Page 2 of 16
AS8.1-2 | Pain Physiology and Clinical Pain Assessment — SDL Guide (Part 2)
Clinical Pain Assessment: Frameworks and Validated Tools
Accurate pain assessment is the foundation of pain management. The guiding principle, endorsed by the Joint Commission and the International Association for the Study of Pain (IASP), is that pain is what the patient says it is — subjective experience is the primary datum. No biomarker, imaging modality, or physiological measurement can replace a systematic clinical history and validated self-report tool. The anaesthesiologist's role is to elicit that history with precision, interpret it mechanistically, and translate it into an actionable analgesic plan.
A comprehensive pain history uses the SOCRATES mnemonic: Site, Onset (sudden or gradual; spontaneous or precipitated), Character (aching, burning, stabbing, throbbing, electric-shock), Radiation, Associating symptoms (nausea, allodynia, weakness, autonomic features), Time course (constant, intermittent, breakthrough), Exacerbating and relieving factors, and Severity. Character is particularly important: throbbing pain suggests vascular origin; colicky pain suggests smooth muscle spasm in a hollow viscus; burning and electric-shock qualities suggest neuropathic involvement. Radiation follows dermatomal patterns in somatic neuropathic pain (e.g., L4–L5 disc prolapse radiating to the lateral calf) or sclerotomal/referred patterns in visceral pain (e.g., cardiac ischaemia referring to the left arm and jaw).
Validated rating scales must be matched to the patient's clinical context.
- Numeric Rating Scale (NRS): patient rates pain intensity 0 (no pain) to 10 (worst imaginable pain). Simple, rapid, validated for adults with intact verbal communication. A reduction of ≥2 points or ≥33% is considered clinically significant.
- Visual Analogue Scale (VAS): a 100 mm horizontal line from 'no pain' to 'worst pain.' More precise than NRS for research but slightly more demanding for clinical use.
- Verbal Rating Scale (VRS): categorical descriptors (none, mild, moderate, severe). Useful for patients with limited numerical literacy.
- Faces Pain Scale – Revised (FPS-R): six faces ranging from neutral to extreme distress; validated for children aged 4–16 years, and also useful in cognitively impaired adults.
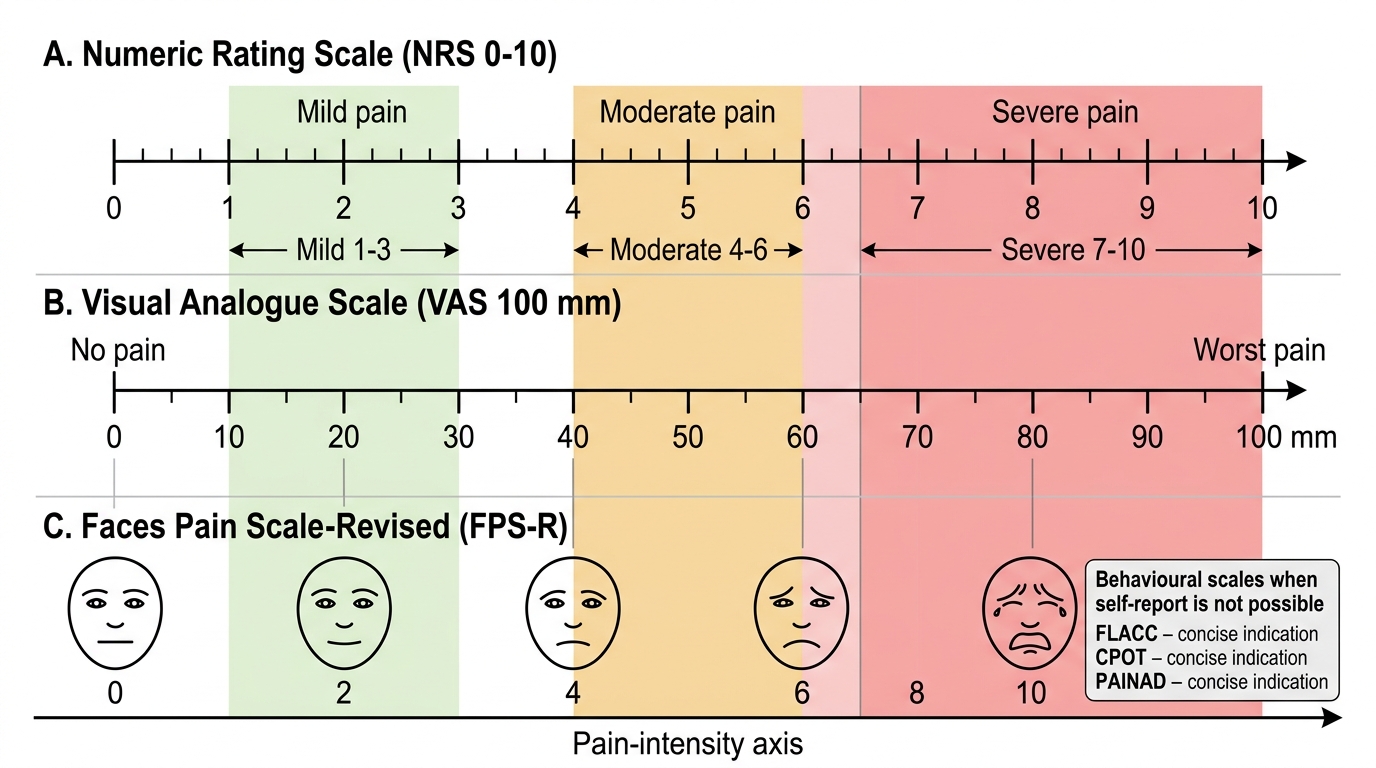
Pain Intensity Scales and Equivalence Zones
For pre-verbal children or adults who cannot self-report (e.g., severe dementia, intubated ICU patients), behavioural observation scales are used. The FLACC scale (Face, Legs, Activity, Cry, Consolability), each scored 0–2, is validated for children aged 2 months to 7 years. The Critical Care Pain Observation Tool (CPOT) assesses facial expression, body movements, muscle tension, and ventilator compliance in ICU patients. In cognitively impaired elderly patients, the PAINAD scale (Pain Assessment in Advanced Dementia) uses a similar behavioural observation framework.
Beyond intensity, a comprehensive assessment evaluates pain quality (nociceptive vs. neuropathic screening using tools such as the DN4 or PainDETECT questionnaires), temporal pattern (background pain vs. breakthrough pain or incident pain provoked by movement or procedures), functional impact (activity, sleep, mood, social function), and the patient's expectations and goals of treatment. Patients with chronic pain often do not expect or require complete elimination of pain — a reduction from 8/10 to 4/10 that allows resumption of daily activities may constitute excellent treatment.
Documentation must record the scale used, the score, the time of assessment, and the action taken — creating a structured audit trail that enables the treating team to monitor trajectory and adjust treatment rationally.
SELF-CHECK
A 45-year-old man with a herniated L5/S1 disc complains of burning, electric-shock pain radiating down the lateral aspect of his right leg, associated with allodynia to light touch over the dorsum of the right foot. The pain persists even when he is lying still. Which mechanism BEST explains these features?
A. Peripheral sensitisation of intact nociceptors by prostaglandins released from the herniated disc
B. Activation of silent nociceptors by inflammatory mediators at the disc-nerve interface
C. Injury to the L5 nerve root causing neuropathic pain with spontaneous ectopic discharge and central sensitisation
D. Referred visceral pain from a retroperitoneal structure compressing the femoral nerve
Reveal Answer
Answer: C. Injury to the L5 nerve root causing neuropathic pain with spontaneous ectopic discharge and central sensitisation
The combination of burning/electric-shock character, dermatomal radiation (L5 territory: lateral calf and dorsum of foot), allodynia, and spontaneous pain at rest are the hallmarks of neuropathic pain arising from nerve root injury. Neuropathic pain results from injury to the somatosensory nervous system itself — here, compression of the L5 root produces ectopic discharge in damaged axons and triggers central sensitisation in the dorsal horn, amplifying and sustaining the pain even without ongoing mechanical provocation. Option A (peripheral sensitisation) would produce primary hyperalgesia at the disc site, not distal allodynia. Option B (silent nociceptor activation) causes somatic nociceptive pain at the injury site. Option D is incorrect because femoral nerve territory is the anterior thigh, not the lateral calf/dorsum of foot.
Assessing Pain in Special Populations
Standard self-report pain scales assume verbal fluency, numerical literacy, and intact cognition — assumptions that fail in several important clinical groups. Adapting the assessment strategy to the patient's capacity is a core professional competency.
Paediatric assessment varies by developmental stage. Neonates and infants communicate pain through physiological responses (tachycardia, tachypnoea, oxygen desaturation) and behaviours (facial grimacing, body posturing, inconsolable crying). The NIPS (Neonatal Infant Pain Scale) and PIPP (Premature Infant Pain Profile) are validated for neonates. Infants aged 2 months to 2 years are assessed using FLACC. Children aged 3–4 years can use the Faces scale. Self-report is reliable from approximately age 5 onwards. Clinicians must avoid relying solely on the parent's perception, as parental anxiety can both over- and under-report the child's pain.
Elderly patients merit specific consideration for three reasons. First, older adults frequently under-report pain due to stoicism, fear of addiction, or resignation ('it's just old age'). Second, cognitive impairment — present in up to 50% of hospitalised patients over 80 — invalidates verbal self-report and requires behavioural scales. Third, the presence of pain catastrophising, depression, and sleep disturbance amplifies perceived pain intensity and functional impairment, making psychosocial assessment integral to the clinical evaluation.
Patients with substance use disorders present a particular challenge. Prior opioid exposure from addiction or long-term therapy produces tolerance, meaning standard analgesic doses may be inadequate. Opioid-dependent patients may also display heightened pain sensitivity — opioid-induced hyperalgesia (OIH) — where chronic opioid exposure paradoxically increases pain sensitivity through central sensitisation mechanisms including NMDA receptor upregulation. Managing acute pain in these patients requires collaboration between the anaesthesiologist and addiction medicine team, often involving methadone or buprenorphine continuation plus multimodal non-opioid analgesia.
Critically ill patients on mechanical ventilation cannot self-report and may be receiving sedatives that mask behavioural pain cues. The CPOT or Behavioural Pain Scale (BPS) should be used at standardised intervals, particularly before and after procedures known to be painful (suctioning, repositioning, drain manipulation). Inadequately treated pain in the ICU drives agitation, tachycardia, increased oxygen consumption, and — paradoxically — worsens delirium.
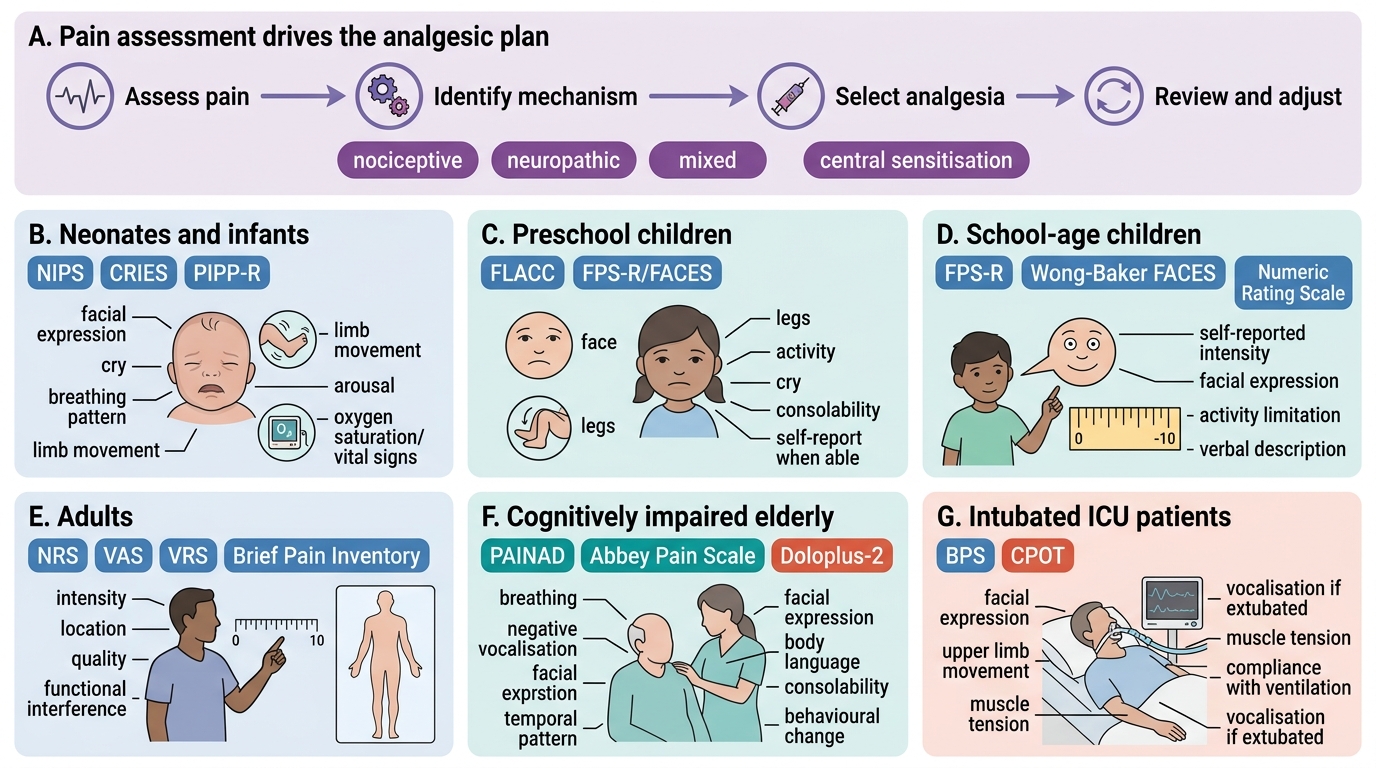
Pain Assessment Tools by Patient Population
Integrating Assessment into an Analgesic Plan
Pain assessment does not end with a number on a scale — it must generate a structured analgesic plan that is regularly reviewed. The assessment-plan-review cycle is the operational backbone of pain management.
Once a thorough assessment is complete, the anaesthesiologist synthesises the information into a mechanistic pain diagnosis: Is this predominantly nociceptive (tissue damage activating intact nociceptors — appropriate for NSAIDs, opioids, regional anaesthesia)? Neuropathic (nerve injury — requires adjuvants: gabapentinoids, TCAs, SNRIs, topical agents)? Mixed (both components — most perioperative and cancer pain scenarios)? Or central sensitisation-dominant (fibromyalgia, complex regional pain syndrome — requires centrally acting agents and psychological intervention)?
This mechanistic diagnosis directly informs analgesic selection: a patient with pure nociceptive post-operative pain from a laparotomy is managed with paracetamol, an NSAID (if not contraindicated), an opioid titrated to response, and an epidural or wound infiltration catheter — multimodal analgesia targeting multiple mechanisms simultaneously to reduce reliance on any single agent and minimise side effects. Adding a gabapentinoid to this regimen is rational for patients with pre-existing neuropathic pain or those undergoing procedures with high risk of chronic post-surgical pain (thoracotomy, mastectomy, limb amputation).
Reassessment after analgesic administration must use the same validated scale at a defined time point: typically 30 minutes after oral administration, 15 minutes after intravenous administration, and 5 minutes after neuraxial administration. A response that fails to achieve the target score (commonly NRS ≤3 for moderate-to-severe pain) triggers dose adjustment, analgesic route change, or mechanistic re-evaluation. Failure to reassess is one of the most common reasons pain remains undertreated in hospital settings.
Patient education and expectation management are also part of the assessment-to-plan pathway. Patients who understand that 'some pain after surgery is expected and manageable' and who are taught to use patient-controlled analgesia (PCA) devices correctly experience better pain outcomes than those who are given no preparation. Preoperative pain education — now a standard component of Enhanced Recovery After Surgery (ERAS) protocols — forms part of the anaesthesiologist's broader pain management role.
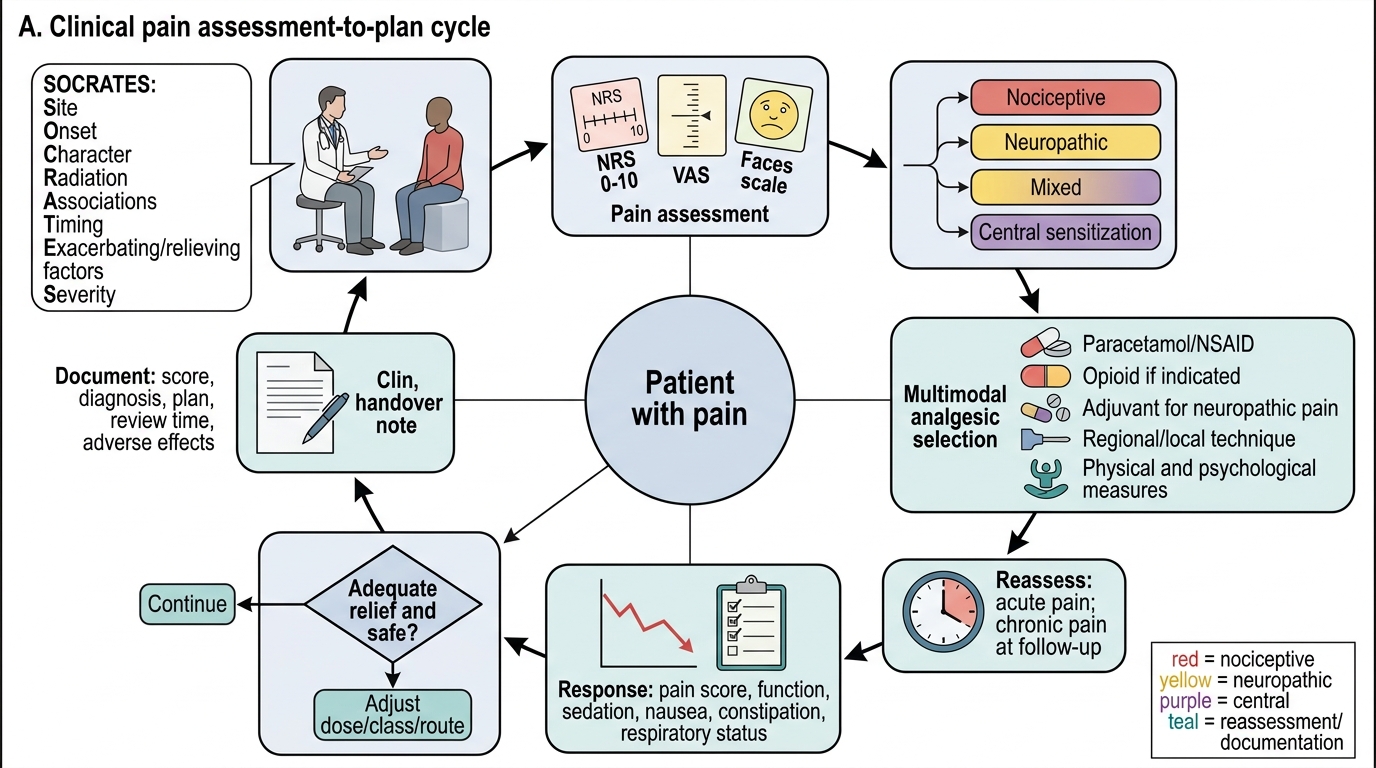
Clinical Pain Assessment-to-Plan Cycle