Page 5 of 15
AS3.2-3 | Pre-anaesthetic History, Medication Review and Clinical Examination Documentation — SDL Guide (Part 2)
Clinical Examination: Airway, Cardiovascular, Respiratory, and Documentation
The clinical examination component of the pre-anaesthetic assessment is focused and targeted — it is not a full systems examination but a problem-oriented assessment shaped by the history findings. Unlike the history, which relies on the patient's recall and self-report, the clinical examination provides objective data that the anaesthesiologist can measure, record, and act upon immediately. This combination of subjective history and objective examination is what makes the pre-anaesthetic assessment far more reliable than either element alone. Three areas are mandatory regardless of the history findings: the airway assessment, the cardiovascular examination, and the respiratory examination. Additional systems examination is directed by specific history findings — for example, a neurological examination is indicated before spinal or epidural anaesthesia in a patient with pre-existing neurological deficits, and an abdominal examination is essential when ascites or organomegaly may affect laparoscopic surgery or prone positioning. The airway assessment is discussed first because it is unique to anaesthesia and its findings determine the entire airway management strategy for the procedure. A documented, systematic difficult airway prediction prevents the most catastrophic scenario in anaesthetic practice: an unanticipated difficult intubation in an anaesthetised, apnoeic patient with no plan for alternative airway management.
The airway assessment is unique to anaesthesia and its findings determine the entire airway management strategy. A documented difficult airway prediction prevents the catastrophic scenario of an unexpected difficult intubation in an anaesthetised, apnoeic patient. The airway assessment components:
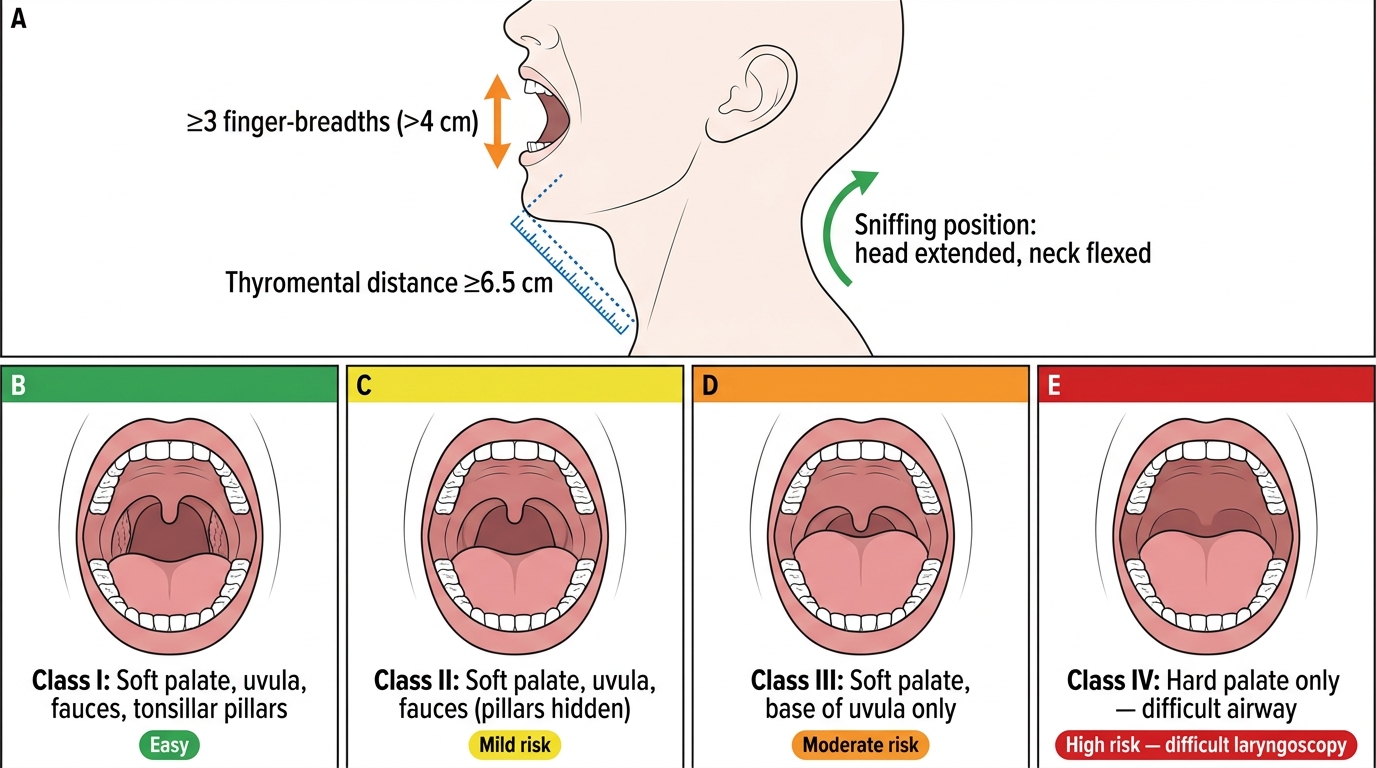
- Mouth opening (inter-incisor distance): ≥3 finger breadths (~4-5 cm) is adequate. Below 3 cm predicts difficulty with direct laryngoscopy.
- Mallampati class (Class I-IV): assessed with patient sitting, mouth maximally open, tongue protruded, without phonation. Class I — uvula, fauces, and tonsillar pillars fully visible; Class II — uvula and fauces visible, pillars hidden; Class III — only base of uvula visible; Class IV — hard palate only. Class III-IV predicts difficulty with laryngoscopy.
- Thyromental distance: measured from the thyroid notch to the chin with head fully extended. ≥6.5 cm is favourable; <6 cm predicts difficulty.
- Neck mobility: can the patient assume the 'sniffing position' (neck flexed, head extended on atlanto-occipital joint)? Limited neck extension (cervical spondylosis, halo brace, rheumatoid arthritis affecting the atlanto-axial joint) significantly impairs laryngoscopy.
- Facial features: beard (reduces mask seal), receding chin (micrognathia — predicts difficult laryngoscopy), protruding incisors (bucktooth — impairs laryngoscope handle insertion), high arched palate (Class III/IV Mallampati more likely), body habitus (obesity — short fat neck, excess pharyngeal tissue).
- Teeth: loose or capped teeth may be dislodged or fractured during laryngoscopy; missing teeth affect mask seal. Document precisely and include in consent.
The LEMON mnemonic aids systematic airway assessment: Look externally (beard, obesity, short neck, facial abnormalities); Evaluate the 3-3-2 rule (mouth opening 3 fingers, hyoid-chin 3 fingers, thyromental 2 fingers); Mallampati class; Obstruction (stridor, foreign body, tumour, haematoma); Neck mobility.
The cardiovascular examination relevant to anaesthesia focuses on: pulse rate and rhythm (arrhythmia must be characterised and, if new, investigated before elective surgery); blood pressure in both arms (significant difference >10-15 mmHg between arms suggests subclavian stenosis or aortic pathology — relevant for arterial line placement and BP monitoring site); JVP (elevated JVP in CCF affects fluid management and head positioning); apex beat (displaced apex suggests cardiomegaly); heart sounds (a new murmur must be characterised — systolic murmur in aortic stenosis is a high-risk finding and warrants echocardiography before major elective surgery; aortic stenosis is poorly tolerated under general anaesthesia because the fixed outflow obstruction cannot compensate for the vasodilation caused by induction agents); and peripheral perfusion (central and peripheral cyanosis, capillary refill time, pedal oedema).
The respiratory examination assesses: respiratory rate and oxygen saturation on room air (baseline SpO2 below 94% without a known cause requires investigation); chest expansion symmetry; percussion (dullness may indicate pleural effusion, which affects respiratory mechanics during anaesthesia, particularly in laparoscopic procedures where the Trendelenburg position further compromises ventilation); auscultation (wheeze — current bronchospasm requires treatment before elective surgery; crepitations — bilateral basal crepitations in a patient with CCF indicate pulmonary oedema, which dramatically increases anaesthetic risk).
Documentation of the clinical examination must be specific and clinically actionable. Vague documentation ('chest clear, heart sounds normal') is inadequate. The anaesthetic note should state, for example: 'Airway: mouth opening 3 finger-breadths, Mallampati Class II, thyromental distance 6.5 cm, neck mobility full, no predictors of difficult intubation — plan for routine RSI. CVS: BP 148/92 mmHg right arm, pulse 76/min regular, no murmurs, JVP not elevated, no ankle oedema. RS: SpO2 98% on air, RR 16/min, air entry equal bilaterally, no added sounds.'
Airway Assessment: Clinical Measurements and Mallampati Classification
SELF-CHECK
During a pre-anaesthetic assessment, a patient is asked to open his mouth maximally and protrude his tongue. You can see only the hard palate — the soft palate and uvula are completely hidden. What is his Mallampati class and what does this predict?
A. A. Mallampati Class II — mild difficulty expected with laryngoscopy
B. B. Mallampati Class III — soft palate visible but uvula hidden
C. C. Mallampati Class IV — only hard palate visible, predicts difficult laryngoscopy
D. D. Mallampati Class I — full oropharyngeal exposure, easy airway
Reveal Answer
Answer: C. C. Mallampati Class IV — only hard palate visible, predicts difficult laryngoscopy
When only the hard palate is visible with maximal mouth opening and tongue protrusion (no soft palate visible), this is Mallampati Class IV. Class IV is the highest grade and predicts significant difficulty with direct laryngoscopy. Class I shows full exposure (uvula, fauces, tonsillar pillars). Class II shows uvula and fauces but not the pillars. Class III shows only the soft palate and base of uvula. Mallampati IV combined with other unfavourable features (thyromental distance less than 6.5 cm, limited neck mobility, mouth opening less than 3 finger-breadths) should trigger a plan for awake fibreoptic intubation or alternative airway management technique.
Monitoring During and Interpretation After the Assessment
The pre-anaesthetic assessment produces both a clinical record and a monitoring prescription — a decision about what level of intraoperative and postoperative monitoring the patient's risk profile requires. This section addresses how assessment findings translate into monitoring decisions and how to interpret abnormal findings.
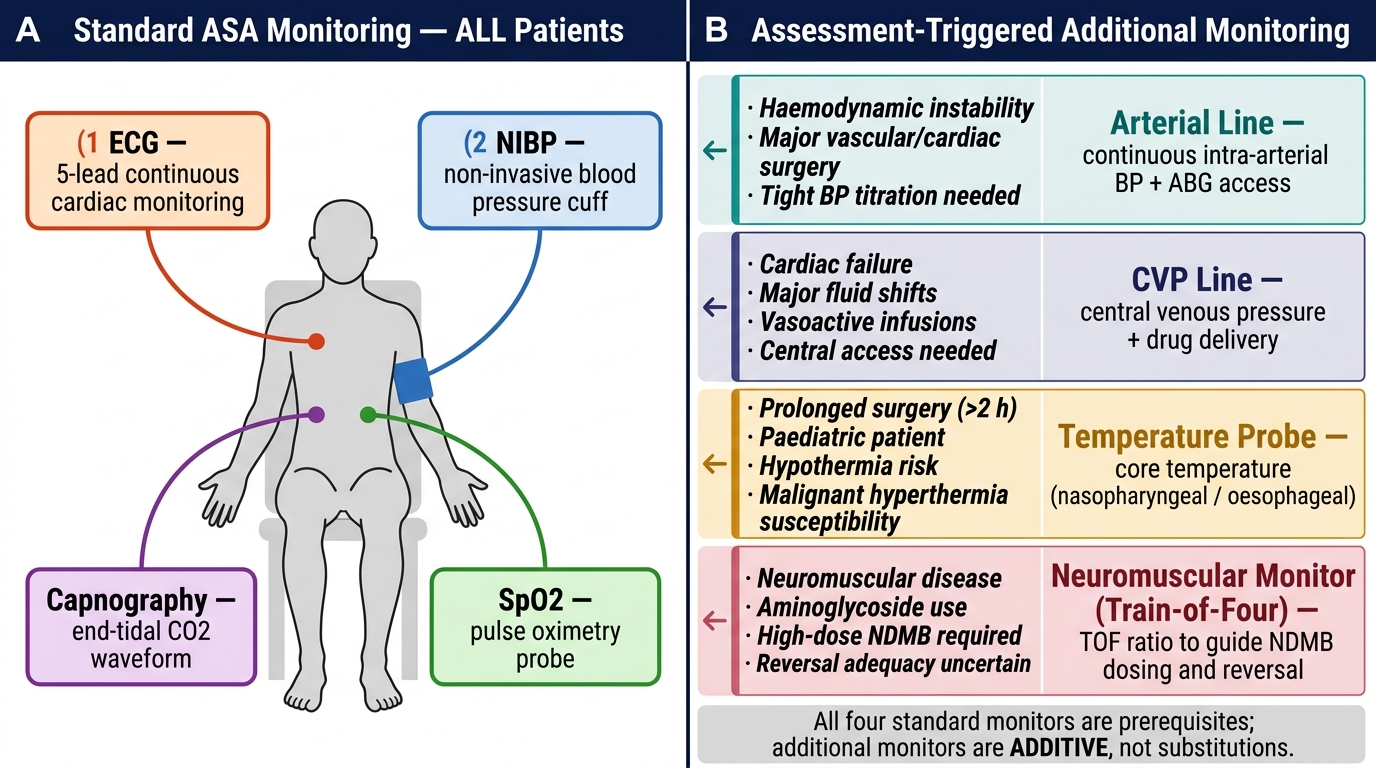
Standard monitoring for every patient under anaesthesia includes the basic anaesthetic monitor triad: non-invasive blood pressure (NIBP) measured at least every 5 minutes, continuous ECG (lead II for rhythm + lead V5 for ischaemia), and pulse oximetry (SpO2). These are non-negotiable for any patient receiving any form of anaesthesia. Additional monitoring is layered on the basis of the pre-anaesthetic assessment findings.
Capnography (end-tidal CO2, EtCO2): mandatory for all intubated patients; confirms tracheal intubation (immediate rise in EtCO2 after intubation) and provides a breath-by-breath reflection of ventilation adequacy and cardiac output. In the pre-anaesthetic assessment, identifying any condition that affects CO2 elimination — severe COPD, pulmonary embolism, low cardiac output — allows the anaesthesiologist to set appropriate EtCO2 targets (in COPD, a slightly elevated EtCO2 may reflect the patient's chronic baseline rather than hypoventilation).
Invasive arterial pressure monitoring (arterial line): indicated in haemodynamically unstable patients, major vascular or cardiac surgery, anticipated significant intraoperative blood pressure fluctuations, or when frequent blood sampling is needed. The assessment identifies patients likely to need this level of monitoring: those with severe hypertension, significant cardiac disease, morbid obesity with limited NIBP accuracy, or shock physiology.
Central venous pressure (CVP) monitoring: indicated for large-volume fluid management, vasopressor infusion (when peripheral access is unsuitable), or total parenteral nutrition. CVP does not reliably predict fluid responsiveness alone (integrated with dynamic measures), but is useful for trend monitoring.
Neuromuscular blockade monitoring (peripheral nerve stimulator, train-of-four): indicated when neuromuscular blocking agents are used; particularly important in patients with myasthenia gravis, myopathies, or renal failure (where drug clearance is prolonged). The pre-anaesthetic assessment identifies these patients and prompts planning for reversal of neuromuscular blockade and postoperative respiratory monitoring.
Temperature monitoring: important in prolonged procedures, paediatric patients, and any procedure with high heat loss risk (open abdominal or thoracic surgery). Identifying hypothermia risk preoperatively allows planning for active warming devices.
Abnormal pre-anaesthetic findings and their interpretation:
- Baseline SpO2 92-94%: suggests chronic respiratory compromise (severe COPD, ILD, pulmonary hypertension) — do not target 100% SpO2 in COPD patients (abolishes hypoxic drive); set SpO2 target 88-92%
- Irregular pulse: if new, characterise by ECG before elective surgery; atrial fibrillation with rapid ventricular response should be rate-controlled before anaesthesia
- New murmur: refer for echocardiography before elective surgery; severe aortic stenosis (valve area <1 cm2 or mean gradient >40 mmHg) significantly increases anaesthetic risk
- Resting BP >180/110 mmHg: consider deferring elective surgery until better controlled; however, acutely lowering BP immediately before surgery can be dangerous — gradual optimisation is preferred
ASA Standard Monitoring and Assessment-Triggered Additional Monitoring
Applied Practice and Documentation Standards
The pre-anaesthetic assessment is only as valuable as its documentation. An assessment that is performed but not recorded might as well not have happened: it does not guide the operating team, it does not protect the anaesthesiologist medicolegally, and it cannot inform the postoperative care plan.
Provided image
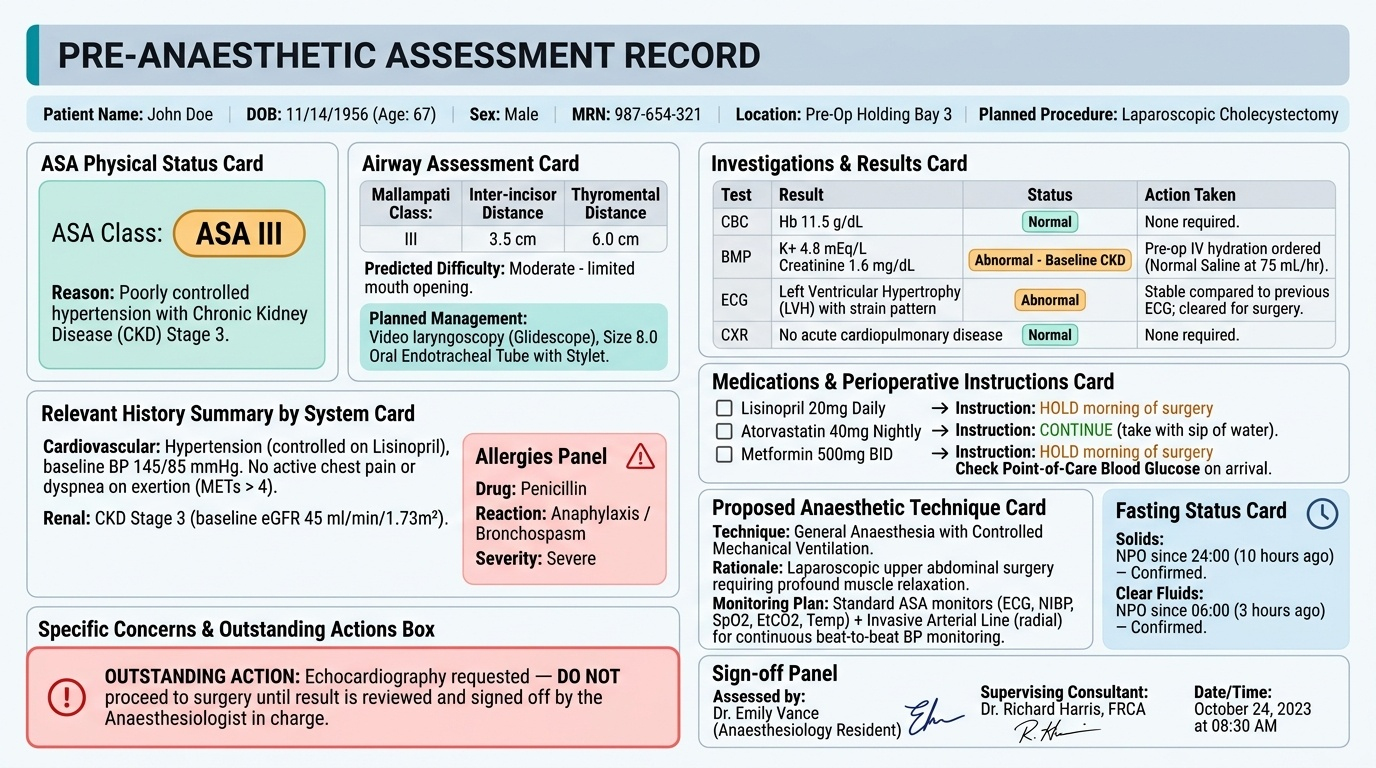
A complete pre-anaesthetic assessment record contains the following elements, in order: patient identification and planned procedure; ASA Physical Status classification with the reason (e.g. 'ASA III — poorly controlled hypertension with CKD stage 3'); airway assessment findings with the predicted airway difficulty and the planned airway management technique; relevant history summary by system; medication list with perioperative instructions for each drug; relevant investigation results (blood results, ECG interpretation, CXR findings) with normal/abnormal designation and the action taken; the proposed anaesthetic technique with rationale; the monitoring plan; the fasting instruction confirmed; and any specific concerns or outstanding actions (e.g. 'echocardiography requested — do not proceed to surgery until result reviewed by anaesthesiologist in charge').
For supervised practice in the medical student or intern setting, the recommended approach is to perform the assessment independently first, then present findings to the supervising anaesthesiologist. Common documentation errors to avoid:
1. Vague airway description — 'airway normal' tells the operating team nothing; document Mallampati class, inter-incisor distance, and thyromental distance specifically
2. Incomplete allergy documentation — document the drug, the reaction, and the severity; 'no known drug allergies' is a positive finding that should be stated, not an absence of documentation
3. Generic medication instructions — 'continue usual medications' is insufficient; list each drug with its specific instruction
4. Missing anaesthetic history — failure to ask about previous difficult airway or family history of malignant hyperthermia has caused patient deaths; this question must be asked and documented
5. Undated, unsigned, or incomplete notes — medicolegally, an unsigned note does not establish authorship; an undated note cannot establish the timeline of clinical decisions
The pre-anaesthetic assessment concludes with a conversation with the patient that covers: the planned anaesthetic technique in plain language; the specific risks relevant to this patient (e.g. difficult intubation — tell the patient honestly and plan accordingly; risk of postoperative nausea — discuss prophylactic antiemetics); the fasting and medication instructions for the day of surgery; and what to expect in the anaesthetic room and recovery area.
IMPORTANT: When a difficult airway is identified during the pre-anaesthetic assessment of a previously anaesthetised patient, always try to obtain the notes from the previous anaesthetic — these will document what laryngoscopy grade was seen, what technique was used, and what worked. If a 'difficult airway alert' sticker or card was given to the patient, check for it. Forewarned is forearmed.