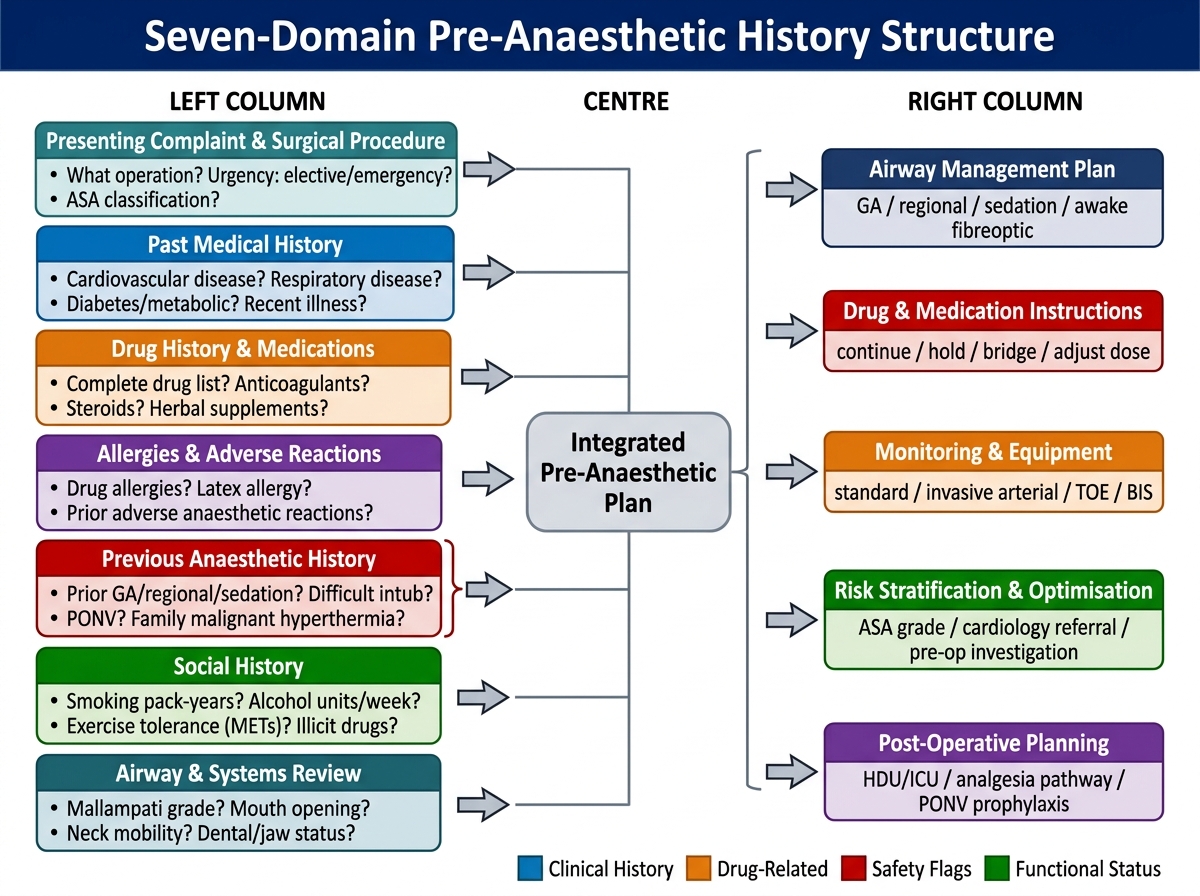
Seven-Domain Pre-Anaesthetic History: Inputs and Downstream Anaesthetic Plan Decisions
Medication Review: A Systematic Approach
The medication review is a critical subspecialty skill within the pre-anaesthetic assessment because the interaction between a patient's existing medications and anaesthetic drugs is a common source of perioperative complications. A systematic medication review goes beyond simply listing drugs — it generates specific perioperative management instructions for every drug on the patient's list.
The systematic approach to medication review has five steps. First, obtain a complete drug list: ask the patient to bring all medications to the assessment; cross-reference with the GP letter, discharge summary, and electronic records; check for over-the-counter drugs and herbal supplements (patients often omit these). Second, classify each drug by perioperative action: continue, hold, adjust dose, or bridge. Third, identify drugs with direct anaesthetic interactions: specific drug classes that alter anaesthetic management are listed below. Fourth, write explicit medication instructions for the night before and the morning of surgery. Fifth, document the medication review in the anaesthetic pre-assessment record, including any drugs held and the plan for resumption.
The following framework covers the most clinically significant drug categories:
| Drug class | Examples | Perioperative action | Reason |
|---|---|---|---|
| Beta-blockers | Metoprolol, atenolol, carvedilol | Continue | Abrupt withdrawal causes rebound tachycardia and ischaemia |
| ACE inhibitors / ARBs | Enalapril, losartan | Debated — many centres hold day of surgery | Perioperative refractory hypotension from blunted renin-angiotensin response |
| Statins | Atorvastatin, rosuvastatin | Continue | Withdrawal increases perioperative cardiac events |
| Warfarin | Warfarin | Hold 3-5 days; bridge with LMWH if high VTE risk | INR must approach normal for most surgery |
| DOACs | Apixaban, rivaroxaban | Hold 24-48 h; dabigatran 48-96 h (renally adjusted) | Direct thrombin or Xa inhibition cannot be reversed without specific antidotes |
| Aspirin | Aspirin 75-150 mg | Continue for low-bleeding-risk surgery; hold 7 days for high-bleeding-risk | Risk of perioperative MI vs bleeding |
| P2Y12 inhibitors | Clopidogrel, ticagrelor | Hold 5-7 days | Platelet function does not recover faster |
| Oral hypoglycaemics | Metformin, glipizide | Hold morning of surgery; metformin held 24-48 h if renal risk | Hypoglycaemia risk; metformin lactic acidosis if perioperative renal impairment |
| Insulin | All types | Continue long-acting at 50-80% dose; hold rapid-acting without food | Hypoglycaemia risk |
| MAO inhibitors | Phenelzine, tranylcypromine | Traditionally hold 2 weeks; consult psychiatrist | Risk of hypertensive crisis (sympathomimetics) and serotonin syndrome (pethidine) |
| Steroids (long-term) | Prednisolone ≥5 mg/day >3 weeks | Continue; add steroid cover (hydrocortisone 50-100 mg IV at induction) | HPA axis suppression; risk of adrenal crisis |
| Thyroid medications | Levothyroxine, carbimazole | Continue | Thyroid status must be stable perioperatively |
Document the final instruction for every drug in a format the ward nurses can act on: for example, 'Metoprolol 50 mg — TAKE as usual on morning of surgery with a small sip of water. Enalapril 10 mg — OMIT on morning of surgery; resume with the first oral intake postoperatively. Metformin 500 mg — OMIT from midnight before surgery; resume 48 h after surgery if renal function is normal.'
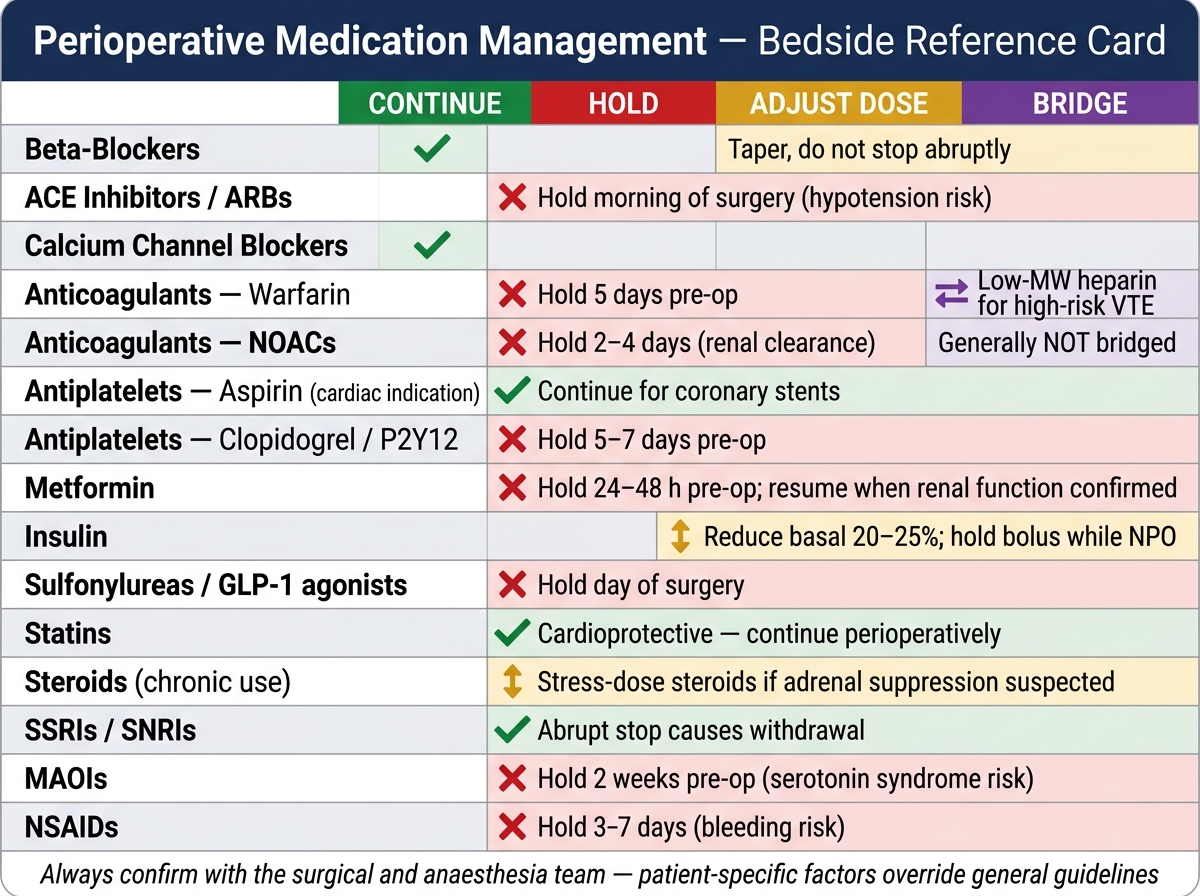
Perioperative Medication Management — Bedside Reference Card