Page 1 of 8
AN13.1-8 | General Features, Joints, radiographs & surface marking (Upper Limb) — SDL Guide
Learning Objectives
- Describe the fascia, compartments, superficial veins, and lymphatic drainage of the upper limb (AN13.1)
- Describe the dermatomes of the upper limb and their clinical significance (AN13.2)
- Identify and describe the structure, movements, and neurovascular supply of the elbow, radio-ulnar, wrist, and first carpometacarpal joints (AN13.3)
- Describe the sternoclavicular, acromioclavicular, carpometacarpal, and metacarpophalangeal joints (AN13.4)
- Identify bones and joints of the upper limb on standard radiographs (AN13.5)
- Identify and demonstrate important bony landmarks of the upper limb on a living subject (AN13.6)
- Identify and demonstrate surface projections of major veins, arteries, and perform muscle testing (AN13.7)
- Describe the embryological development of the upper limb (AN13.8)
INSTRUCTIONS
This module is divided into 4 content parts, each followed by a self-check quiz. Read each part carefully, paying attention to bold terms — these are the key vocabulary you need. Try the self-checks before revealing answers. Use the Glossary page at the end as your revision checklist.
References
- Gray's Anatomy for Students, 4th Edition — Drake, Vogl & Mitchell (Textbook)
- Clinically Oriented Anatomy, 8th Edition — Moore, Dalley & Agur (Textbook)
- Netter's Atlas of Human Anatomy, 7th Edition (Atlas)
- Last's Anatomy: Regional and Applied, 13th Edition — Chummy S. Sinnatamby (Textbook)
Version 1.0 | Academe Content Engine
CLINICAL SCENARIO
A 22-year-old cricket player is brought to the emergency department at a government hospital in Chennai after falling on his outstretched hand during a match. The X-ray shows a fracture at the lower end of the radius. The orthopaedic resident asks: "Which joint is affected? What structures could be damaged? Can you feel the bony landmarks to assess displacement?" To answer these questions confidently, you need to understand the joints, surface anatomy, and radiographic appearance of the upper limb — exactly what this module covers.
WHY THIS MATTERS
The upper limb is the most commonly injured region in trauma cases across Indian hospitals. Whether you become an orthopaedic surgeon setting fractures, a physician examining a patient's pulse, or a paediatrician checking a newborn's limb development, you will use the knowledge from this module every single day. Understanding how to feel bony landmarks, read an X-ray, and test muscles are skills you will practise in your very first clinical posting.
You're currently studying Nerve and Muscle Physiology in Physiology — the same nerves that supply these joints also control the muscles you'll learn to test here. In Biochemistry, you're exploring calcium and phosphate homeostasis — the very minerals that give bones their hardness and make them visible on X-rays.
RECALL
Think back to your NCERT Biology class. You learned that the human skeleton has 206 bones, and that joints are places where two or more bones meet. You also know that ligaments connect bone to bone, while tendons connect muscle to bone. You've already studied anatomical terminology and general features of bones and joints in earlier weeks — so terms like diaphysis, synovial joint, flexion, and extension should be familiar.
Now imagine holding your own arm out in front of you. You can feel hard bumps at your elbow and wrist — those are bony landmarks. You can see blue lines on the inner side of your forearm — those are superficial veins. This module will teach you exactly what each of these structures is, what it does, and how to identify it on an X-ray or a living person.
Fascia and Compartments of the Upper Limb
Just as a building has walls that divide rooms, the upper limb has sheets of tough connective tissue called fascia that divide it into separate compartments. There are two layers to understand:

Figure: Fascia and Compartments of the Upper Limb
Superficial fascia is the fatty layer just beneath the skin. Think of it like the padding inside a jacket — it contains fat, cutaneous nerves, superficial veins (like the cephalic and basilic veins), and lymphatic vessels. In the palm, the superficial fascia is specially modified — it's dense and firmly bound to the underlying palmar aponeurosis (a tough sheet of tissue that helps you grip objects without the skin sliding around).
Deep fascia is a tougher, denser layer that wraps around the muscles like a tight sleeve. In the arm, it sends inward projections called intermuscular septa — the medial intermuscular septum and the lateral intermuscular septum — that divide the arm into two compartments:
- Anterior compartment (front): Contains the flexor muscles (biceps brachii, brachialis, coracobrachialis) — these bend the elbow
- Posterior compartment (back): Contains the extensor muscle (triceps brachii) — this straightens the elbow
The forearm has a similar arrangement but with an additional layer. The interosseous membrane (a tough sheet connecting the radius and ulna) creates a deeper boundary, giving the forearm three compartments: anterior (flexors), posterior (extensors), and a small lateral compartment (mobile wad of Henry — brachioradialis and the radial extensors).
Why does compartmentalisation matter? In a condition called compartment syndrome — which can occur after a fracture or crush injury — swelling within a closed compartment raises pressure dangerously high, compressing nerves and blood vessels. This is a surgical emergency because the fascia won't stretch to accommodate the swelling.
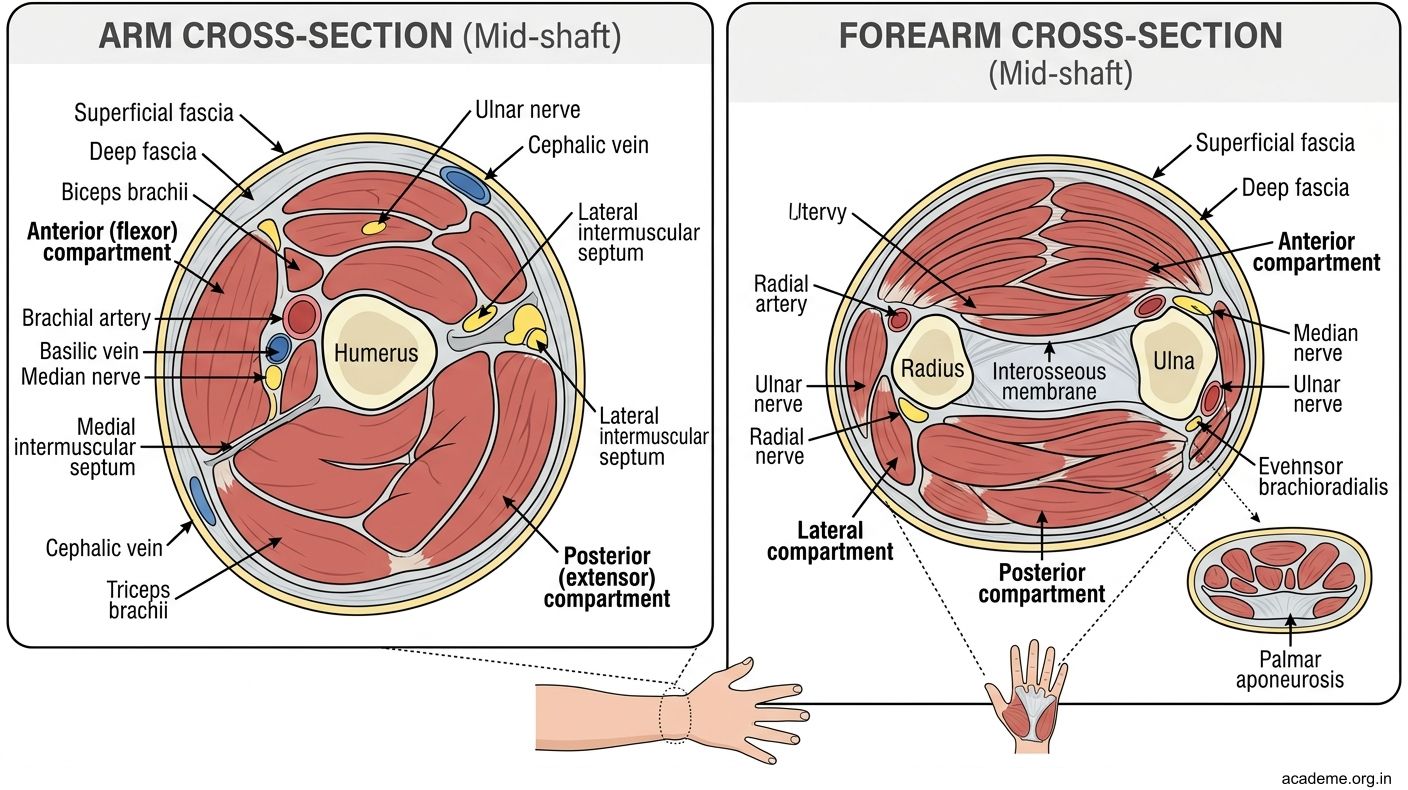
Figure: Fascia and Compartments of the Upper Limb
Superficial Veins and Lymphatic Drainage
The upper limb has two major systems for returning blood to the heart: deep veins (which run alongside arteries) and superficial veins (which run in the superficial fascia, visible through the skin).

Figure: Superficial Veins and Lymphatic Drainage
The two most important superficial veins are:
- Cephalic vein: Starts on the lateral (thumb) side of the dorsal venous arch on the back of the hand. It travels up the lateral side of the forearm and arm, runs in the deltopectoral groove (the groove between the deltoid and pectoralis major muscles), and drains into the axillary vein. Remember: C for Cephalic, C for lateral (think "C" curves outward).
- Basilic vein: Starts on the medial (little finger) side of the dorsal venous arch. It travels up the medial side of the forearm, pierces the deep fascia midway up the arm, and joins the brachial veins to form the axillary vein. Remember: B for Basilic, B for medial ("B" like "beside the Body").
At the elbow, the median cubital vein connects the cephalic to the basilic vein. This is the vein most commonly used for blood collection (venipuncture) in hospitals because it is large, superficial, and relatively fixed in position over the bicipital aponeurosis — a tough sheet that protects the brachial artery and median nerve lying just deep to it.
Lymphatic drainage follows a predictable pattern:
- Superficial lymphatics drain into cubital lymph nodes (at the elbow, near the medial epicondyle) and then to axillary lymph nodes
- Deep lymphatics follow the deep veins and also drain into axillary lymph nodes
- The axillary lymph nodes are the final common pathway — they receive lymph from the entire upper limb, the breast, and part of the thoracic wall
Clinical relevance: When a patient has breast cancer, surgeons assess the axillary lymph nodes for spread. After axillary lymph node removal, the arm may develop lymphoedema (swelling due to blocked lymph drainage) — a common complication that physiotherapists help manage.
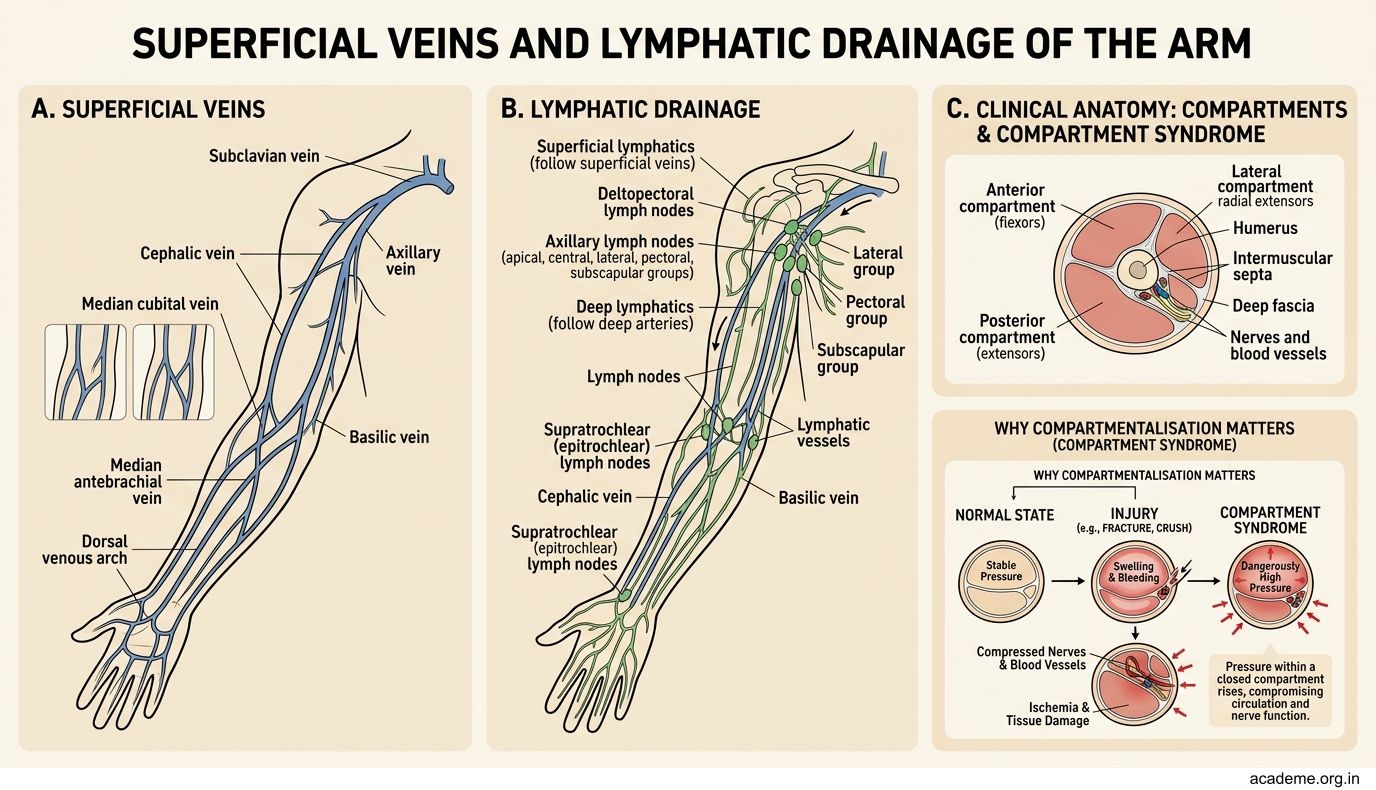
Figure: Superficial Veins and Lymphatic Drainage
Dermatomes of the Upper Limb
A dermatome is an area of skin supplied by a single spinal nerve root. Think of it like a map where each zone has its own "postcode" — the spinal nerve that carries sensation from that region to the brain.

Figure: Dermatomes of the Upper Limb
The upper limb is supplied by spinal nerves C5 through T1 (and partly T2). Here's a simple way to remember the pattern — imagine standing in the anatomical position with your arm by your side, palm facing forward:
- C5: Lateral (outer) side of the upper arm — over the deltoid region (the "regimental badge area")
- C6: Lateral forearm and thumb — if you give a thumbs-up, you're in C6 territory
- C7: Middle finger — the longest finger gets the middle nerve root
- C8: Medial (inner) forearm and little finger
- T1: Medial side of the upper arm and forearm (the area that rests against your body)
- T2: Medial arm and a small area of the axilla
Mnemonic: Think of raising your arm sideways (abduction). The highest dermatome (C5) is at the shoulder, and the numbers increase as you move down and medially toward the body — like a clock winding from lateral to medial.
Important clinical note: Dermatomes overlap significantly — loss of a single nerve root may cause only reduced (not absent) sensation. However, the "autonomous zone" of each dermatome (the central area with minimal overlap) is useful for testing:
- C6 autonomous zone: Tip of the thumb
- C7 autonomous zone: Tip of the middle finger
- C8 autonomous zone: Tip of the little finger
Dermatome knowledge is essential for diagnosing nerve root compression (as in cervical disc prolapse) and for planning nerve blocks for regional anaesthesia.
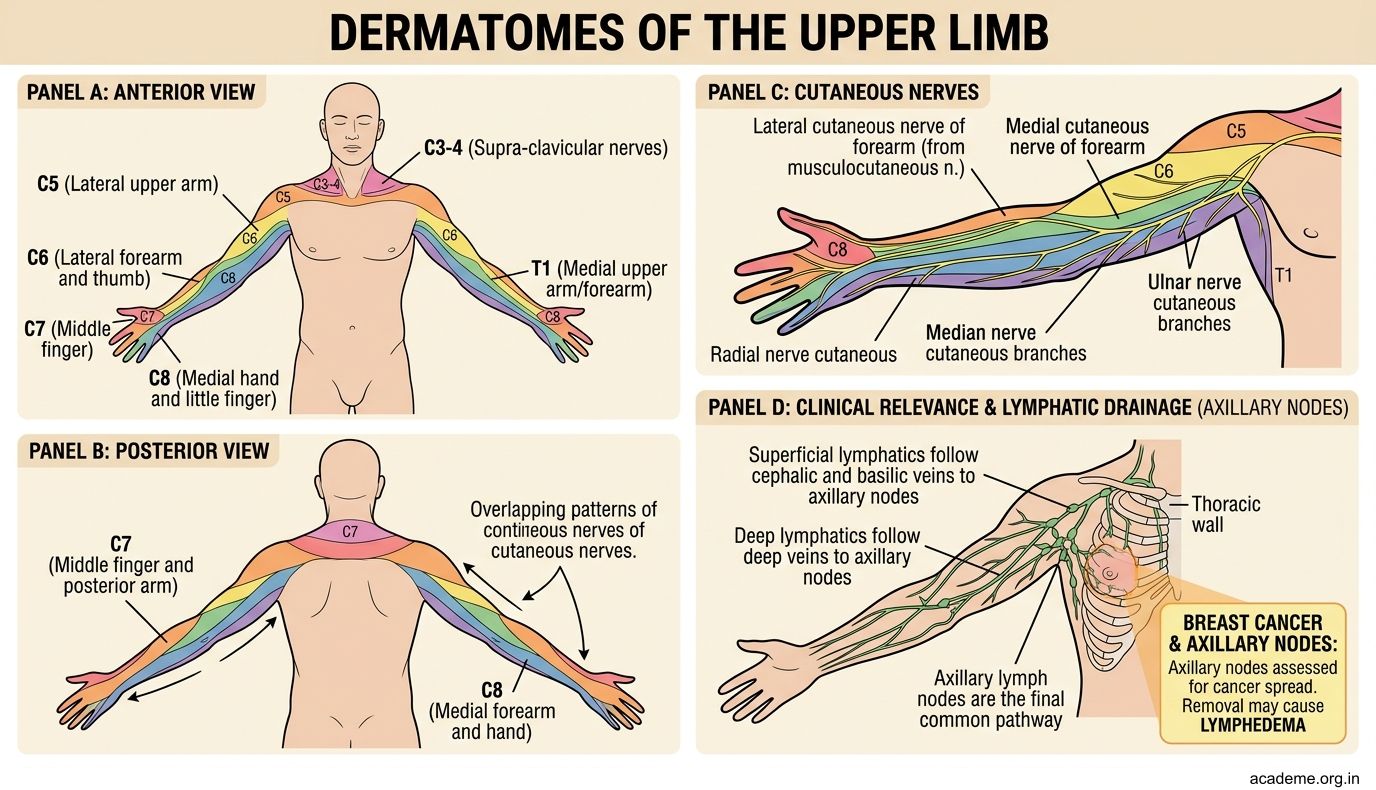
Figure: Dermatomes of the Upper Limb
SELF-CHECK — Fascia, Veins & Dermatomes
A nurse needs to draw blood from a patient. Which vein at the cubital fossa is most commonly used for venipuncture, and what structure deep to it protects the brachial artery?
A. Cephalic vein; bicipital aponeurosis
B. Median cubital vein; bicipital aponeurosis
C. Basilic vein; intermuscular septum
D. Median cubital vein; deep fascia
Reveal Answer
Answer: B. Median cubital vein; bicipital aponeurosis
A patient with cervical disc disease has reduced sensation over the tip of the thumb. Which nerve root is most likely compressed?
A. C5
B. C6
C. C7
D. C8
Reveal Answer
Answer: B. C6