Page 5 of 17
AS5.{3,6} | Peripheral Nerve Blocks and Common Surgical Blocks — SDL Guide
CLINICAL SCENARIO
A 35-year-old motorcyclist arrives in the emergency department with a comminuted fracture-dislocation of the right wrist. He is haemodynamically stable, fasting for four hours, and anxious. The hand surgeon wants to take him to theatre immediately. An axillary brachial plexus block is performed in 12 minutes: the patient is comfortable, the surgeon operates in a bloodless field with tourniquet, and the patient is eating an hour after closure. No airway was instrumented, no opioids were given systemically, and he is alert enough to follow post-operative instructions. Peripheral nerve blocks are not a niche skill reserved for subspecialists — they are a core competency that transforms acute surgical care. This SDL covers the principles, anatomy, and techniques of peripheral nerve blocks and common surgical blocks (AS5.3, AS5.6).
WHY THIS MATTERS
Peripheral nerve blocks (PNBs) are increasingly the default anaesthetic strategy for limb surgery, trauma care, and postoperative pain management in high-volume surgical centres worldwide. For the Indian medical graduate observing in theatre, understanding what each block targets, what anatomy governs its placement, and what complications to watch for transforms passive observation into meaningful clinical learning. These skills also underpin safe postoperative analgesia — a patient with a femoral nerve catheter after knee replacement needs a nurse and junior doctor who understand what a numb leg means and what it does not.
RECALL
Review the following before proceeding:
- Brachial plexus organisation: Roots (C5–T1) → Trunks (upper/middle/lower) → Divisions → Cords (lateral/posterior/medial) → Terminal branches (musculocutaneous, median, radial, ulnar, axillary).
- Lower limb innervation: femoral nerve (L2–L4, anterior thigh and knee), sciatic nerve (L4–S3, posterior thigh, leg below knee), obturator nerve (L2–L4, medial thigh).
- Local anaesthetic pharmacology: maximum doses — lignocaine 3 mg/kg plain / 7 mg/kg with adrenaline; bupivacaine 2 mg/kg — and LAST management with 20% intralipid.
- Ultrasound fundamentals: echogenicity of nerves (hyperechoic fascicular appearance), surrounding vessels, and tissue planes.
Clinical Indication and Relevance of Peripheral Nerve Blocks
Peripheral nerve blocks achieve surgical anaesthesia or postoperative analgesia by depositing local anaesthetic solution adjacent to a peripheral nerve or nerve plexus at a point remote from the surgical site. Unlike neuraxial blocks, PNBs are anatomically targeted — only the nerve(s) supplying the operative region are blocked, preserving haemodynamic stability and leaving bladder and bowel function intact.
The principal indications for PNBs in surgery can be grouped as follows. As the sole anaesthetic, PNBs are excellent for forearm and hand surgery (axillary or infraclavicular block), shoulder surgery (interscalene block), lower-leg and foot surgery (sciatic ± femoral block), and inguinal hernia repair (ilioinguinal/iliohypogastric block with or without TAP block). As an adjunct to general anaesthesia, PNBs reduce intraoperative opioid requirements, blunt the haemodynamic stress response, and provide superior postoperative analgesia — enabling earlier mobilisation and discharge. For trauma, a femoral nerve block or fascia iliaca block provides immediate pain relief for hip fracture while the patient awaits definitive surgery.
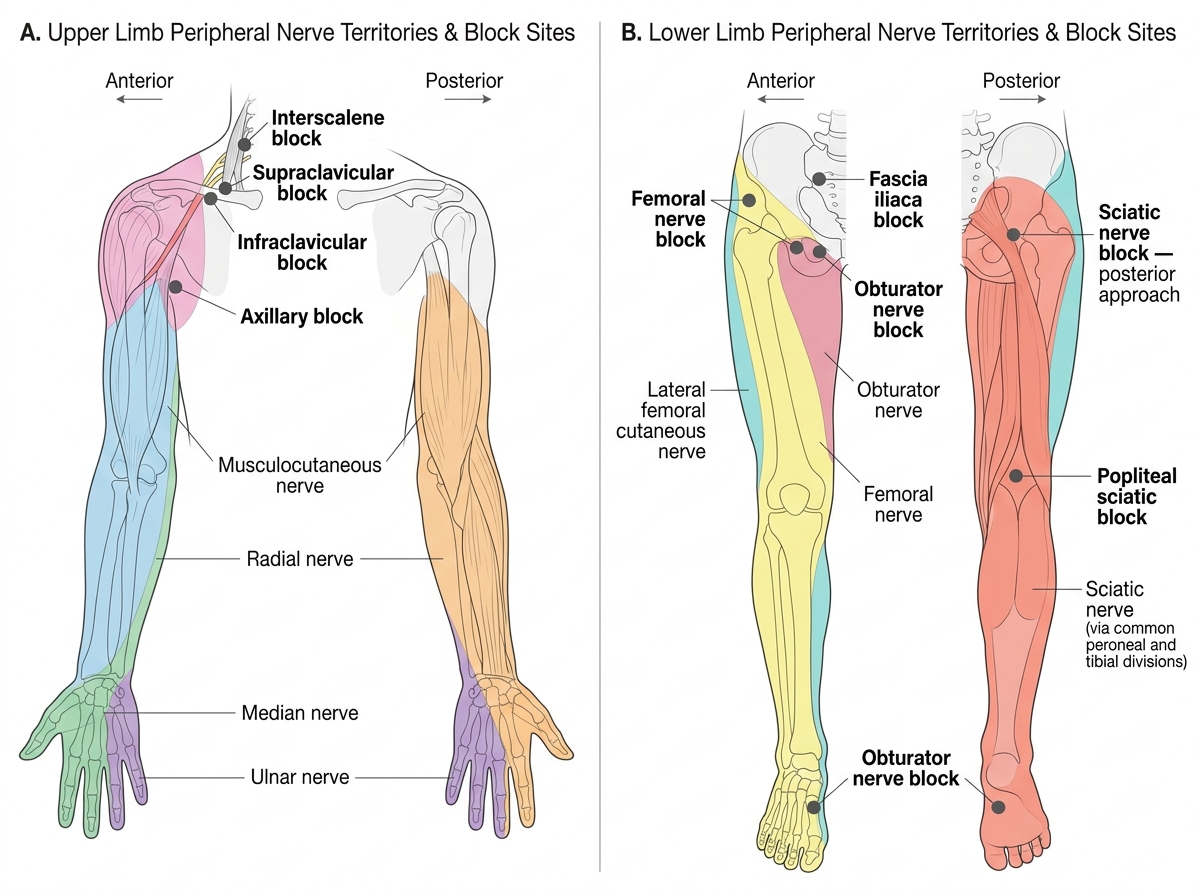
Cutaneous Territories of Major Peripheral Nerves and Block Approach Sites: Upper and Lower Limb
PNBs are particularly advantageous in patients with respiratory compromise (no risk of high neuraxial block causing respiratory muscle paralysis), those on anticoagulants where neuraxial block is contraindicated (compressible sites can be directly observed for haematoma), and those with latex allergy or malignant hyperthermia susceptibility (avoids triggering agents entirely). The decision to use a PNB rather than neuraxial block or GA requires assessment of the nerve coverage needed, patient anatomy, operator experience, and the availability of ultrasound guidance.
Anatomy Governing Peripheral Nerve Block Placement
Safe and effective PNB placement requires a working knowledge of the relevant anatomy at each block site — not just the nerve itself, but the surrounding structures that must be avoided and the tissue planes that guide needle approach.
Brachial plexus approaches exploit the anatomical continuity of the plexus sheath. At the interscalene level (between the anterior and middle scalene muscles), the C5, C6, and C7 roots are superficial and accessible but in close proximity to the phrenic nerve (C3–C5) running on the anterior surface of the anterior scalene — phrenic nerve block is essentially universal (100%) with interscalene block, causing ipsilateral hemidiaphragm paralysis. The internal jugular vein, carotid artery, and vertebral artery are nearby. At the supraclavicular level, the trunks/divisions converge compactly just posterolateral to the subclavian artery as it crosses over the first rib — producing compact, reliable "spinal of the arm" coverage, but with risk of pneumothorax (the lung apex is immediately below). At the axillary level, the terminal nerves (median, radial, ulnar, musculocutaneous) surround the axillary artery in a neurovascular bundle — the musculocutaneous nerve often exits the sheath proximally to enter coracobrachialis, requiring separate injection.
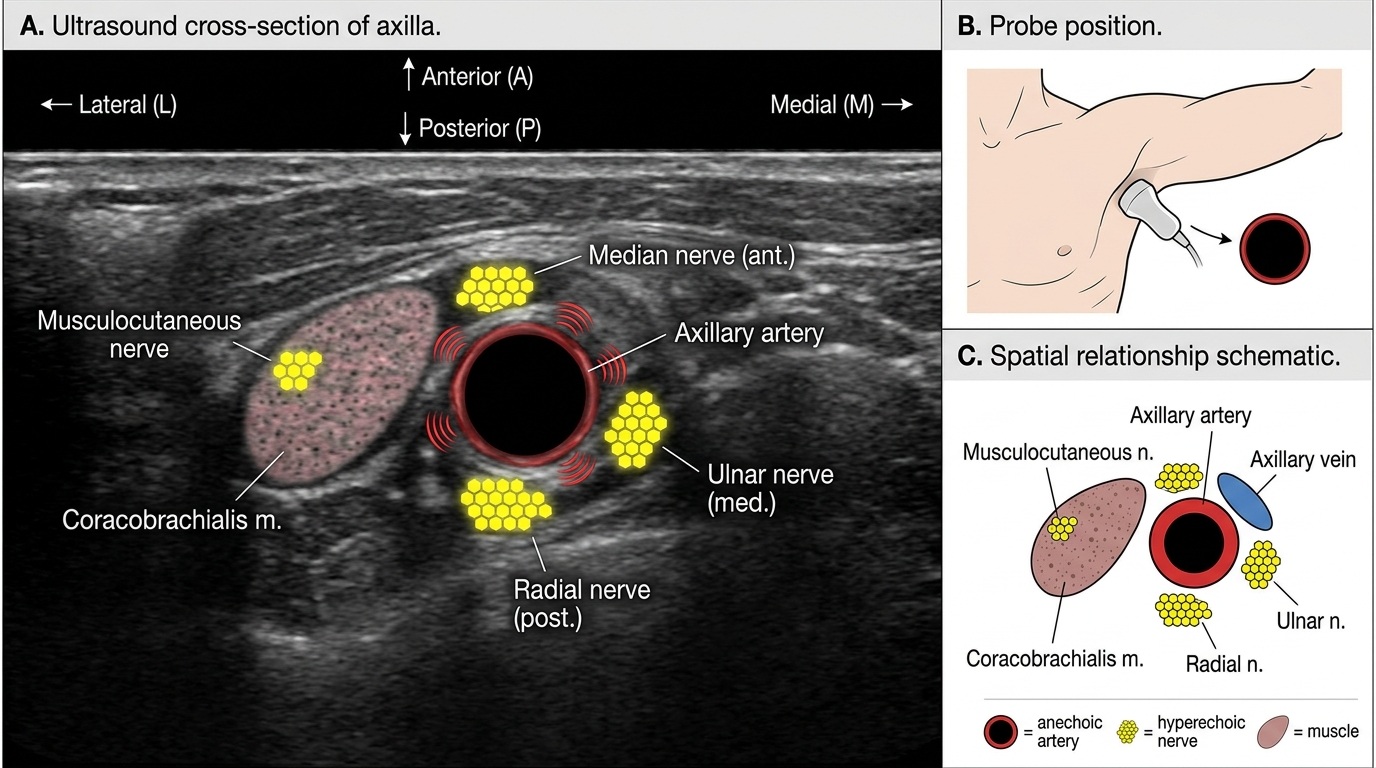
Axillary Ultrasound Anatomy for Brachial Plexus Block
Lower limb anatomy for common blocks: The femoral nerve (L2–L4) emerges from beneath the inguinal ligament lateral to the femoral artery (mnemonic: NAVEL from lateral to medial — Nerve, Artery, Vein, Empty space, Lymphatics). It divides almost immediately below the ligament into its terminal branches, so blocks must be placed at or just below the inguinal ligament to be effective. The sciatic nerve (L4–S3, the largest peripheral nerve in the body) exits the pelvis through the greater sciatic foramen below piriformis, passes between the greater trochanter and ischial tuberosity, and descends in the posterior thigh. It can be blocked at the subgluteal level (posterior approach) or in the popliteal fossa where it divides into the tibial nerve (medial, plantar flexion) and common peroneal nerve (lateral, dorsiflexion and eversion). The popliteal approach is particularly useful for foot and ankle surgery when combined with a saphenous nerve block.
Techniques: Brachial Plexus Blocks
The technique of a peripheral nerve block has evolved dramatically with the introduction of ultrasound guidance (USG), which has largely replaced nerve stimulator guidance as the standard of care in equipped centres. USG allows real-time visualisation of the nerve, needle, and surrounding structures, reducing the risk of intravascular injection, pneumothorax, and nerve injury while improving block success rates. In the era before ultrasound, anaesthetists relied on anatomical landmarks plus a nerve stimulator — a device that delivers a small current through the needle tip to elicit a motor twitch at the lowest possible current (0.2–0.3 mA indicates close proximity; 0.5 mA is the clinical threshold). While nerve stimulators remain useful in environments without ultrasound or when imaging is obscured by bowel gas or oedema, ultrasound is now the default in any well-equipped setting. Regardless of which guidance method is used, the procedural principles of patient safety, strict asepsis, dose-limiting, and real-time aspiration remain non-negotiable and are laid out in the following sequence.
General steps applicable to all PNBs:
1. Patient preparation — IV access, monitors (NIBP, SpO2, ECG), resuscitation equipment and drugs (including 20% intralipid) available.
2. Positioning — optimised for both patient comfort and probe/needle access.
3. Skin preparation — antiseptic, sterile drape.
4. Ultrasound probe selection — high-frequency linear probe (10–15 MHz) for superficial nerves; lower frequency for deep structures.
5. Needle — typically a short-bevel, echogenic block needle (e.g., 22G × 50–100 mm).
6. In-plane vs out-of-plane — in-plane (needle visualised along its entire length) is preferred for most blocks.
7. Aspiration before every injection to exclude intravascular placement.
8. Injection — slow, incremental, with frequent aspiration; observe spread of LA around the nerve under ultrasound ("doughnut sign" or circumferential spread is ideal).
9. Post-block monitoring — check block onset (temperature difference, pinprick, motor power at 10–15 minutes).
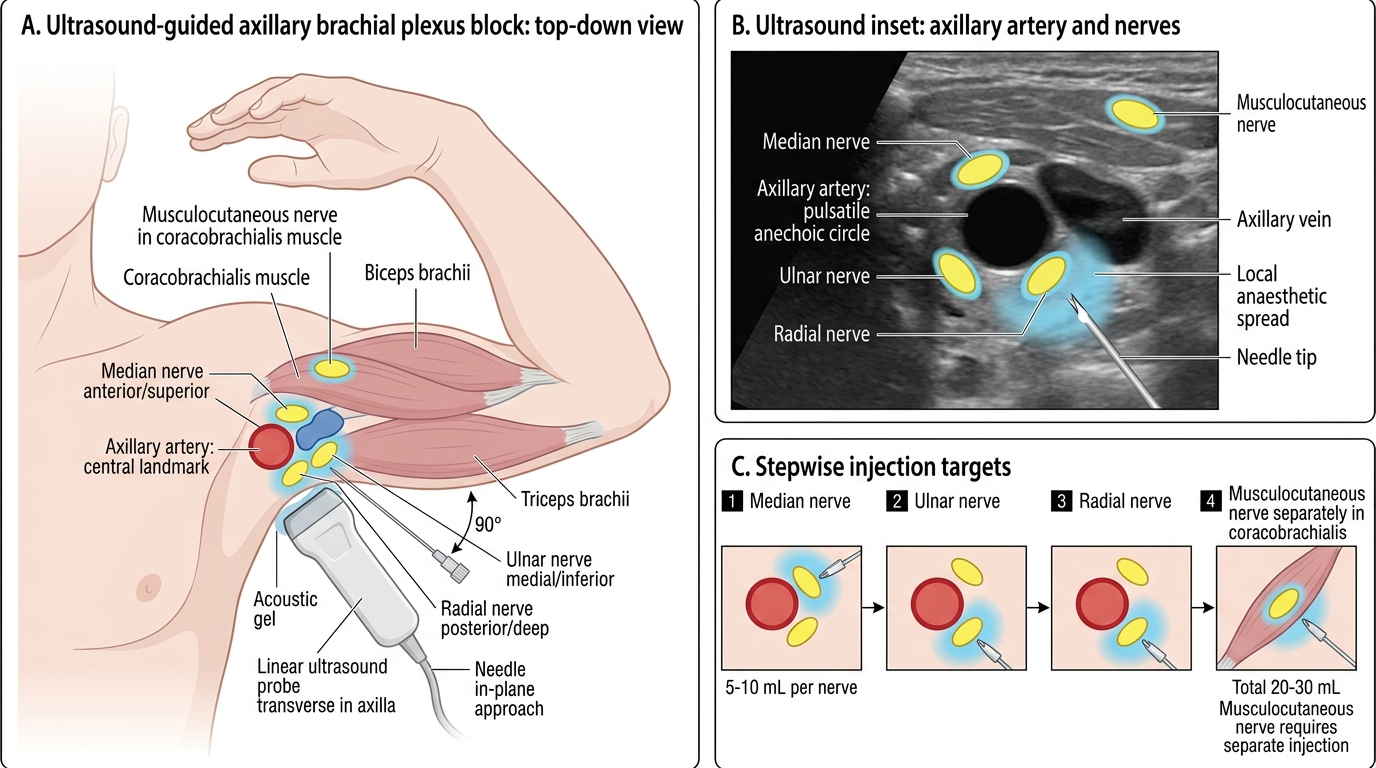
Ultrasound-Guided Axillary Brachial Plexus Block
Axillary block technique: Patient supine, arm abducted 90°, elbow flexed. Probe placed transversely in the axilla. The axillary artery is the central landmark — identified as a round, pulsatile, anechoic (black) structure. The median nerve lies anterior/superior, ulnar nerve medial/inferior, radial nerve posterior (deep to artery). The musculocutaneous nerve is found separately within or adjacent to the coracobrachialis muscle belly. LA is deposited around each nerve — typically 5–10 mL per nerve, total 20–30 mL of 0.5% bupivacaine or 1.5–2% lignocaine depending on duration required.
Supraclavicular block technique: Patient supine, head turned away. Probe placed in the supraclavicular fossa. The subclavian artery is identified pulsating on the first rib — the brachial plexus appears as a "cluster of grapes" superolateral to the artery. Needle inserted in-plane from lateral to medial. LA deposited within the cluster — 20–30 mL. Onset: 10–15 minutes, duration 8–12 hours with bupivacaine. Key risk: pneumothorax (always check for lung sliding on ultrasound after injection in training settings).
SELF-CHECK
During an axillary brachial plexus block, the musculocutaneous nerve must be blocked separately. Why does it require a separate injection?
A. It is too small to be seen on ultrasound and must be blocked by landmark technique
B. It leaves the brachial plexus sheath proximally to enter the coracobrachialis muscle, so a single sheath injection may not reach it
C. It arises directly from the cervical plexus and is not part of the brachial plexus sheath
D. It is blocked by diffusion from the axillary artery sheath and requires no separate injection
Reveal Answer
Answer: B. It leaves the brachial plexus sheath proximally to enter the coracobrachialis muscle, so a single sheath injection may not reach it
The musculocutaneous nerve (C5–C7) is a terminal branch of the lateral cord that exits the brachial plexus sheath proximal to the axilla to enter the coracobrachialis muscle, where it travels distally to supply the lateral forearm (lateral cutaneous nerve of forearm). Because it lies outside the axillary neurovascular sheath at the level of the axillary block, a single sheath injection does not reliably anaesthetise its territory. A separate injection into the substance of coracobrachialis under ultrasound guidance is required if forearm coverage is needed.