Page 2 of 8
AN13.1-8 | General Features, Joints, radiographs & surface marking (Upper Limb) — SDL Guide (Part 2)
Elbow Joint
The elbow joint is a synovial hinge joint — like a door hinge, it mainly allows movement in one plane (flexion and extension). But it's actually a compound joint with three articulations sharing one joint capsule:

Figure: Elbow Joint
- Humero-ulnar joint: Between the trochlea of the humerus and the trochlear notch of the ulna — this is the main hinge
- Humero-radial joint: Between the capitulum of the humerus and the head of the radius
- Proximal radio-ulnar joint: Between the head of the radius and the radial notch of the ulna — this allows pronation and supination (turning the palm up and down)
Ligaments:
• Medial (ulnar) collateral ligament: A strong triangular ligament on the inner side. It has three parts — anterior, posterior, and transverse bands. This ligament is commonly injured in throwing sports ("Tommy John injury" in baseball — or cricket fast bowlers in the Indian context).
• Lateral (radial) collateral ligament: On the outer side, blending with the annular ligament
• Annular ligament: A ring-shaped ligament that wraps around the head of the radius like a collar, holding it in place while allowing it to rotate. In young children, a sudden pull on the arm can cause the radial head to slip partially out of this ring — called a "pulled elbow" or nursery maid's elbow, commonly seen in paediatric OPDs across India.
Movements:
• Flexion (0-150°): Biceps brachii, brachialis, brachioradialis
• Extension (back to 0°): Triceps brachii, anconeus
• The carrying angle (10-15°, greater in females) is the slight lateral angulation at the elbow that allows the forearm to clear the hip when carrying objects
Blood supply: Anastomosis around the elbow from branches of the brachial, radial, and ulnar arteries
Nerve supply: Musculocutaneous, radial, median, and ulnar nerves (Hilton's Law — the nerves supplying muscles acting on a joint also supply that joint itself)
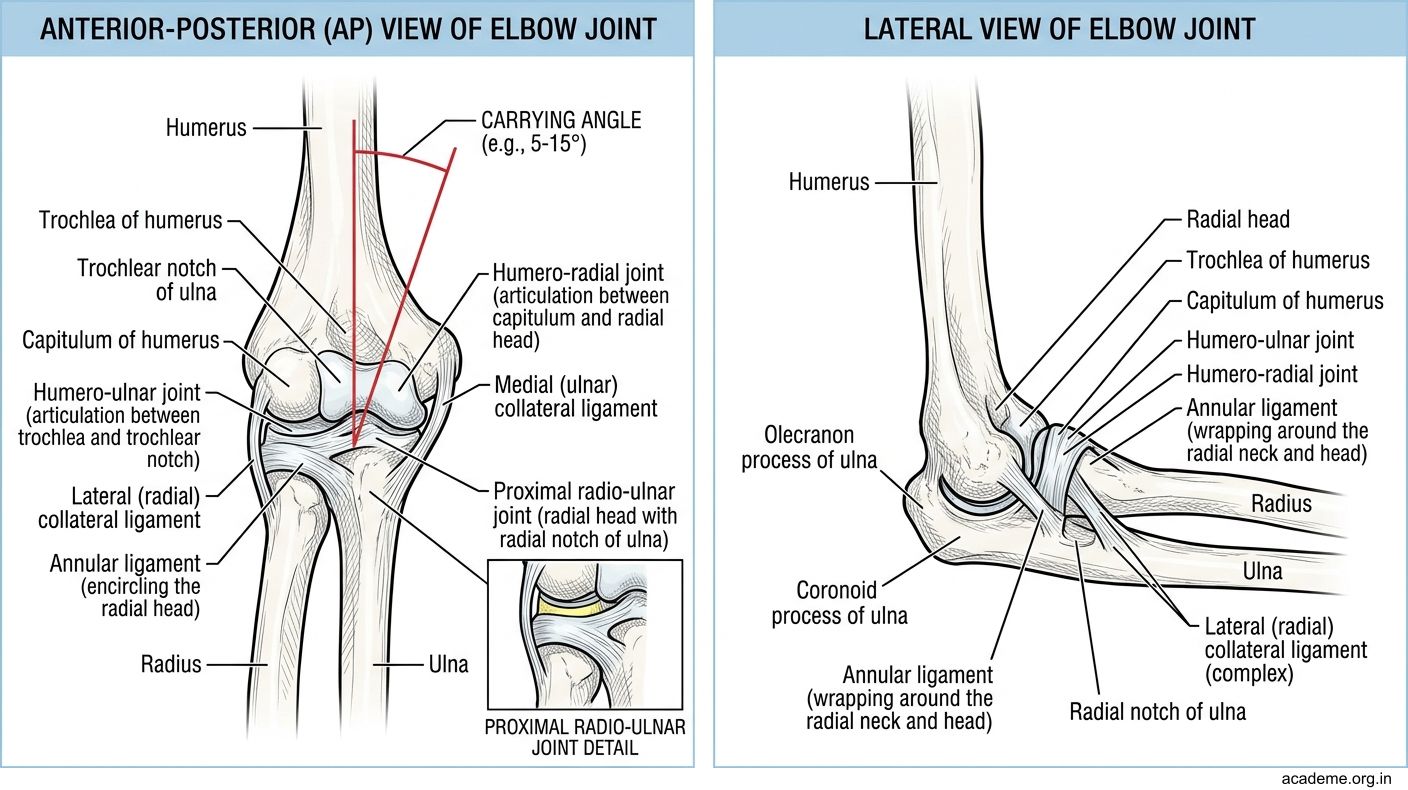
Figure: Elbow Joint
Radio-ulnar Joints and Wrist Joint
Proximal radio-ulnar joint (described above with the elbow) and distal radio-ulnar joint work together to produce pronation (turning the palm downward/backward) and supination (turning the palm upward/forward). Imagine turning a doorknob — the radius rotates around the ulna while the ulna stays relatively still.

Figure: Radio-ulnar Joints and Wrist Joint
The distal radio-ulnar joint is a pivot joint between the head of the ulna and the ulnar notch of the radius. An articular disc (triangular fibrocartilage complex, or TFCC) separates this joint from the wrist joint. TFCC injuries are common in falls on the outstretched hand and cause persistent wrist pain on the ulnar (little finger) side.
Wrist joint (radiocarpal joint) is a synovial ellipsoid joint between:
• Proximal surface: Lower end of the radius + articular disc (ulna does NOT directly articulate with the carpal bones)
• Distal surface: Scaphoid, lunate, and triquetral bones (proximal row of carpal bones)
Movements at the wrist:
• Flexion: Flexor carpi radialis, flexor carpi ulnaris, palmaris longus
• Extension: Extensor carpi radialis longus & brevis, extensor carpi ulnaris
• Abduction (radial deviation): Flexor carpi radialis + extensor carpi radialis longus & brevis
• Adduction (ulnar deviation): Flexor carpi ulnaris + extensor carpi ulnaris
• No rotation occurs at the wrist — what appears to be wrist rotation is actually pronation/supination at the radio-ulnar joints
Blood supply: Dorsal and palmar carpal arches (branches of radial and ulnar arteries)
Nerve supply: Anterior interosseous nerve (median) and posterior interosseous nerve (radial)
Clinical note: The scaphoid bone is the most commonly fractured carpal bone (from falls on outstretched hand). It's notorious because fracture may not show on initial X-ray and has a risk of avascular necrosis due to its retrograde blood supply (blood enters from the distal end).
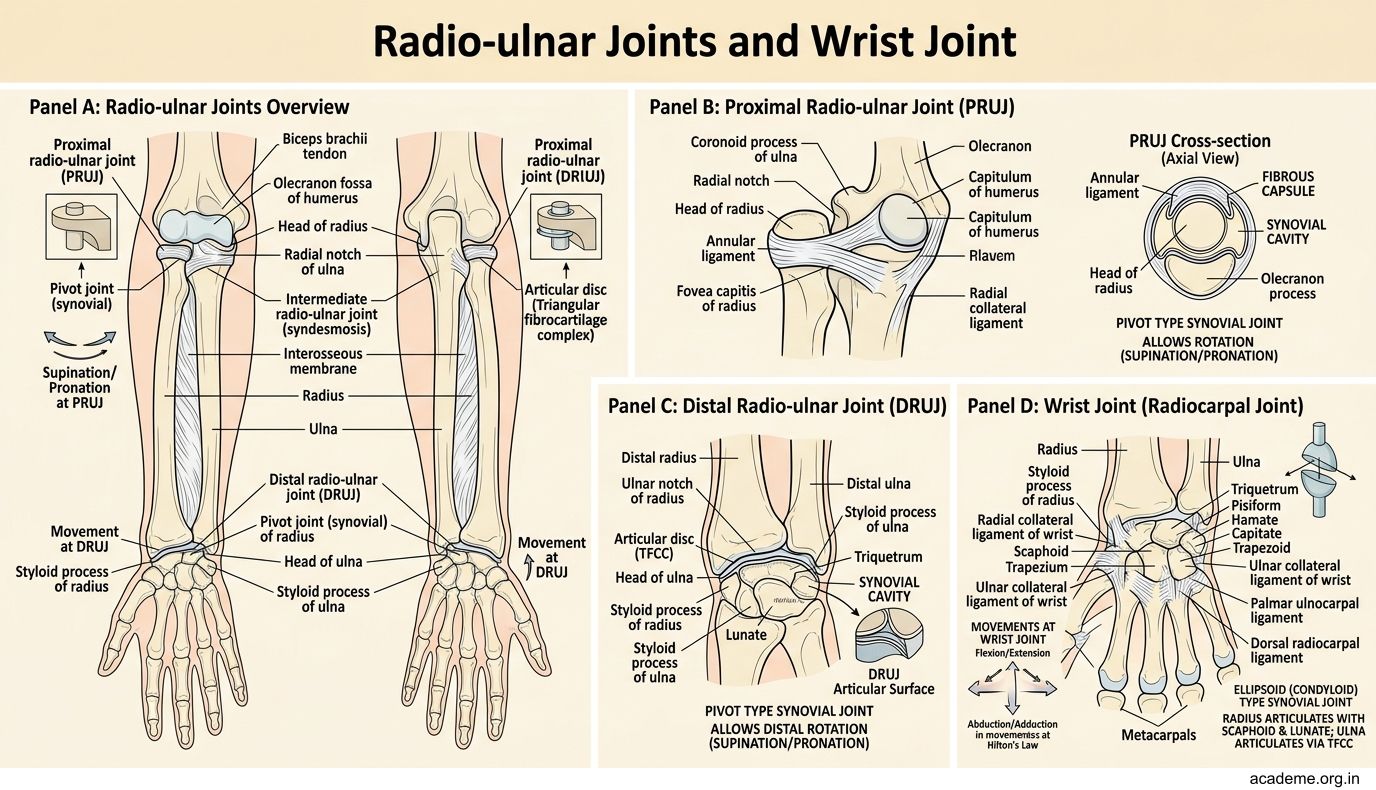
Figure: Radio-ulnar Joints and Wrist Joint
First Carpometacarpal Joint and Other Joints
The first carpometacarpal (CMC) joint is special — it's a saddle joint between the trapezium bone and the base of the first metacarpal. Just as a horse rider sits in a saddle that curves in two directions, the articular surfaces of this joint are concave in one plane and convex at right angles to it.

Figure: Metacarpophalangeal (MCP) joints

Figure: Acromioclavicular (AC) joint

Figure: Other joints to know:

Figure: First Carpometacarpal Joint and Other Joints
This unique design allows the thumb to perform opposition — the ability to touch the tips of all other fingers. Opposition is what makes the human hand so versatile for gripping, writing, and performing surgery. It involves a combination of flexion, medial rotation, and adduction.
Movements of the first CMC joint:
• Flexion/Extension (in the plane of the palm)
• Abduction/Adduction (perpendicular to the palm)
• Opposition/Reposition
• Circumduction
Osteoarthritis of the first CMC joint is very common (especially in older women) and causes pain at the base of the thumb during gripping activities — opening jars becomes painful.
Other joints to know:
Sternoclavicular (SC) joint: The ONLY bony connection between the upper limb and the axial skeleton. It's a saddle-type synovial joint with an intra-articular disc. Despite being small, it's remarkably strong — dislocation is rare; the clavicle usually fractures first.
Acromioclavicular (AC) joint: A plane synovial joint between the acromion of the scapula and the lateral end of the clavicle. Stabilised by the coracoclavicular ligament (conoid + trapezoid). AC joint injuries are common in contact sports — graded I to VI based on the degree of separation.
Metacarpophalangeal (MCP) joints: Condyloid (ellipsoid) joints that allow flexion, extension, abduction, adduction, and circumduction. The collateral ligaments are slack in extension and taut in flexion — this is why, if a hand must be immobilised, it should be splinted in the "position of safety" (MCPs flexed at 70-90°) to prevent contracture of these ligaments.
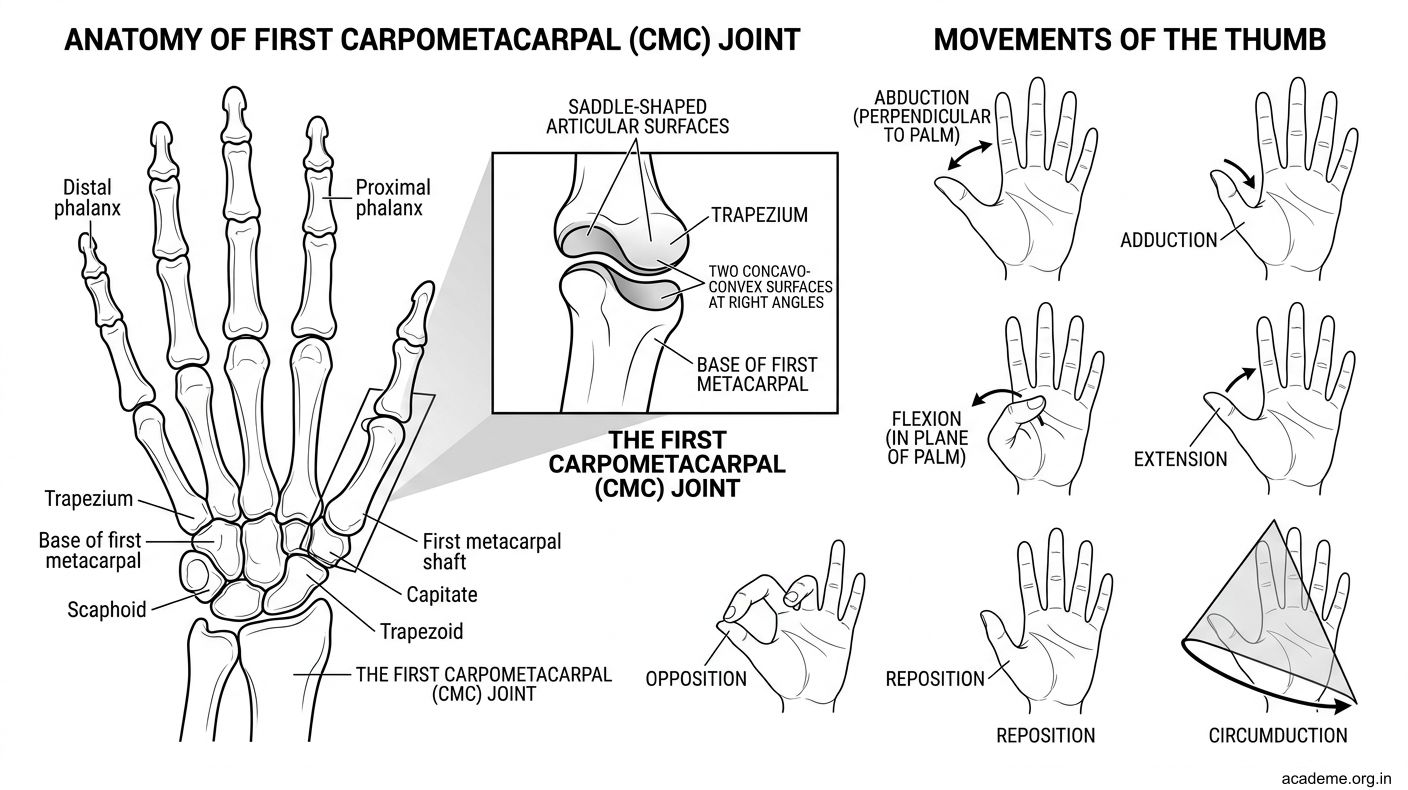
Figure: First Carpometacarpal Joint and Other Joints
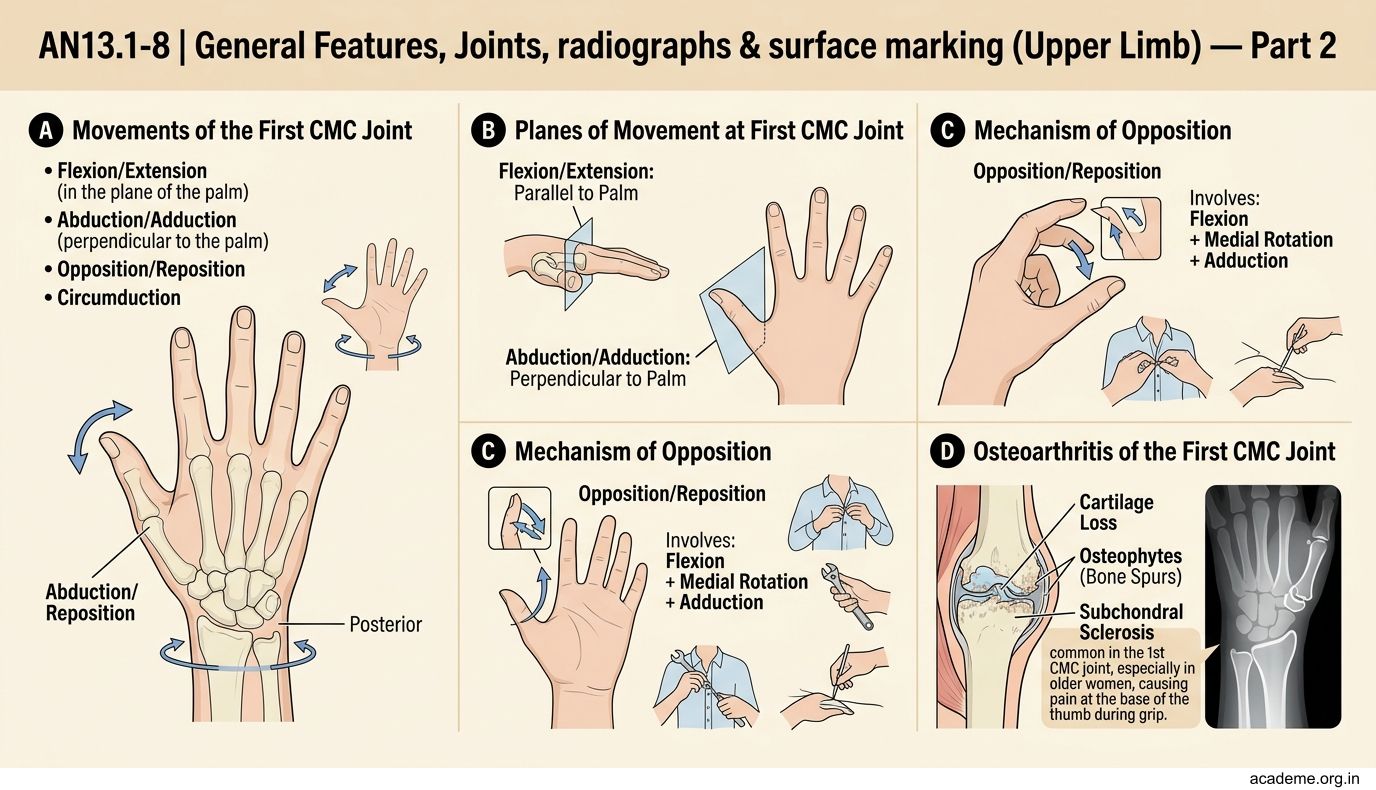
Figure: Other joints to know:
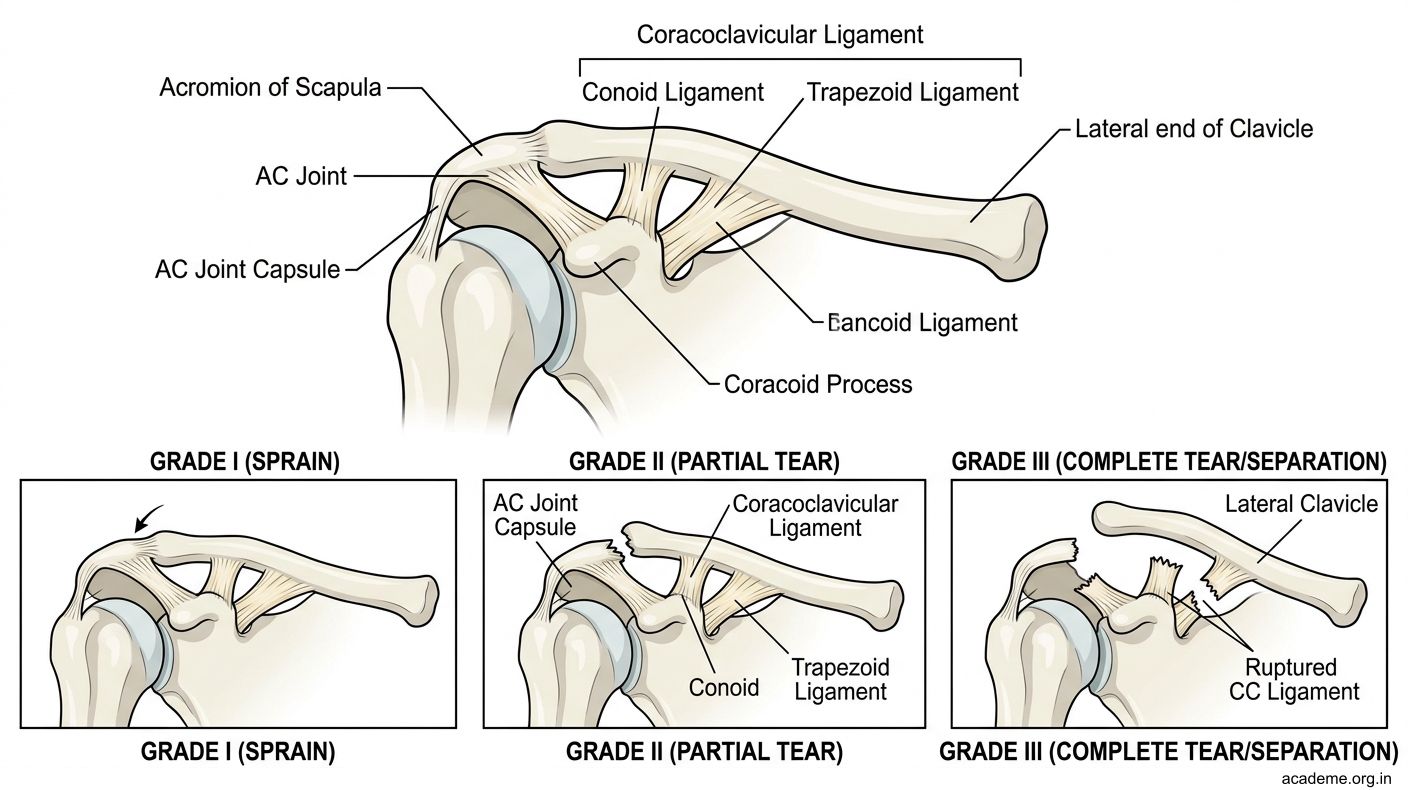
Figure: Acromioclavicular (AC) joint
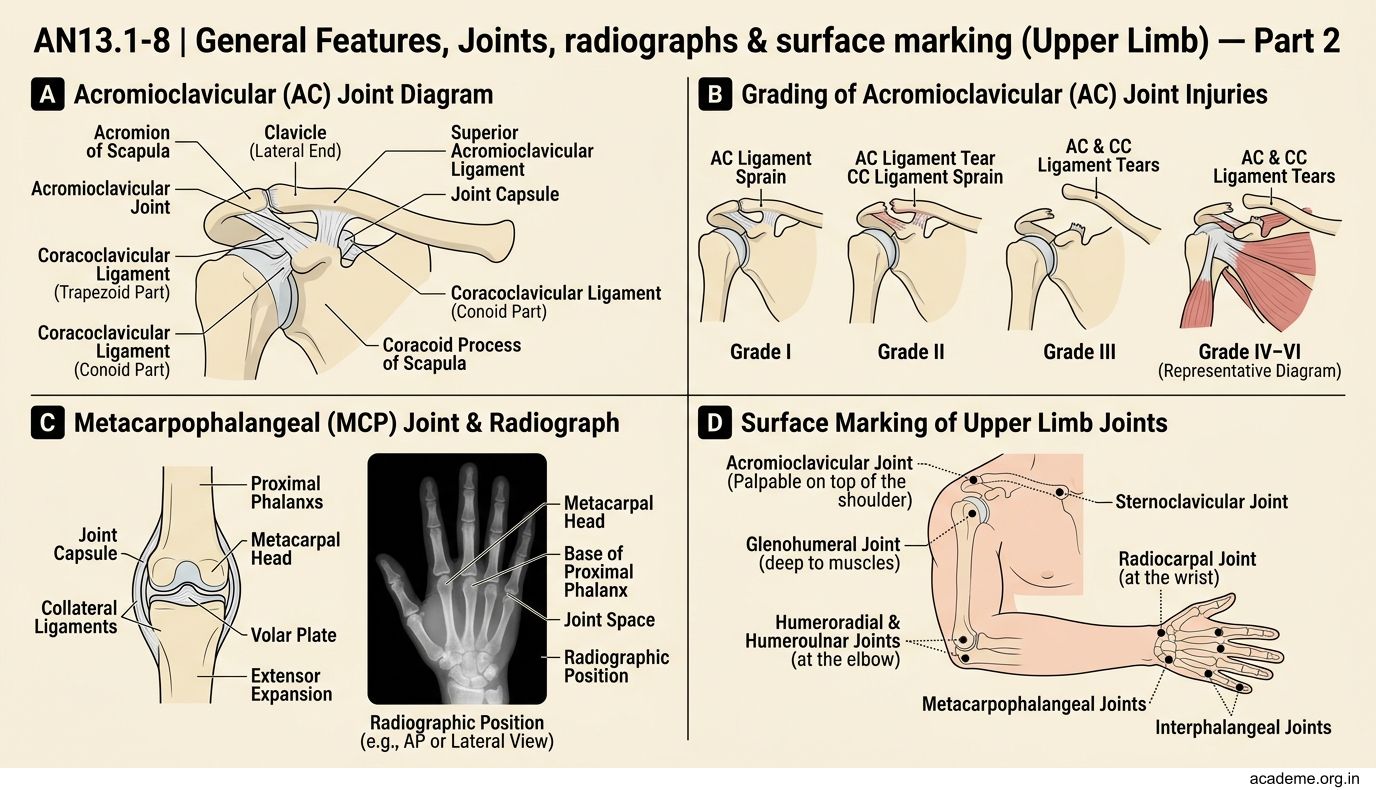
Figure: Metacarpophalangeal (MCP) joints
CLINICAL PEARL
Position of Safety for Hand Splinting: When immobilising an injured hand, always splint with the wrist in 20-30° extension, MCPs flexed at 70-90°, and IPs in slight flexion. This is called the "Edinburgh position" or position of safety. It keeps the collateral ligaments of the MCP joints at maximum stretch, preventing the fibrosis and shortening that would make the fingers permanently stiff. You'll see this applied routinely in orthopaedic and plastic surgery wards.
SELF-CHECK — Joints of the Upper Limb
A 3-year-old child is brought to the paediatric OPD after her mother pulled her by the hand while crossing the road. The child is crying and holding her forearm in pronation. What is the most likely diagnosis?
A. Fracture of the radial head
B. Pulled elbow (subluxation of the radial head)
C. Dislocation of the elbow joint
D. Fracture of the olecranon
Reveal Answer
Answer: B. Pulled elbow (subluxation of the radial head)
Which is the ONLY bony articulation connecting the upper limb skeleton to the axial skeleton?
A. Acromioclavicular joint
B. Shoulder joint
C. Sternoclavicular joint
D. Scapulothoracic joint
Reveal Answer
Answer: C. Sternoclavicular joint