Page 10 of 16
AS8.4-5 | Pain Management in Palliative Care and Terminal Illness — SDL Guide (Part 2)
Routes of Administration in Palliative Care: Transition from Oral to Parenteral
The oral route is always preferred when functional — it preserves patient autonomy, is cost-effective, and avoids procedural risks. However, as illness progresses, oral administration becomes impractical due to dysphagia, nausea, vomiting, reduced consciousness, severe mucositis (following chemotherapy or radiotherapy), or intestinal obstruction. The anaesthesiologist must be familiar with the clinical triggers for route change and the specific pharmacological adjustments required.
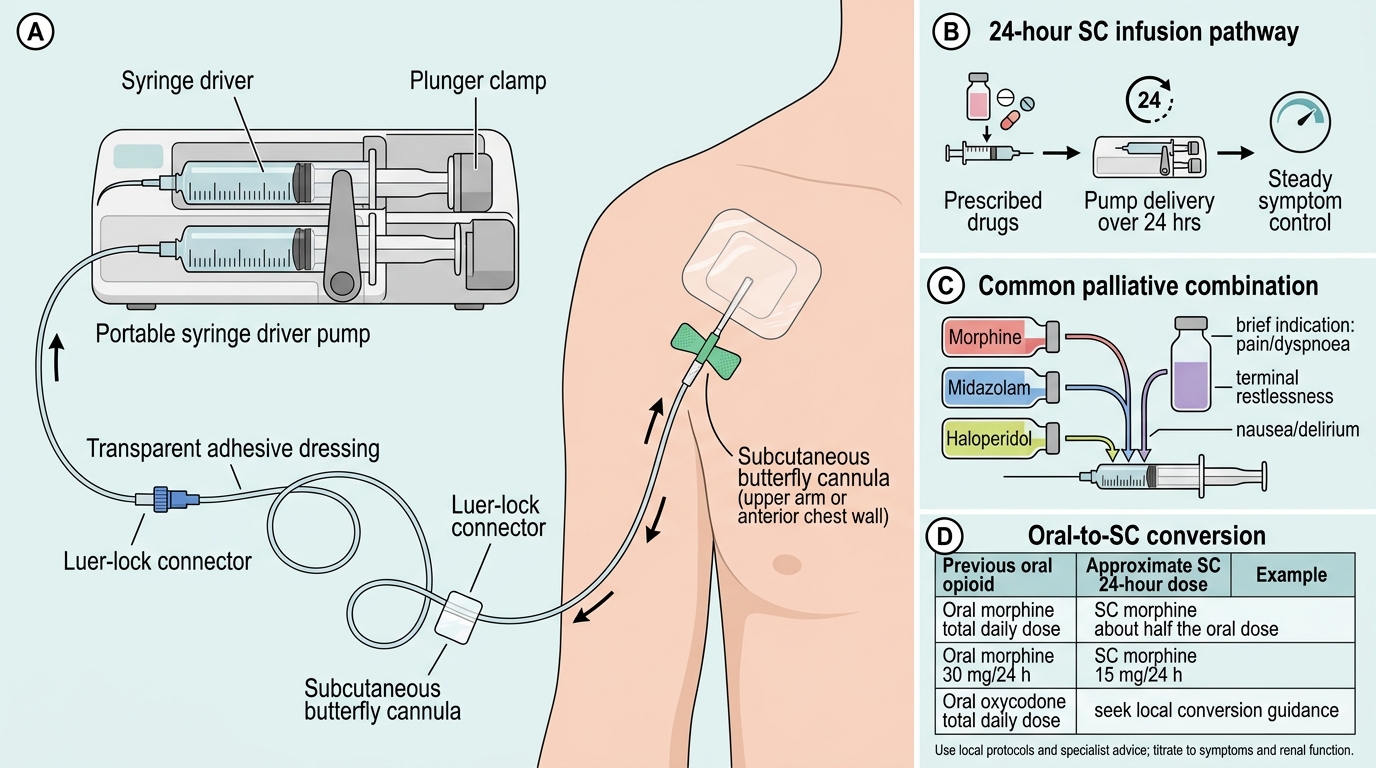
Subcutaneous (SC) infusion via a syringe driver is the gold-standard parenteral route in palliative care. A portable battery-operated syringe driver delivers a continuous SC infusion over 24 hours, maintaining stable plasma analgesic levels — avoiding the peaks and troughs associated with intermittent injections. Subcutaneous tissue absorption is reliable, sites are comfortable and accessible (anterior chest wall, upper arm, abdomen, thigh), and the device can be set up and managed by a trained nurse in a home or hospice setting. Diamorphine (diacetylmorphine) is highly water-soluble, allowing large doses in a small volume — the preferred opioid for SC infusion in the UK. Where diamorphine is not available (including India), morphine or hydromorphone can be used. Fentanyl is available as a continuous SC infusion in specialist units.
Dose conversion for route change:
- Oral morphine → SC morphine: divide oral total daily dose by 2 (SC bioavailability approximately twice that of oral)
- SC morphine → IV morphine: same dose (IV and SC morphine have approximately equal bioavailability when given by continuous infusion)
- Oral morphine → transdermal fentanyl: oral morphine 60 mg/24 h ≈ fentanyl 25 μg/h patch (allow 12–24 hours for patch to reach steady state; maintain oral breakthrough morphine during the transition period)
Compatibility of drugs in the syringe driver is clinically important. Multiple drugs are often combined in a single syringe — analgesic (morphine/diamorphine), antiemetic (metoclopramide, haloperidol, cyclizine), anxiolytic (midazolam), and antisecretory (hyoscine butylbromide). Not all combinations are compatible: cyclizine is incompatible with most opioids at concentrations above 10 mg/mL; dexamethasone is generally given separately. Palliative care formularies (e.g., the Palliative Care Formulary — PCF) must be consulted before combining drugs in a syringe driver.
Palliative Subcutaneous Syringe Driver Setup
Rectal administration (suppositories) is an underused but practical option when oral administration is temporarily unavailable and SC infusion is not immediately accessible. Morphine, oxycodone, and paracetamol are available as suppositories in many countries. Rectal bioavailability is variable (50–80% for morphine) but adequate for short-term symptom management.
Transmucosal fentanyl products (buccal tablets, intranasal sprays) provide rapid onset (5–15 minutes) and short duration (1–2 hours) — designed specifically for breakthrough cancer pain that is rapid in onset and brief in duration, which poorly matches the pharmacokinetics of oral IR morphine (30-minute onset, 4-hour duration).
Symptom Management in the Last Days of Life
In the final hours to days of life — the active dying phase — the clinical picture changes. Peripheral circulation fails, consciousness diminishes, swallowing ceases, and the oral route is no longer available. Pain may persist and require continued management via SC or IV routes. Additional symptoms — dyspnoea, terminal restlessness, respiratory secretions, and retained secretions causing the audible 'death rattle' — require anticipatory management.
Dyspnoea is extremely distressing in terminal illness and is experienced by up to 70% of dying patients. Low-dose opioids (morphine 1–2 mg SC every 4 hours in opioid-naïve patients; 25% dose increment in those already on opioids) effectively relieve the sensation of breathlessness through μ receptor-mediated reduction of respiratory drive and modification of the affective-motivational response to hypercapnia. There is strong evidence that appropriate opioid doses do not precipitately end life in this context — the primary effect is relief of suffering, not apnoea. Oxygen is indicated for dyspnoea caused by hypoxaemia but not for dyspnoea in normoxaemic patients — it does not relieve the symptom and may impose unwanted restriction.
Terminal restlessness (agitation) affects 25–85% of dying patients and is the source of greatest distress for families who witness it. Causes include uncontrolled pain, urinary retention, constipation, drug toxicity, metabolic derangement (hypercalcaemia, uraemia, hyponatraemia), and existential distress. Management: first, identify and reverse any reversible cause (catheterise for urinary retention; review and discontinue culprit drugs). If agitation persists and is causing suffering, midazolam 2.5–5 mg SC every 4 hours or by SC infusion (10–30 mg/24 h) is the first-line anxiolytic-sedative for terminal restlessness. Haloperidol 0.5–2 mg SC is useful when delirium features are prominent. Levomepromazine (methotrimeprazine) combines antiemetic, anxiolytic, and mild analgesic properties and is widely used in UK palliative care for refractory agitation.
Respiratory secretions in the dying phase are managed with hyoscine butylbromide (buscopan) 20 mg SC every 4 hours or 40–120 mg/24 h by SC infusion — an antimuscarinic agent that reduces secretion production without causing CNS adverse effects (unlike hyoscine hydrobromide, which crosses the blood-brain barrier and causes confusion). Repositioning the patient to allow secretions to drain by gravity is equally important.
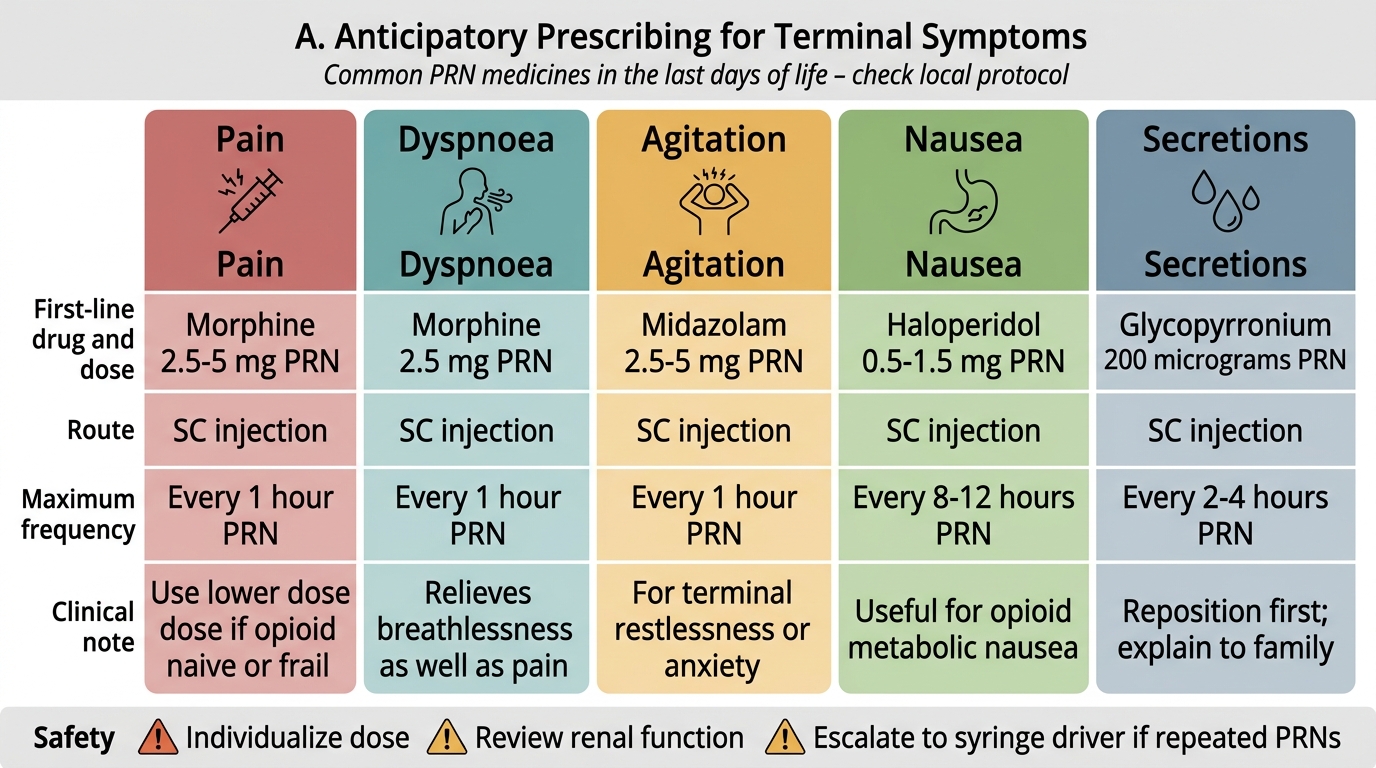
Anticipatory prescribing (also termed 'just in case' prescribing) involves writing prescriptions for the five most likely terminal symptoms — pain, dyspnoea, agitation, nausea/vomiting, and retained secretions — before they arise, so that nursing staff in home, hospice, or ward settings can administer them without delay when needed at 3 AM.
Anticipatory Prescribing in Terminal Care
Self-Assessment: Applying Palliative Pain Principles to Clinical Scenarios
Use these clinical scenarios to self-assess your mastery of NMC 2024 competencies AS8.4 and AS8.5 before the formal quiz. Work through each scenario, then check your reasoning against the principles covered in this module.
Scenario A: A 70-year-old man with advanced prostate cancer and vertebral bone metastases scores his pain at 8/10 on the NRS. He is on oral morphine MR 30 mg twice daily. His wife reports he uses six breakthrough doses daily of oral morphine IR 10 mg. What is the total 24-hour opioid consumption? What is the appropriate new regular dose? What adjuvant analgesic should be added for bone pain, and why?
Scenario B: A 58-year-old woman with end-stage ovarian cancer develops difficulty swallowing, nausea, and NRS pain 7/10. She is on oral morphine MR 60 mg twice daily. You plan to convert her to a SC morphine infusion via a syringe driver. What is the total 24-hour oral morphine dose? What SC morphine dose should be prescribed over 24 hours? What PRN SC breakthrough dose should be available, and how frequently?
Scenario C: A patient in the last 24 hours of life is unresponsive, breathing is irregular, and the family reports intermittent facial grimacing suggesting pain. The nursing team calls to ask whether to administer the anticipatory SC morphine. The family is distressed and asks whether giving morphine 'will hasten death.' How do you respond, and what action do you take?
Scenario D: A 65-year-old man with pancreatic cancer has NRS 9/10 pain, dominated by upper abdominal visceral pain that is poorly controlled despite oral morphine 120 mg/24 h plus paracetamol and NSAIDs. He is admitted for specialist palliative pain management. What interventional procedure should be discussed, and what is its mechanism and expected outcome?
Key competency check: can you state the oral morphine to SC morphine dose conversion ratio? Can you name the first-line drug and dose for terminal agitation and for respiratory secretions in the dying patient? Can you explain to a family — in plain language — why morphine does not hasten death when used for palliative symptom control? These are the practical knowledge targets of AS8.4 and AS8.5.
CLINICAL PEARL
When a patient can no longer swallow, do not wait for the on-call doctor to prescribe SC analgesia — anticipatory prescribing prevents crisis. Every patient admitted to a palliative care unit or placed on an end-of-life care pathway should have five anticipatory prescriptions written in advance: SC morphine (or equivalent opioid) for pain and dyspnoea; SC midazolam for agitation; SC haloperidol for nausea/delirium; SC hyoscine butylbromide for secretions. The dose is chosen based on the patient's current oral opioid dose and expected symptom burden. This practice, standard in UK palliative care and increasingly adopted in India's growing hospice sector, prevents the single most common preventable failure in end-of-life care: a patient dying in avoidable distress because the nurse could not reach a doctor to prescribe at 2 AM.