Page 2 of 8
AN20.1-10 | General Features, Joints, radiographs & surface marking (Lower Limb) — SDL Guide (Part 2)
Venous Drainage & Varicose Veins
Superficial Veins
- Great (Long) Saphenous Vein (GSV): Begins at the medial end of the dorsal venous arch of the foot → passes anterior to medial malleolus → up the medial side of the leg → passes posterior to medial condyle of femur → enters the femoral vein at the saphenous opening (4 cm below and lateral to pubic tubercle) via the cribriform fascia. Contains 12-15 valves.
- Small (Short) Saphenous Vein (SSV): Begins at lateral end of dorsal venous arch → passes posterior to lateral malleolus → up the posterior midline of the leg → pierces deep fascia to enter the popliteal vein.

Figure: Why anatomy matters

Figure: Step 1 (emptying)

Figure: Perforating Veins
Perforating Veins: Connect superficial to deep venous systems. Valves normally allow flow from superficial → deep only.
Varicose Veins (AN20.5)
- Definition: Dilated, tortuous superficial veins due to incompetent valves
- Anatomical basis: Valve incompetence (especially at saphenofemoral junction for GSV, or in perforating veins) → blood refluxes from deep to superficial → increased superficial venous pressure → vessel wall dilation and elongation → tortuous varicosities
- Venous ulcer location: Above medial malleolus (gaiter area) — maximal hydrostatic pressure + poor tissue perfusion from chronic venous hypertension → skin breakdown
- DVT (AN20.5): Virchow's triad — Stasis (prolonged immobility) + Endothelial damage + Hypercoagulability. Soleal sinuses are the primary DVT initiation site. Popliteal and femoral DVT can propagate to iliac veins. Risk of pulmonary embolism.
- Indian context: Prolonged squatting (Asian posture) compresses popliteal veins → DVT risk in susceptible individuals
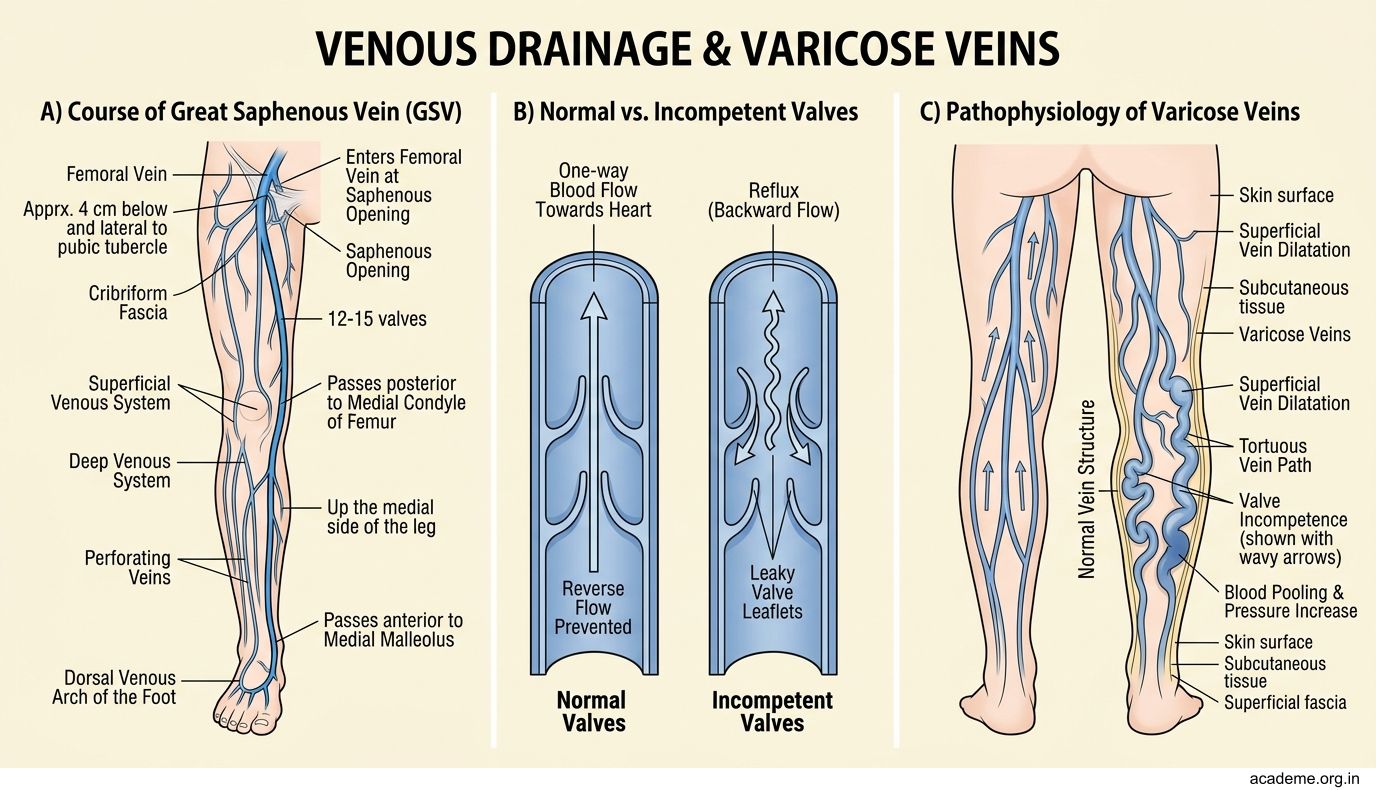
Figure: Perforating Veins
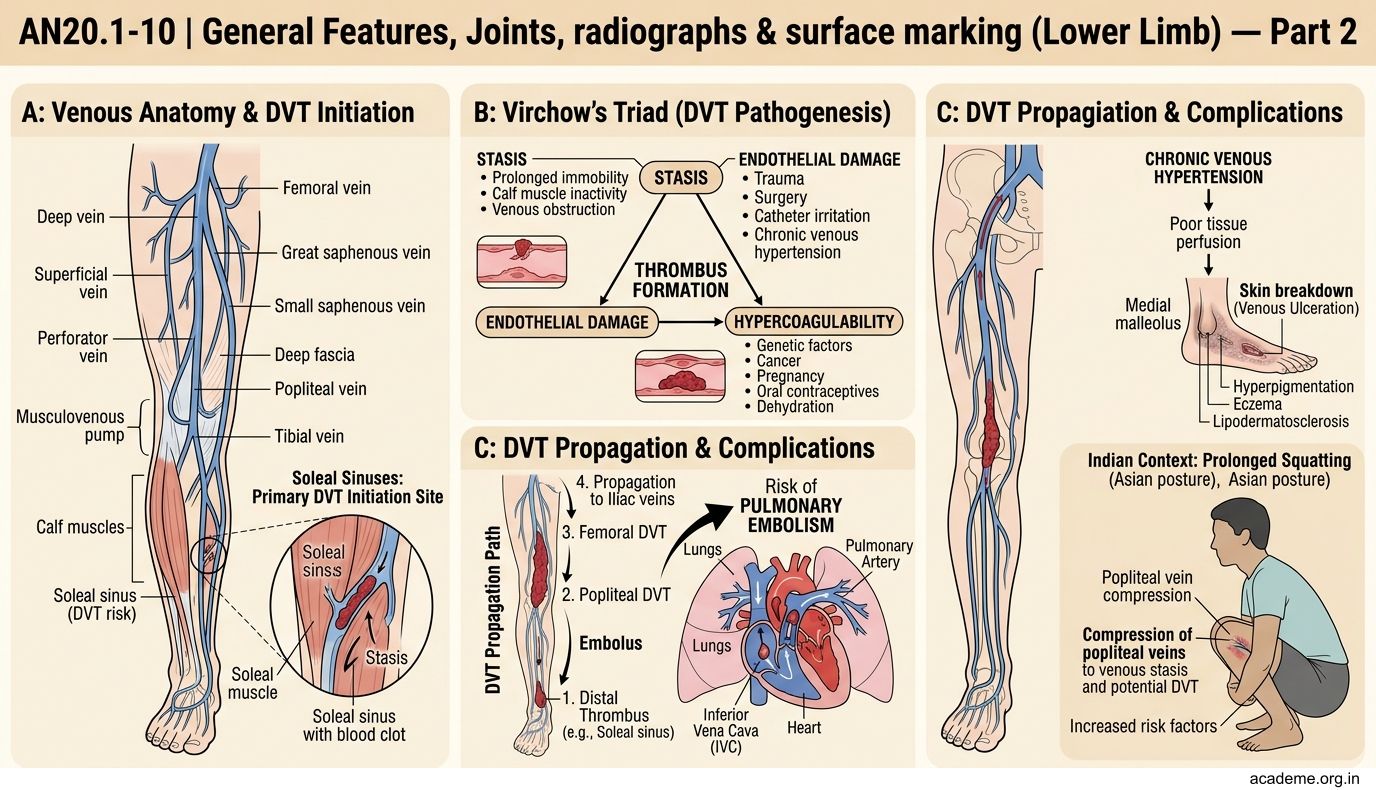
Figure: Step 1 (emptying)
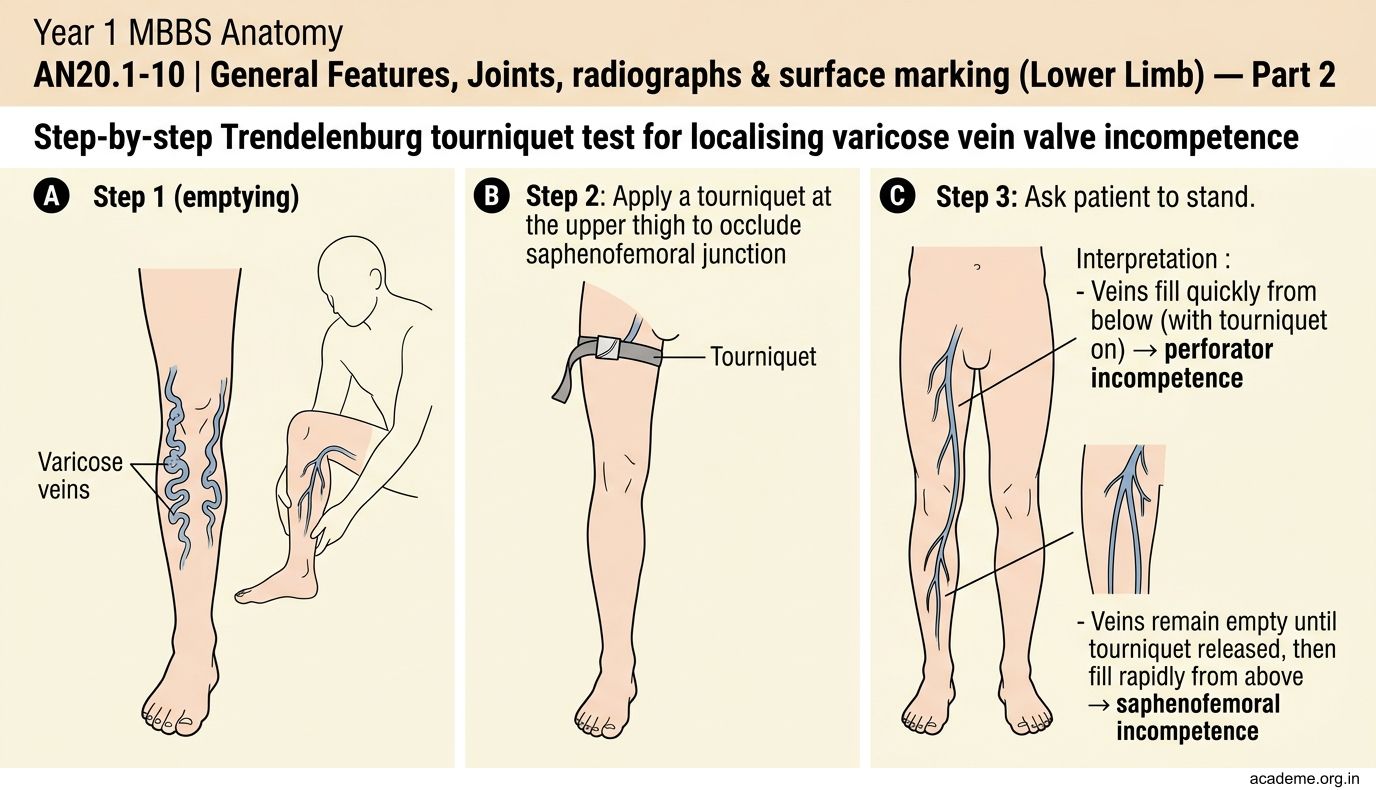
Figure: Why anatomy matters
CLINICAL PEARL
The Trendelenburg test identifies the site of valve incompetence in varicose veins:
Step 1 (emptying): Elevate the leg 45° to empty superficial veins.
Step 2 (tourniquet): Apply a tourniquet at the upper thigh to occlude saphenofemoral junction.
Step 3 (standing): Ask patient to stand.
Interpretation:
- Veins fill quickly from below (with tourniquet on) → perforator incompetence
- Veins remain empty until tourniquet released, then fill rapidly from above → saphenofemoral junction incompetence (the commonest cause)
Why anatomy matters: The test works because we're systematically blocking different levels of valve incompetence. Understanding the anatomy (saphenofemoral junction at saphenous opening, 4 cm below and lateral to pubic tubercle) guides surgical ligation at the correct level.
Lymphatic Drainage & Inguinal Lymphadenopathy
Lymphatic Drainage of the Lower Limb (AN20.3 & AN20.4)

Figure: Deep inguinal nodes
Superficial inguinal nodes (in the femoral triangle):
- Horizontal group: Along the inguinal ligament → drain the lower anterior abdominal wall, perineum, external genitalia, gluteal region, anal canal
- Vertical group: Along the great saphenous vein → drain the entire lower limb superficially
Deep inguinal nodes: Along the femoral vein, medial to it → drain the deep structures of the lower limb and receive efferents from superficial inguinal nodes. Cloquet's node (Rosenmuller's node) = highest deep inguinal node, lies in the femoral canal.
Clinical — Inguinal Lymphadenopathy (AN20.4):
- Infected toe/foot/leg → vertical superficial inguinal nodes
- External genitalia/anal infection → horizontal superficial inguinal nodes
- Scrotal carcinoma → superficial inguinal nodes (NOT external iliac — because scrotum drains to inguinal nodes, NOT para-aortic)
- Testicular carcinoma → para-aortic nodes (because testes develop in abdomen and drain to lumbar/para-aortic nodes, NOT inguinal)
- Penile carcinoma → inguinal nodes
- Metastatic nodes: Hard, non-tender, fixed. Primary can be anywhere in the drainage territory.
Exam trap: Don't confuse scrotal lymphatics (→ inguinal) with testicular lymphatics (→ para-aortic).
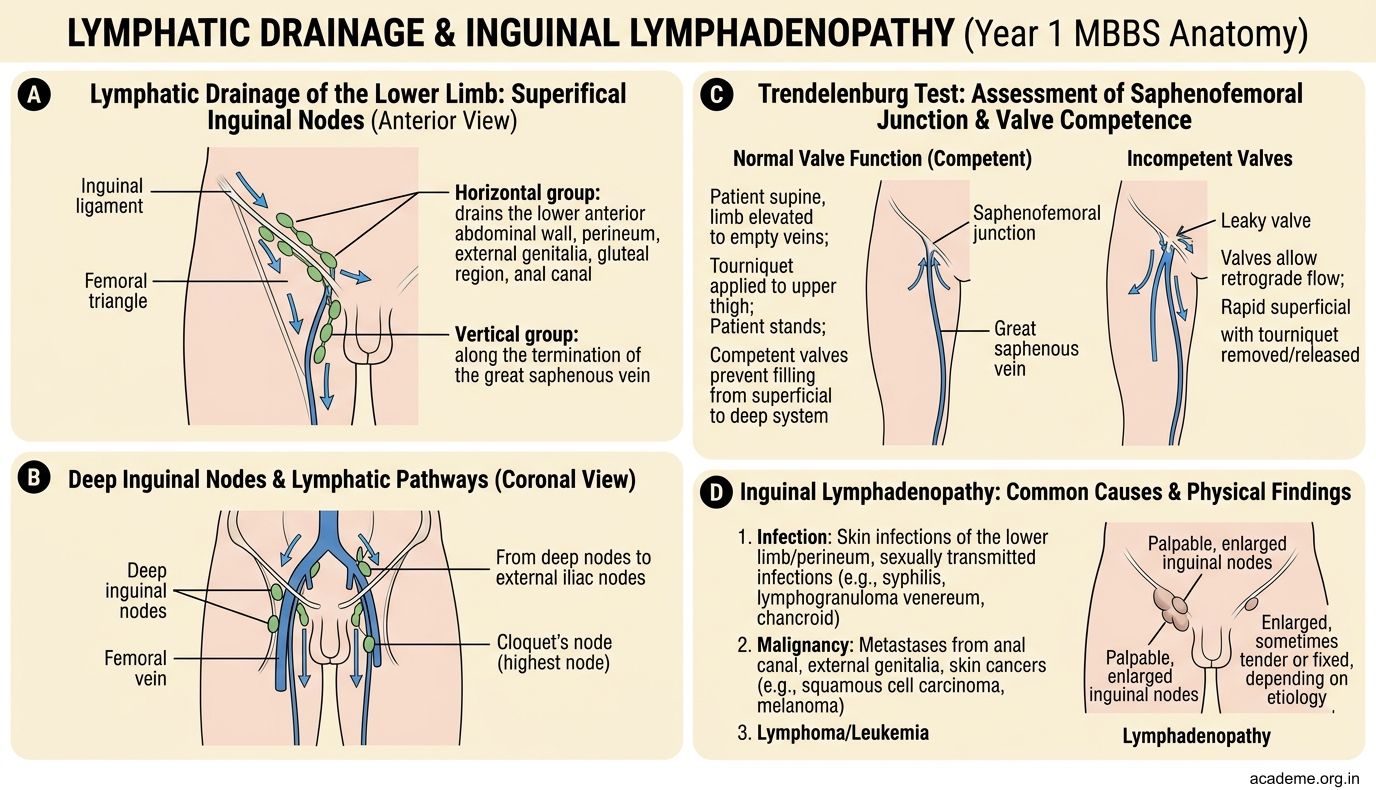
Figure: Deep inguinal nodes
SELF-CHECK — 1
A 24-year-old hockey player sprains his ankle in inversion. Which ligament is MOST likely torn first?
A. Deltoid (medial) ligament
B. Anterior talofibular ligament (ATFL)
C. Calcaneofibular ligament (CFL)
D. Posterior talofibular ligament (PTFL)
Reveal Answer
Answer: B. Anterior talofibular ligament (ATFL)
A patient with a swollen red leg returns from a 12-hour train journey. DVT is suspected. Which venous structure is the primary initiation site for DVT in the lower limb?
A. Great saphenous vein
B. Femoral vein at the saphenous opening
C. Soleal venous sinuses
D. Popliteal vein
Reveal Answer
Answer: C. Soleal venous sinuses
Radiographs of the Lower Limb — What to Identify
AP Radiograph of the Hip (AN20.6)
Identify: Head of femur (spherical, in acetabulum), neck of femur (angle of inclination ~126°), greater trochanter, lesser trochanter (on posteromedial aspect, visible on AP), intertrochanteric line/crest, femoral shaft.
Shenton's line: Smooth arc from inferior border of superior pubic ramus to inferior border of femoral neck — disrupted in fracture/dislocation of hip.
Neck-shaft angle: Normal ~126° (coxa vara <120°, coxa valga >135°)

Figure: Key measurements
AP Radiograph of the Knee
Identify: Medial and lateral femoral condyles, medial and lateral tibial condyles (plateaux), tibial spine (intercondylar eminence), head of fibula, joint space (medial 3-4mm, lateral 3-4mm), patella (on AP partially superimposed), fabella (sesamoid in gastrocnemius — normal variant).
AP + Lateral Radiograph of the Ankle
Identify on AP: Tibial plafond, medial malleolus, lateral malleolus (fibula tip), talar trochlea (dome), ankle mortise (uniform 3mm joint space all around — asymmetry indicates instability or fracture).
Identify on Lateral: Tibia, fibula (superimposed posteriorly), talus, calcaneus, navicular, cuboid, 5th metatarsal base (avulsion fracture site — do not confuse with accessory ossicle).
AP Radiograph of the Foot
Identify: All five metatarsals, phalanges (proximal, middle, distal), tarsals (medial, intermediate, lateral cuneiforms; navicular; cuboid). Check Lisfranc alignment: medial border of 2nd metatarsal should align with medial border of middle cuneiform.
Key measurements:
- Bohler's angle (on lateral calcaneus X-ray): Normal 20-40°. Reduced in calcaneal fractures (falls from height).
- Hilgenreiner's line (hip): horizontal through both triradiate cartilages — used for DDH assessment in infants.

Figure: Radiographs of the Lower Limb — What to Identify
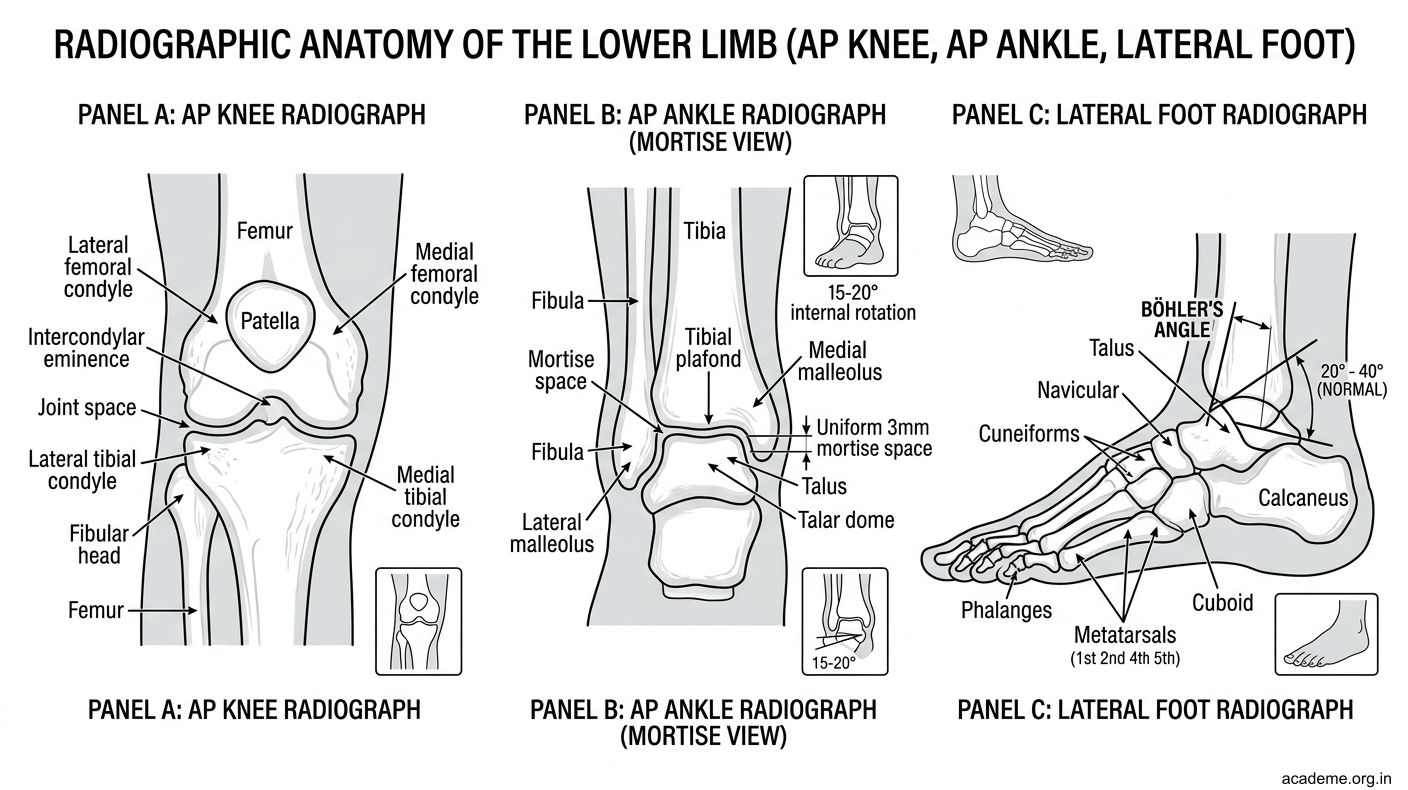
Figure: Radiographs of the Lower Limb — What to Identify
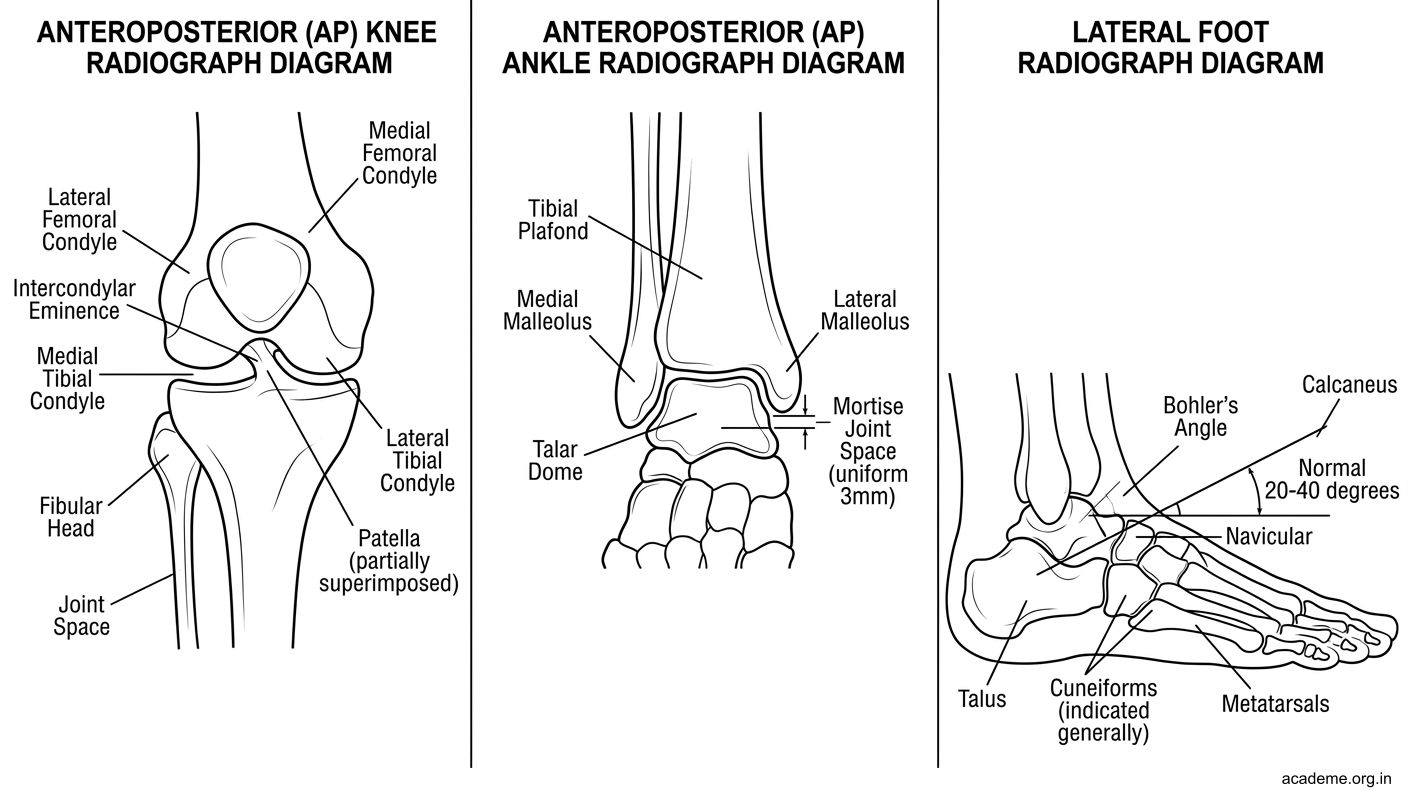
Figure: Radiographs of the Lower Limb — What to Identify
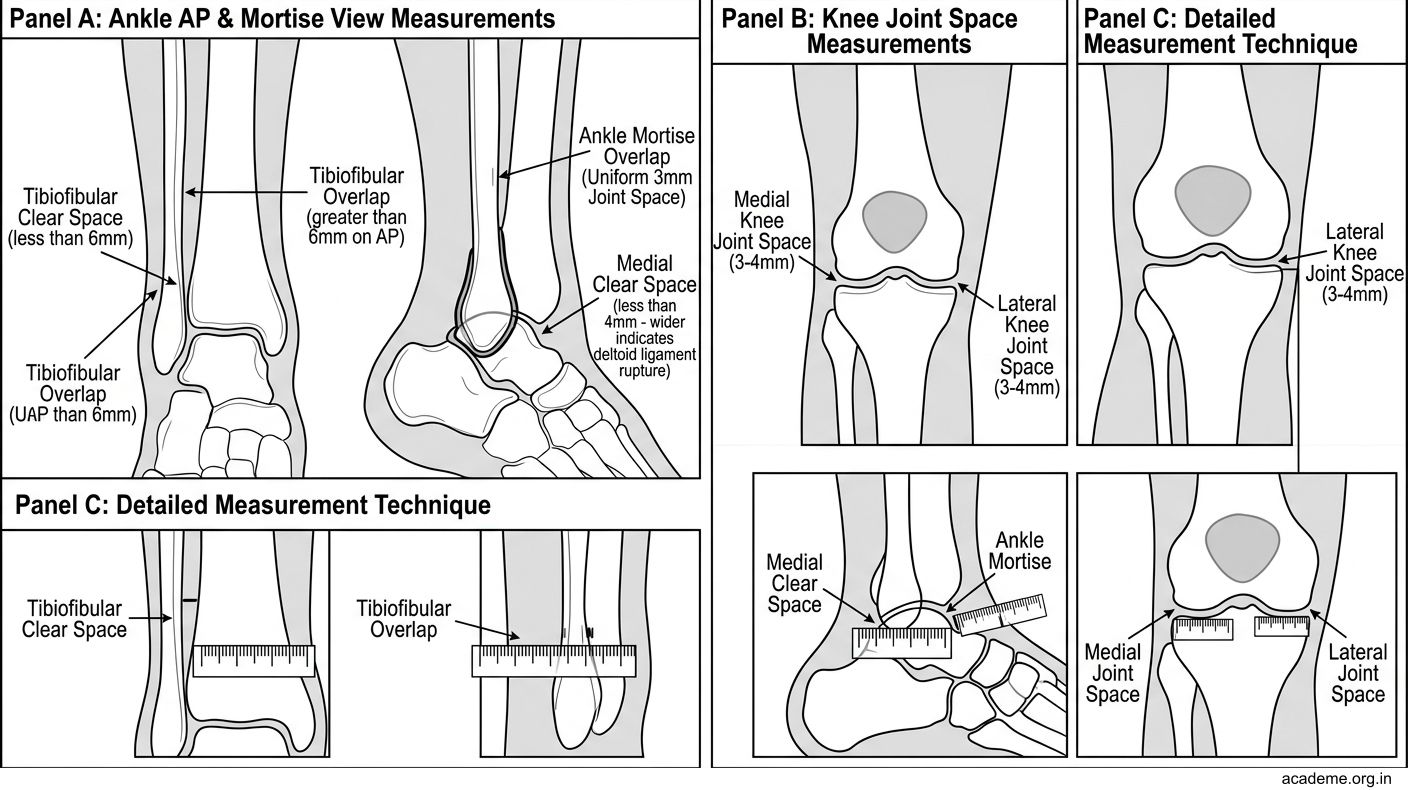
Figure: Key measurements