Page 9 of 16
AS8.4-5 | Pain Management in Palliative Care and Terminal Illness — SDL Guide
CLINICAL SCENARIO
A 62-year-old man with end-stage pancreatic cancer is referred to the palliative care team. He has not slept in three days; his pain is 9/10 on the NRS; he is on oral morphine 10 mg every six hours but it is providing only 90 minutes of relief before the pain returns. His wife says: 'The nurses tell us morphine will kill him if we give more — we'd rather he suffer than die sooner.' His palliative care physician sits down and explains three things. First, the current dose is inadequate — rapid titration is indicated and safe. Second, there is strong evidence that appropriate palliative opioid use does not shorten life in patients who are already dying — the doctrine of double effect is a theological relic here, not a clinical guide. Third, the goal of care has shifted: it is no longer cure, or even prolongation of life at the cost of suffering, but the best possible quality of the remaining time. By the end of the week, with morphine 30 mg four-hourly, subcutaneous haloperidol for nausea, a fentanyl patch for overnight stability, and a frank family conversation about goals, he is sleeping six hours each night and spending afternoons with his grandchildren. This is palliative care anaesthesiology at its most profound and most necessary.
WHY THIS MATTERS
India accounts for approximately 20% of the world's cancer burden and has one of the lowest rates of opioid availability per capita — a paradox driven by regulatory barriers, prescriber fear, and social stigma rather than clinical need. For every anaesthesiologist, physician, and surgeon who encounters patients with cancer, HIV/AIDS, end-stage organ failure, or progressive neurological disease, a working understanding of palliative pain management is not optional. It is the difference between a patient who dies in uncontrolled agony — a preventable failure of medical care — and one who dies in comfort, with dignity, surrounded by family. The NMC 2024 competencies AS8.4 (pain management in palliative care) and AS8.5 (pain management in the terminally ill) recognise this explicitly. They require a final-year medical student to describe the principles, pharmacology, routes of administration, and ethical frameworks underpinning pain management at the end of life — a domain that will be directly relevant in every clinical specialty, from oncology to geriatrics, nephrology, and general medicine.
RECALL
Recall from the preceding SDLs in this cluster: the WHO analgesic ladder prescribes 'by mouth, by the clock, by the ladder' — regular dosing to maintain analgesic steady state, with rescue doses for breakthrough pain (1/6 to 1/10 of the total daily dose, available as required). Strong opioids (morphine, oxycodone, fentanyl) have no ceiling dose for cancer pain; titration is limited only by adverse effects. Morphine-6-glucuronide (M6G) accumulates in renal failure, making fentanyl or hydromorphone preferable in significant renal impairment. Adjuvant analgesics (gabapentinoids, TCAs, corticosteroids) complement opioids for neuropathic and bone pain. These pharmacological foundations are applied directly in this module to the specific clinical context of palliative care and the actively dying patient.
Goals of Care in Palliative Medicine: The Clinical and Ethical Context
Palliative care is defined by the World Health Organization as 'an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification, assessment, and treatment of pain and other problems — physical, psychosocial, and spiritual.' Critically, this definition does not restrict palliative care to the final days of life. Modern palliative medicine endorses early integration alongside curative or disease-modifying treatment — a model supported by landmark trials demonstrating that early palliative care in patients with non-small cell lung cancer improved both quality of life and overall survival compared with standard oncological care alone.
The shift from curative to palliative intent is not a moment of abandonment — it is a reorientation of clinical goals. Where disease-directed treatment once aimed to prolong life, palliative care optimises the quality of remaining life. Four domains define the palliative care agenda: physical comfort (pain and symptom control), psychological wellbeing (anxiety, depression, existential distress), social support (family communication, practical and financial burden), and spiritual care (meaning, reconciliation, hope).
For pain specifically, the ethical framework guiding management in palliative care is grounded in the principle of beneficence — the duty to relieve suffering — balanced against the principle of non-maleficence. The widely cited doctrine of double effect — which holds that a clinician may administer an action with a good intended effect (analgesia) even if a foreseeable but unintended bad effect (respiratory depression) might result — has historically been invoked to justify opioid dose escalation in dying patients. However, contemporary evidence does not support the premise: appropriate opioid titration in patients receiving palliative care does not accelerate death. Multiple observational studies and systematic reviews have failed to demonstrate shortened survival from correctly titrated palliative opioid prescribing. The ethical justification for adequate analgesia in terminal illness is therefore straightforward beneficence, not a complex moral calculus.
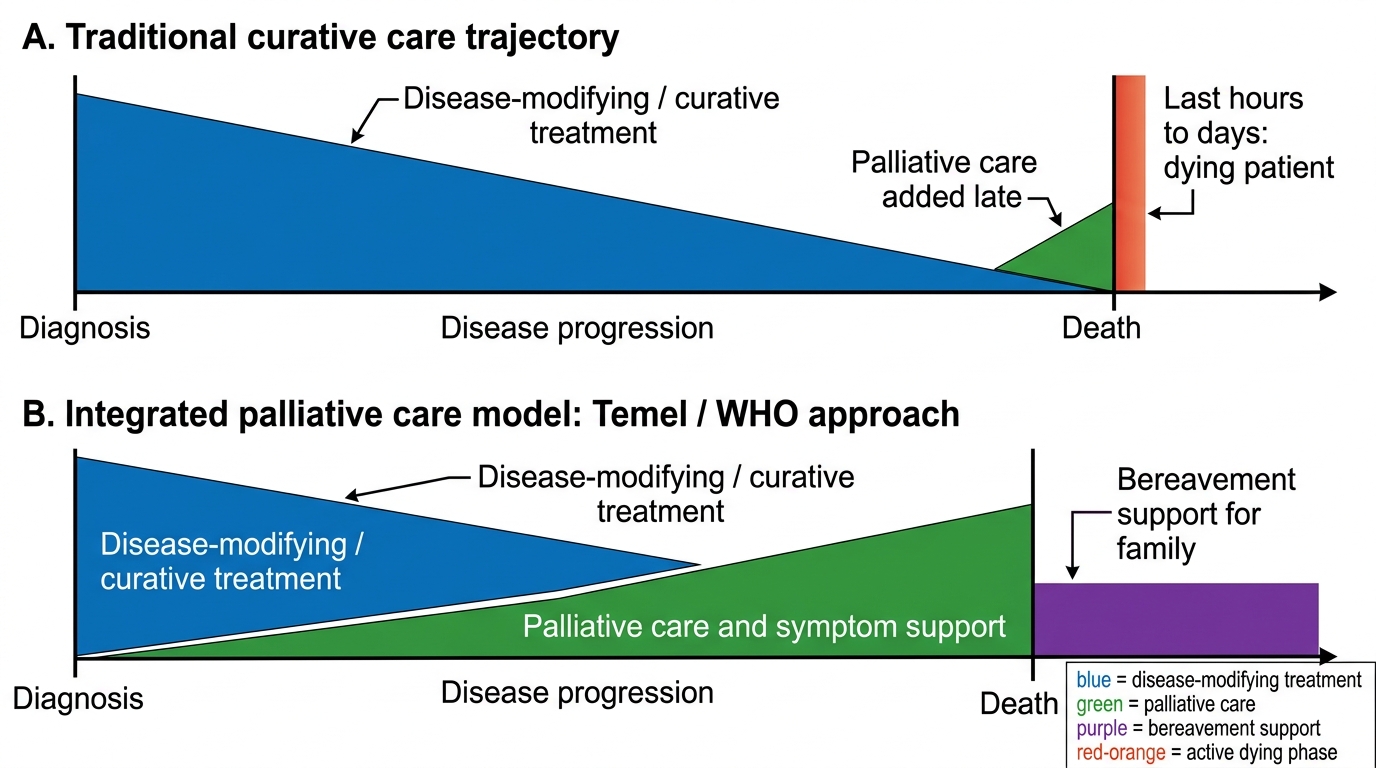
Traditional Versus Integrated Palliative Care Trajectories
The dying patient — the patient in the last hours to days of life — has specific clinical needs that differ from the patient with stable chronic or advanced illness. Common symptoms requiring active management include pain, dyspnoea (often the symptom most feared by patients and families), agitation and terminal restlessness, respiratory secretions (the 'death rattle'), nausea, and urinary retention. The anaesthesiologist and palliative care clinician must anticipate these symptoms and have management plans already prescribed — 'just in case' or anticipatory prescribing — so that symptom relief is not delayed while waiting for telephone orders at 3 AM.
Opioid Titration for Cancer Pain: Principles and Practice
Cancer pain affects 55–95% of patients at some stage of their illness and is the symptom most feared by patients with advanced malignancy. It is typically mixed in character: nociceptive somatic pain (bone metastases, surgical wounds), nociceptive visceral pain (hepatic capsule distension, bowel obstruction, peritoneal disease), and neuropathic pain (tumour infiltration of nerve plexuses, post-chemotherapy peripheral neuropathy, post-radiotherapy fibrosis). Each component may require a different pharmacological approach. The anaesthesiologist must characterise all contributing pain types before designing the analgesic regimen.
Morphine remains the first-line strong opioid for cancer pain in most resource settings, including India. The principles of morphine titration for cancer pain are as follows:
Starting doses: in opioid-naïve patients with moderate-to-severe cancer pain, oral morphine immediate-release (IR) 5–10 mg every 4 hours (with an equivalent breakthrough dose of 5–10 mg available every hour as required) is appropriate. In elderly, frail, or cachectic patients, begin at the lower end (2.5–5 mg four-hourly). Modified-release (MR) morphine provides 12-hourly dosing once the total daily requirement has been established with IR morphine — transfer by calculating the total 24-hour IR dose and dividing into two equal MR doses. A breakthrough IR dose of 1/6 to 1/10 of the total 24-hour dose remains available.
Dose escalation: if more than two or three breakthrough doses are required per 24 hours, the regular background dose is insufficient. Calculate the total opioid consumed in 24 hours (regular + breakthrough) and redistribute as the new regular dose. This arithmetic escalation — with regular reassessment — continues until pain is controlled or until adverse effects limit further dose increases. There is no maximum dose of oral morphine for cancer pain in absolute terms; doses of 1,000–2,000 mg/day are documented in heavily opioid-tolerant patients. What limits dose is the balance of analgesia against adverse effects.
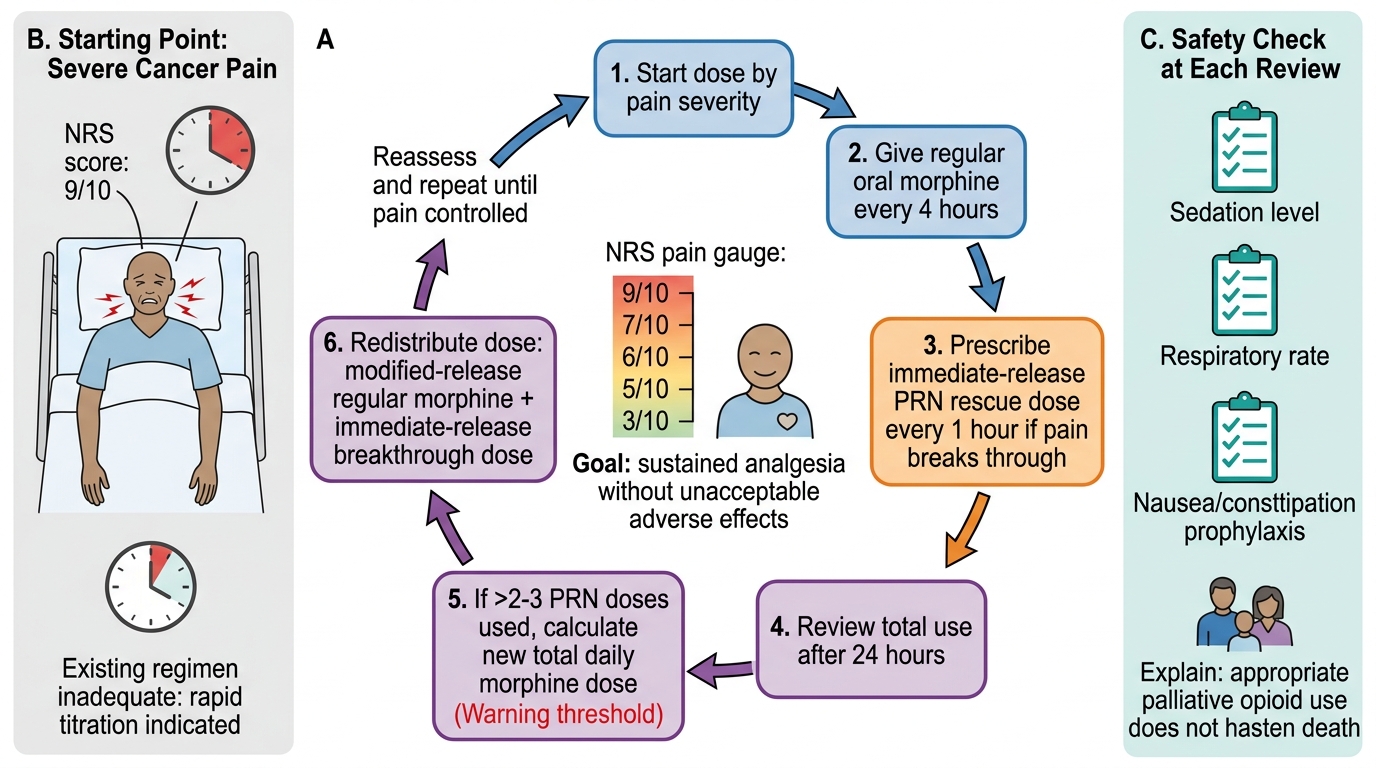
Oral Morphine Titration Cycle for Severe Cancer Pain
Opioid rotation — switching to an alternative opioid when the current one produces inadequate analgesia at the tolerated dose, or intolerable adverse effects — is a standard palliative care practice. Common indications: (1) dose-limiting neurotoxicity from morphine (myoclonus, hyperalgesia, hallucinations — often attributable to M3G accumulation in dehydrated or renally impaired patients); (2) renal impairment requiring a renally safer alternative (fentanyl, buprenorphine); (3) difficulty with oral administration requiring conversion to transdermal or parenteral route. When rotating, apply a 25–30% dose reduction of the calculated equianalgesic dose of the new opioid to account for incomplete cross-tolerance — then re-titrate.
Managing Neuropathic and Bone Pain in Advanced Cancer
Neuropathic pain in cancer is present in approximately 40% of patients with advanced malignancy and frequently co-exists with nociceptive components in a mixed pain syndrome. It is caused by tumour invasion of peripheral nerves or nerve plexuses (brachial plexopathy from apical lung tumour — Pancoast syndrome; lumbosacral plexopathy from pelvic malignancy), epidural spinal cord compression, chemotherapy-induced peripheral neuropathy, and post-herpetic neuralgia (reactivated by immunosuppression from cancer therapy). Neuropathic cancer pain is characterised by burning or electric-shock quality, allodynia, spontaneous lancinating episodes, and dermatomal distribution. It responds poorly to opioids alone and requires targeted adjuvants.
First-line adjuvants for neuropathic cancer pain include gabapentin (starting dose 100–300 mg at night, titrated up to 900–3,600 mg/day in divided doses) and pregabalin (starting dose 25–75 mg twice daily, up to 600 mg/day). These agents reduce dorsal horn excitability by blocking α₂δ calcium channel subunits. Tricyclic antidepressants (amitriptyline 10–75 mg at night) are effective but require caution in elderly patients and those with cardiac conduction abnormalities. Corticosteroids (dexamethasone 8–16 mg daily in divided doses, tapered after initial benefit) reduce peritumoural oedema compressing neural structures and provide rapid, significant pain relief in nerve compression syndromes — the mechanism is reduction of inflammatory oedema at the tumour-nerve interface.
Bone pain from skeletal metastases is an extremely common form of nociceptive cancer pain and one of the most disabling. Multiple mechanisms contribute: periosteal stretch from tumour expansion, mechanical instability from cortical destruction, cytokine-mediated direct osteoclast activation and inflammatory sensitisation of periosteal nociceptors, and nerve impingement from vertebral collapse. Management requires a combined approach:
- NSAIDs (diclofenac, naproxen) reduce prostaglandin-mediated sensitisation of bone nociceptors — particularly effective for bone pain
- Bisphosphonates (zoledronic acid IV monthly; oral ibandronate) and denosumab (anti-RANKL monoclonal antibody) reduce osteoclast activity, decrease skeletal-related events, and provide modest but documented analgesia
- Radiotherapy to metastatic lesions provides pain relief in approximately 60–70% of patients within 2–4 weeks — a standard palliative intervention
- Corticosteroids — as above
- Calcitonin has modest evidence for acute vertebral fracture pain and hypercalcaemia-related bone pain
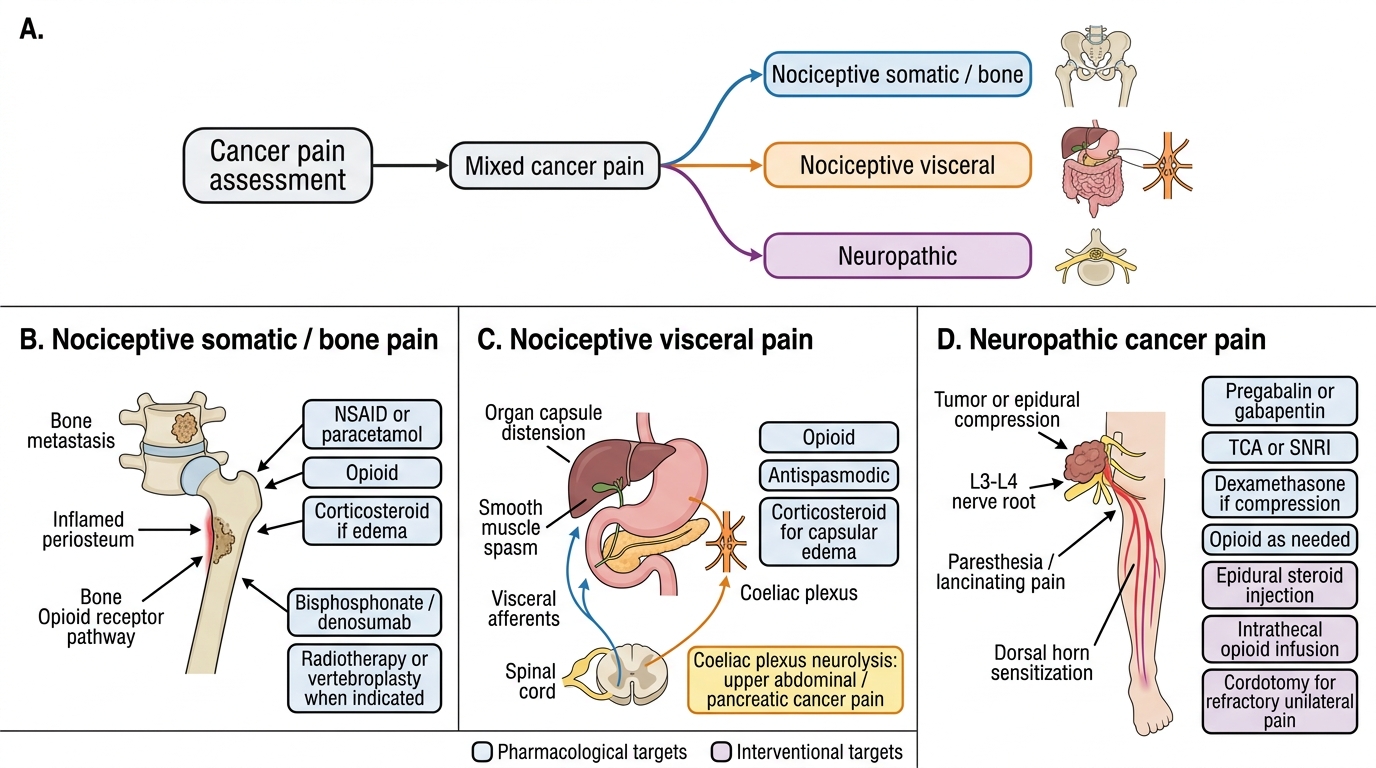
Mixed Cancer Pain: Component-Based Management
Interventional procedures — coeliac plexus neurolysis, epidural steroid injection, intrathecal opioid infusion, cordotomy — are valuable options when systemic pharmacotherapy is limited by adverse effects or inadequate efficacy, and are the domain of the specialist anaesthesiologist in palliative care. Coeliac plexus neurolysis is particularly effective for pancreatic cancer pain: destruction of the coeliac plexus with alcohol or phenol eliminates visceral afferent transmission from the upper abdominal organs and can reduce opioid requirement by 50–75% in patients with refractory upper abdominal cancer pain.
SELF-CHECK
A 55-year-old woman with advanced cervical cancer has severe lumbosacral pain with a burning, lancinating quality and paresthesia in the left leg in the L3–L4 distribution. She is currently on oral morphine 60 mg/day (modified-release) with poor pain control. Which modification to her analgesic regimen is MOST appropriate?
A. Double the morphine dose to 120 mg/day — the pain is undertreated nociceptive cancer pain
B. Add dexamethasone 8 mg daily and pregabalin 75 mg twice daily to target the neuropathic component
C. Switch to tramadol — it has dual opioid and serotonin/norepinephrine mechanisms better suited to neuropathic pain
D. Refer for radiotherapy to the lumbar spine — pharmacological management has been exhausted
Reveal Answer
Answer: B. Add dexamethasone 8 mg daily and pregabalin 75 mg twice daily to target the neuropathic component
The clinical features — burning, lancinating quality, paresthesia in an L3–L4 dermatomal distribution — indicate a neuropathic component from lumbosacral plexus involvement by cervical cancer. This pain responds poorly to opioid dose escalation alone. The correct approach is to add adjuvant analgesics targeting the neuropathic mechanism: dexamethasone reduces peritumoural oedema compressing the lumbosacral plexus (immediate effect), and pregabalin blocks α₂δ calcium channel subunits to reduce dorsal horn excitability (onset 1–2 weeks). Option A (morphine doubling) without adjuvants is unlikely to provide adequate neuropathic analgesia and risks dose-limiting toxicity. Option C (tramadol) is a Step 2 weak opioid — stepping down from Step 3 is inappropriate, and tramadol's dual mechanism does not substitute for targeted gabapentinoid therapy. Option D (immediate radiotherapy referral) is premature before optimising pharmacotherapy, though radiotherapy is a valid adjunct once pharmacotherapy is optimised.