Page 1 of 8
AN20.1-10 | General Features, Joints, radiographs & surface marking (Lower Limb) — SDL Guide
Learning Objectives
- Describe the ankle (talocrural) joint — type, articular surfaces, ligaments, movements, blood and nerve supply (AN20.1)
- Describe the subtalar and transverse tarsal (Chopart) joints and their clinical significance (AN20.2)
- Describe fascia lata, venous drainage, lymphatic drainage, retinacula, and dermatomes of the lower limb (AN20.3)
- Explain the anatomical basis of enlarged inguinal lymph nodes and their clinical significance (AN20.4)
- Explain the anatomical basis of varicose veins and deep vein thrombosis (AN20.5)
- Identify bones and joints of the lower limb on anteroposterior and lateral radiographs (AN20.6)
- Identify and demonstrate important bony landmarks of the lower limb (AN20.7)
- Demonstrate palpation of the femoral, popliteal, posterior tibial, anterior tibial, and dorsalis pedis arteries (AN20.8)
- Demonstrate surface projection of lower limb arteries, veins, and nerves (AN20.9)
- Describe the basic concept of development of the lower limb (AN20.10)
INSTRUCTIONS
This is a comprehensive integrative module covering joints, radiographs, surface anatomy, and clinical conditions of the lower limb. The module has 12 blocks — read sequentially. Use the surface anatomy section actively: palpate the landmarks on your own leg as you read. The radiograph section includes annotated descriptions — visualise each bone as you read.
References
CLINICAL SCENARIO
A 70-year-old retired government officer from Pondicherry presents to the vascular surgery OPD with a 3-year history of right leg swelling, brownish skin discolouration above the medial malleolus, and a painful ulcer over the same area. He has visible tortuous veins on the medial side of his leg. His left leg shows similar early changes.
He has had varicose veins since his 40s. His wife adds: 'Last year he had a swollen red leg after a long bus journey to Chennai — they gave him blood thinners at the district hospital.'
This patient has chronic venous insufficiency from varicose veins with a prior DVT — a textbook Lower Limb General Features case. By the end of this module, you'll understand the anatomy behind every finding: why the ulcer is above the medial malleolus, why the DVT happened after the bus journey, and how to find his pulses, draw his veins, and interpret his X-rays.
WHY THIS MATTERS
This integrative module maps to the most clinically tested areas in lower limb anatomy:
- Ankle joint anatomy: The most commonly injured joint in sports; Pott's fracture patterns follow ligamentous anatomy
- Varicose veins & DVT: Extremely common in Indian surgical wards and OPDs
- Lymphadenopathy: Inguinal lymph nodes are palpated in every lower limb examination — infected toe? → inguinal nodes
- Pulse palpation: All 5 LL pulses are tested in clinical examinations (MBBS and PG entrance)
- Surface anatomy: Required for femoral vein cannulation, nerve blocks, saphenous vein cutdown — all essential procedures
- Radiograph reading: Every musculoskeletal OPD requires AP and lateral X-ray interpretation of the hip, knee, and ankle
RECALL
Connect this module to earlier learning:
- Hip joint: Ball-and-socket synovial joint; femoral head in acetabulum; capsule reinforced by iliofemoral (strongest), pubofemoral, ischiofemoral ligaments
- Knee joint: Most complex joint; hinge with rotation; medial and lateral collateral ligaments + cruciate ligaments + menisci
- Arteries: External iliac → femoral → popliteal → anterior tibial + posterior tibial
- Sciatic nerve: L4-S3; bifurcates at apex of popliteal fossa into tibial + common peroneal nerves
- Dermatomes: Medial thigh = obturator (L2,3); anterior thigh = femoral (L2,3,4); medial leg/foot = saphenous (L4); lateral leg = superficial peroneal (L5); dorsum of foot = deep peroneal; sole = tibial (S1,2)
Ankle (Talocrural) Joint
The ankle joint is a synovial hinge joint — the most commonly injured joint in the body.

Figure: Articular surfaces

Figure: Ankle (Talocrural) Joint
Articular surfaces:
- Above: Lower articular surface of the tibia (tibial plafond) + medial malleolus of tibia + lateral malleolus of fibula → form the 'mortise'
- Below: Superior surface (trochlea) of the talus → the 'tenon' fitting into the mortise
- Note: Fibula carries only 10-15% of axial load but is critical for ankle stability
Capsule: Thin anteriorly and posteriorly, thickened on sides as collateral ligaments
Medial (Deltoid) Ligament — strong, fan-shaped, in 4 parts:
- Anterior tibiotalar, Posterior tibiotalar, Tibiocalcaneal, Tibionavicular
- Resists excessive eversion — rarely torn alone; its strength often causes avulsion fractures of medial malleolus instead
Lateral Ligament — 3 separate bands (weaker):
- ATFL (anterior talofibular) — most commonly torn in ankle sprains (inversion injury)
- CFL (calcaneofibular)
- PTFL (posterior talofibular) — rarely torn
Movements:
- Plantarflexion (40°): gastrocnemius, soleus
- Dorsiflexion (20°): tibialis anterior, EDL, peroneus tertius
- Note: Inversion/eversion occur at subtalar joint, NOT the ankle joint
Blood supply: Branches of anterior tibial, posterior tibial, peroneal arteries
Nerve supply: Deep peroneal nerve, tibial nerve, sural nerve
Clinical — Pott's Fracture-Dislocation:
Inversion + plantarflexion mechanism → ATFL torn → then CFL → then avulsion of fibula tip or spiral fibula fracture. Eversion force → medial malleolus avulsion. High-energy → bimalleolar or trimalleolar (posterior malleolus of tibia = 3rd malleolus) fractures.
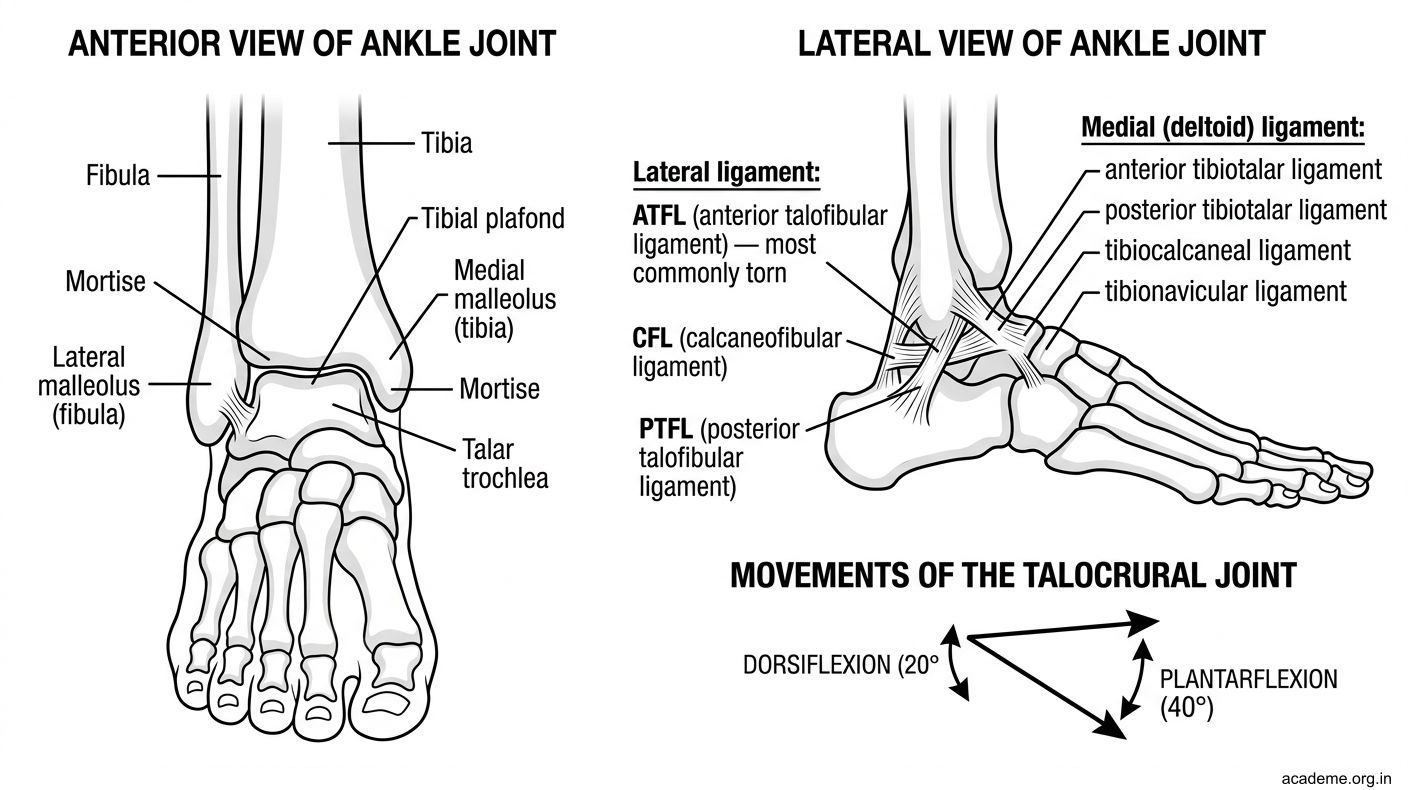
Figure: Ankle (Talocrural) Joint
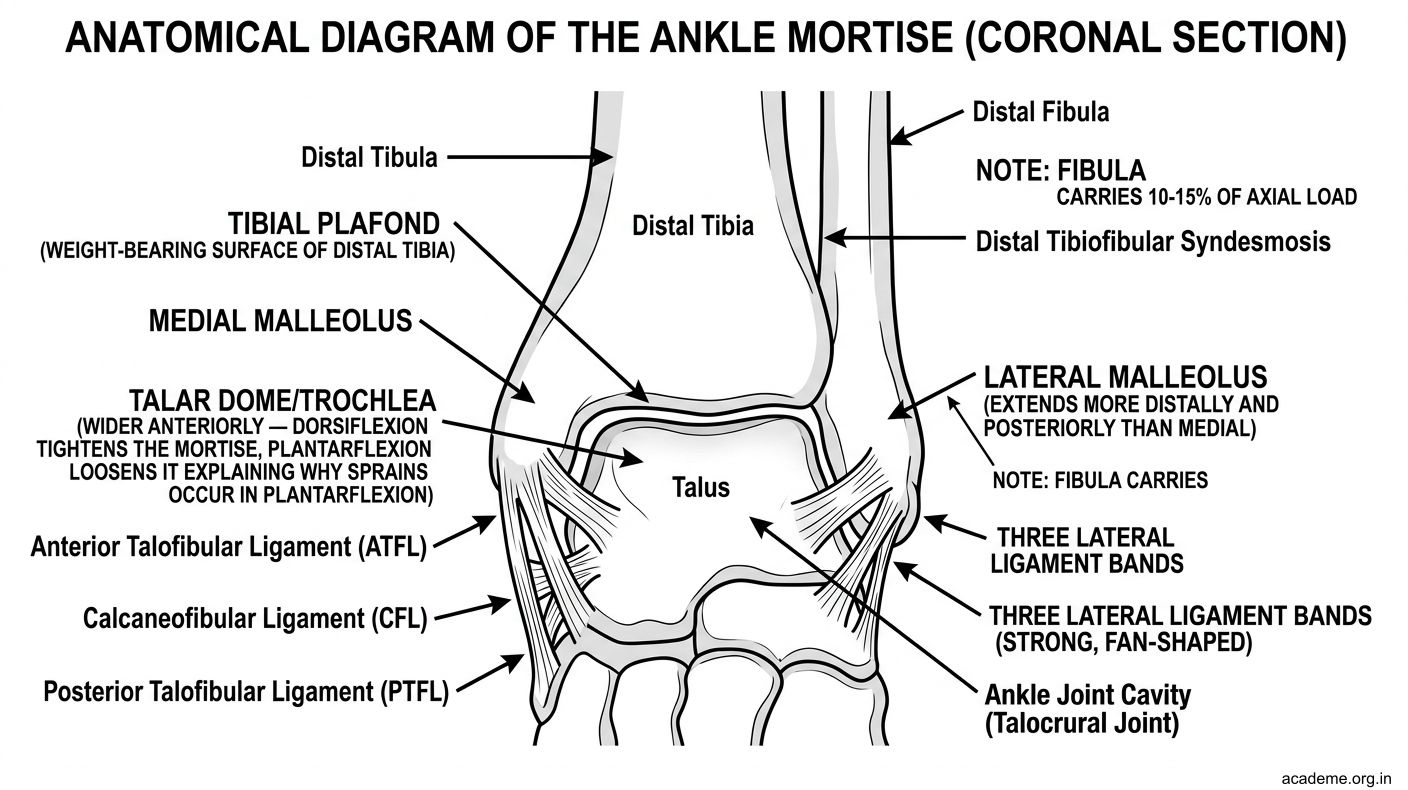
Figure: Articular surfaces
Subtalar & Transverse Tarsal Joints
Subtalar Joint (Talocalcaneal Joint)
- Type: Modified plane synovial joint with separate anterior and posterior joint cavities
- Articular surfaces: Inferior surface of talus on superior surface of calcaneus
- Movements: Inversion and eversion of the foot — this is the primary joint for inversion/eversion, NOT the ankle
- Supported by: Interosseous talocalcaneal ligament (strongest), medial and lateral talocalcaneal ligaments, cervical ligament
- Clinical: Subtalar fusion is done for severe subtalar arthritis (e.g., post-fracture) — eliminates inversion/eversion → stiff foot on uneven ground
Transverse Tarsal Joint (Midtarsal / Chopart's Joint)
- Two joints working together:
- Talonavicular joint (medial): ball-and-socket between talar head and navicular
- Calcaneocuboid joint (lateral): saddle joint between calcaneus and cuboid
- Combined axis allows: adduction/abduction + supination/pronation of forefoot
- Chopart amputation: Amputation through the transverse tarsal joint — preserves the hindfoot with its tendons attached, maintaining some propulsion
- Lisfranc joint: Tarsometatarsal joint — Lisfranc injury (ligamentous rupture with dislocation) is commonly missed on X-ray; look for loss of alignment between 2nd metatarsal base and middle cuneiform
Fascia Lata, Retinacula & Dermatomes
Fascia Lata (AN20.3)
- Deep fascia of the thigh — thick fibrous stocking surrounding all thigh muscles
- Thickened laterally as the iliotibial (IT) band/tract — from iliac tubercle to Gerdy's tubercle on tibia
- IT band: Maintains knee extension (with hip abductors), resists valgus stress
- IT band syndrome: Friction over lateral femoral condyle → lateral knee pain in runners
- Encloses the femoral sheath (with femoral artery, vein, and femoral canal containing lymphatics)
Retinacula
- Extensor retinacula at the ankle: superior (above ankle) and inferior (Y-shaped, below ankle) — retain tendons of anterior compartment
- Flexor retinaculum: Medial aspect of ankle — forms the roof of the tarsal tunnel
- Peroneal retinacula: Lateral aspect — retain peroneal tendons
Dermatomes of the Lower Limb
- L1: Inguinal/groin region
- L2, L3: Anterior and medial thigh
- L4: Medial leg, medial foot (great toe side) — 'medial 4'
- L5: Lateral leg, dorsum of foot, great toe (dorsum) — tested by big toe dorsiflexion
- S1: Lateral foot, small toe, heel — tested by plantarflexion/ankle reflex
- S2: Posterior thigh and leg
- S3, S4: Perineum/perianal
Memory: L4 = lateral knee reflex area (patellar reflex tests L4 primarily), S1 = ankle reflex