Page 6 of 17
AS5.{3,6} | Peripheral Nerve Blocks and Common Surgical Blocks — SDL Guide (Part 2)
Techniques: Common Surgical Blocks
Several peripheral nerve blocks have become so commonly used for specific surgical procedures that they are considered the standard of care at high-volume centres. These are the "work-horse" blocks that every anaesthesia trainee must understand by observation and description.
Femoral nerve block (FNB): Performed below the inguinal ligament with the patient supine. Probe placed transversely in the femoral crease — the femoral artery is the landmark, with the femoral nerve lying lateral to it, appearing as a hyperechoic triangular structure beneath the fascia iliaca. LA (15–20 mL of 0.5% bupivacaine) deposited below the fascia iliaca, lateral to the artery. Provides anaesthesia to the anterior thigh and knee. Commonly used for knee arthroplasty, femoral shaft fractures, and quadriceps tendon repair. Limitation: does not cover the posterior knee (sciatic territory) or the medial leg.
Fascia iliaca block: A volume-dependent block using the fascia iliaca compartment to bathe the femoral nerve and, with large enough volumes, the lateral femoral cutaneous and obturator nerves. A "2-pop" landmark technique (penetrating the fascia lata then the fascia iliaca) or an ultrasound-guided approach may be used. This block is widely employed for hip fracture analgesia in the emergency setting because it is teachable to emergency physicians and provides immediate relief with reduced opioid requirements in elderly, frail patients.
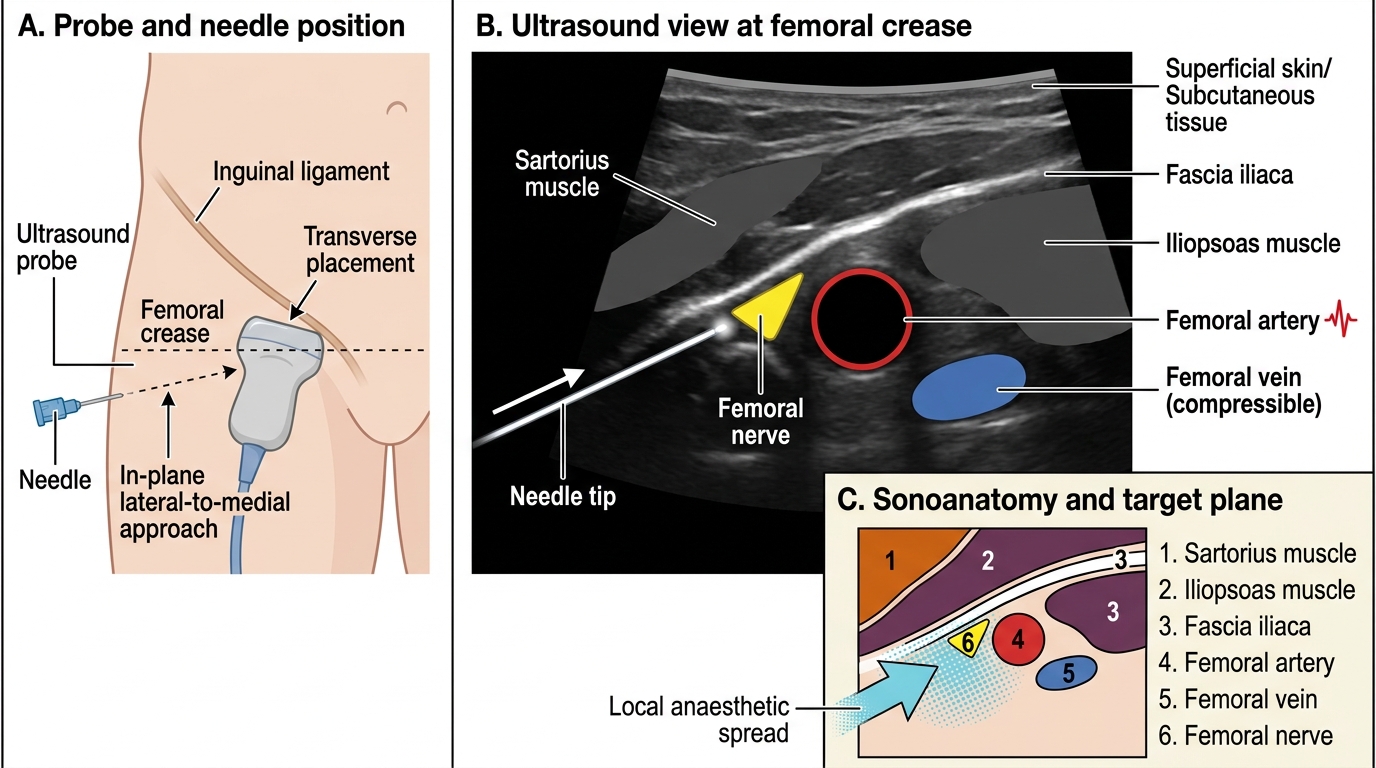
Ultrasound-Guided Femoral Nerve Block at the Femoral Crease
Sciatic nerve block — popliteal approach: Patient supine with knee slightly flexed or in lateral position. Probe placed transversely in the popliteal fossa. The sciatic nerve is identified as a large hyperechoic structure, dividing 4–7 cm above the popliteal crease into the tibial nerve (medial) and common peroneal nerve (lateral). LA deposited proximal to the bifurcation (20–30 mL of 0.5% bupivacaine) to achieve complete block. Covers the leg below knee except the medial strip (saphenous nerve, femoral territory). Combined with a saphenous nerve block, provides complete foot/ankle anaesthesia.
Interscalene block: Targets the C5/C6/C7 roots between the scalene muscles. Essential for shoulder surgery (provides complete shoulder anaesthesia). LA 15–20 mL. Universal ipsilateral phrenic nerve block is an unavoidable consequence — contraindicated if contralateral phrenic nerve is paralysed or if the patient cannot tolerate 20–25% reduction in respiratory capacity (severe COPD, contralateral phrenic palsy).
TAP (Transversus Abdominis Plane) block: LA deposited in the plane between the internal oblique and transversus abdominis muscles, blocking the anterior branches of T10–L1. Used as adjunctive analgesia for lower abdominal surgery (caesarean section, appendicectomy, hernia repair). Does not provide visceral analgesia — only covers the anterior abdominal wall.
Monitoring and Interpretation After Block Placement
The work of a peripheral nerve block does not end when the needle is withdrawn. Systematic post-block monitoring serves two purposes: confirming that the block is working before surgery begins, and detecting early complications before they become irreversible.
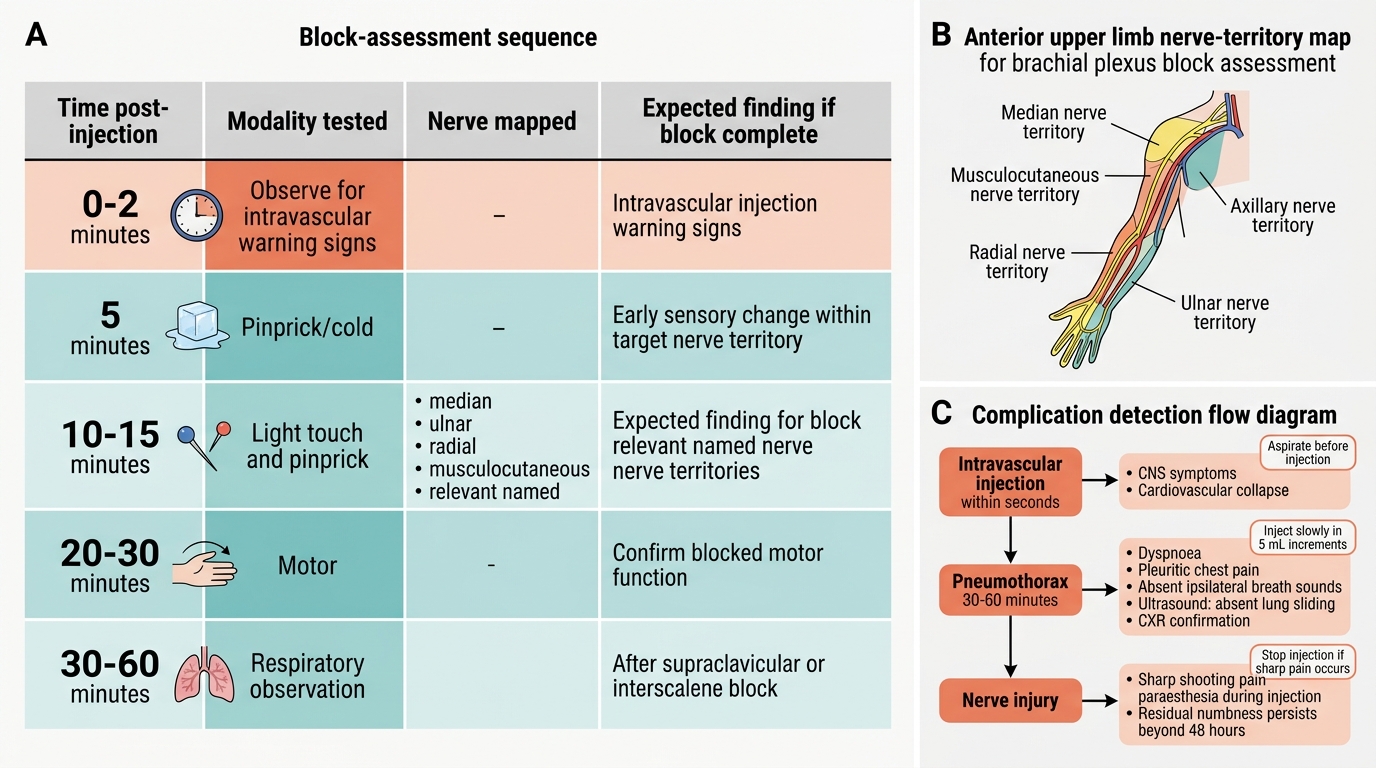
Block onset assessment should begin at 10 minutes after injection. A standard sequence: (1) Temperature discrimination — compare warmth of the blocked limb (vasodilated from sympathetic block) versus the unblocked limb; this is the earliest and most sensitive sign. (2) Pinprick test — use a blunt needle; ask if the sensation feels sharp or blunt compared to the contralateral limb. (3) Motor power — ask for specific movements mapping to the nerves blocked (e.g., wrist extension = radial nerve, thumb opposition = median nerve, finger abduction/adduction = ulnar nerve for an upper limb block). A fully effective block produces warmth, absent pinprick sensation, and motor weakness within 15–20 minutes. An incomplete block at 20–25 minutes should prompt reassessment: was the correct nerve targeted? Is the volume adequate? Is a supplementary block or conversion to GA indicated?
Regional Anaesthesia Block Assessment Sequence
Detecting early complications:
- Intravascular injection — presents within seconds with CNS symptoms (tinnitus, metallic taste, perioral tingling, seizures) or cardiovascular collapse. Prevention: aspiration before every injection; slow incremental injection with pause every 5 mL; ultrasound visualisation of spread.
- Pneumothorax (supraclavicular/interscalene blocks) — may not be apparent for 30–60 minutes; patient develops progressive dyspnoea and pleuritic chest pain; absent breath sounds on ipsilateral side; confirmed by ultrasound (absent lung sliding) or CXR. Small pneumothorax: observe; tension: needle decompression.
- Nerve injury — paraesthesia during needle placement or injection of LA is a warning sign; injection should be stopped immediately if the patient reports sharp, shooting pain. Post-block residual numbness beyond 48 hours should be documented and investigated.
- Local infection — more relevant with indwelling catheters; daily inspection of catheter insertion site for erythema, discharge, or tenderness.
SELF-CHECK
A patient undergoing an interscalene brachial plexus block for right shoulder surgery develops sudden dyspnoea 45 minutes after block placement, with reduced breath sounds on the right. What is the most likely diagnosis and the appropriate first step?
A. Phrenic nerve palsy causing hemidiaphragm paralysis — reassure and observe
B. Pneumothorax — perform chest ultrasound to confirm absent lung sliding, prepare for needle decompression if tension
C. Total spinal from inadvertent epidural injection — immediate intubation
D. Allergic reaction to local anaesthetic — administer adrenaline
Reveal Answer
Answer: B. Pneumothorax — perform chest ultrasound to confirm absent lung sliding, prepare for needle decompression if tension
Pneumothorax is a recognised complication of interscalene and supraclavicular blocks because the needle is placed in proximity to the lung apex. While phrenic nerve palsy is universal with interscalene block, it produces minimal symptoms in healthy patients (modest dyspnoea at worst) and does not cause absent breath sounds or pleuritic pain. Absent breath sounds with progressive dyspnoea 45 minutes post-block is pneumothorax until proven otherwise. Chest ultrasound (absent lung sliding = pneumothorax) confirms the diagnosis rapidly. If tension physiology develops (hypotension, tracheal deviation, JVD), needle decompression at the 2nd intercostal space mid-clavicular line is the immediate intervention.
Applied and Supervised Practice: Observation Framework
At the NMC 2024 competency level for AS5.3 and AS5.6, the expectation is that you observe and describe these procedures — not that you independently perform them. Supervised observation is, however, only clinically valuable if you observe actively rather than passively. This section provides a structured framework for making your observation sessions maximally educational.
Before the block: Review the block anatomy in a textbook or atlas (Morgan & Mikhail Chapter 46; Ajay Yadav's Essentials of Regional Anaesthesia). Know which nerve you are about to see blocked, its anatomical course, and the expected sensory and motor distribution. Identify the surface landmarks before the ultrasound probe is placed — can you find the axillary pulse, the femoral pulse, or the scalene triangle by palpation? Confirm you know the LA being used and its dose relative to the patient's weight.
During the block: Watch the ultrasound screen, not the needle. Identify the target nerve's characteristic hyperechoic appearance. Note how the anaesthetist positions the probe and needle to achieve in-plane visualisation. Observe the "spread" of LA as it infiltrates around the nerve — does it achieve circumferential spread? Watch for intravascular injection signs and listen to how the anaesthetist interrogates the patient during injection.
After the block: Actively participate in the block assessment — test temperature, pinprick, and motor power yourself (under supervision). Document which nerve territories are blocked and which are not. If the block is incomplete, listen to the discussion about supplementation. Ask the supervising anaesthetist to explain what they saw on ultrasound and why they chose that approach for this patient.
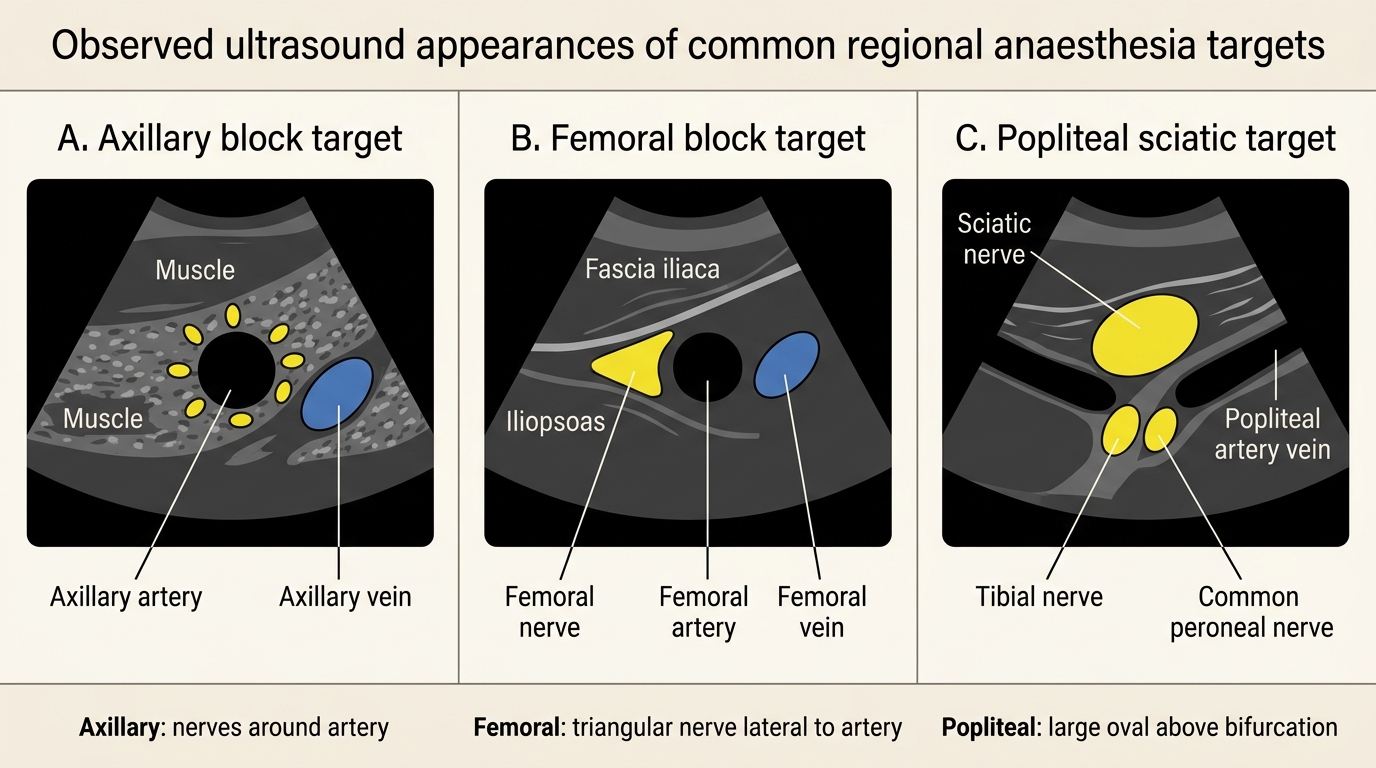
Ultrasound Appearances of Key Block Targets
Over time, watching multiple blocks builds a mental model of normal ultrasound anatomy that makes future procedural learning — when you begin to handle the probe yourself — dramatically faster. Record each block you observe in your logbook with the LA used, volume, block achieved (complete/partial), and any complications or deviations.