Page 1 of 6
AN52.1-8 | Histology & Embryology (Abdomen & Pelvis) — SDL Guide
Learning Objectives
- Identify the microanatomical features of the GIT (oesophagus to large intestine), liver, gallbladder, pancreas, and suprarenal gland (AN52.1)
- Identify the microanatomical features of the urinary system (kidney, ureter, bladder), male and female reproductive systems (AN52.2)
- Identify the microanatomical features of the cardio-oesophageal junction and corpus luteum (AN52.3)
- Describe the development of the anterior abdominal wall (AN52.4)
- Describe the development and congenital anomalies of the diaphragm (AN52.5)
- Describe the development and congenital anomalies of the foregut, midgut, and hindgut (AN52.6)
- Describe the development of the urinary system (AN52.7)
- Describe the development of the male and female reproductive systems (AN52.8)
INSTRUCTIONS
Read each section carefully. This module integrates the microanatomy (histology) of the GIT, liver, urinary, and reproductive systems with the embryological basis of common congenital anomalies. Histology is pattern recognition — build a mental image of each organ's layers and special cells. Embryology explains clinical conditions from malrotation to hypospadias.
References
- Inderbir Singh's Textbook of Human Histology (7th ed.) (Textbook)
- Sadler's Langman's Medical Embryology (14th ed.) (Textbook)
- Gray's Anatomy for Students — Histology and Embryology sections (Textbook)
- OpenStax Anatomy and Physiology 2e — Digestive and Reproductive Systems (Open Access)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A newborn is brought to the neonatal unit in JIPMER with bilious vomiting from the first day of life. Abdominal X-ray shows a "double-bubble sign." Immediately, the attending paediatrician suspects a surgical emergency.
What embryological event failed? At what stage of gut development does the duodenum normally become a solid cord — and when does it recanalise? Why is bilious vomiting (green vomit) a sign of obstruction below the ampulla of Vater? What other midgut anomalies follow a related embryological error?
Embryology and histology are not just academic exercises — they explain the pathophysiology of congenital anomalies encountered daily in paediatric surgery, neonatology, and adult gastroenterology in India.
WHY THIS MATTERS
Why histology and embryology of the abdomen and pelvis matter in Indian clinical practice:
- Congenital anomalies of the GIT: Hirschsprung's disease, malrotation, duodenal atresia, oesophageal atresia — present in neonatal ICUs across India; incidence is not declining
- Liver histology: basis for interpreting liver biopsies in viral hepatitis (B and C — India has among the highest global burdens), alcoholic liver disease, NAFLD, and cirrhosis
- Renal histology: basis for understanding glomerulonephritis patterns (IgA nephropathy is the most common glomerulonephritis in India — seen in young males with haematuria)
- Congenital diaphragmatic hernia (CDH): causes respiratory failure at birth; detected on antenatal ultrasound in MGMCRI OG clinics
- Developmental anomalies of the urogenital system: horseshoe kidney, hypospadias, undescended testis — common in Indian paediatric surgical units
- Testicular histology: histological basis of azoospermia evaluation (Sertoli-cell-only syndrome vs maturation arrest) — important for infertility clinics
RECALL
Before we begin, recall:
- The GIT wall has a universal 4-layer structure: mucosa (epithelium + lamina propria + muscularis mucosae), submucosa, muscularis externa (circular + longitudinal), serosa/adventitia
- The gut tube is derived from endoderm (epithelium); the surrounding connective tissue and muscle is from splanchnic mesoderm
- The liver and pancreas are endodermal outgrowths of the foregut
- The kidney develops from intermediate mesoderm in three successive waves: pronephros → mesonephros → metanephros
- Sexual differentiation: gonads are initially indifferent (both Wolffian and Müllerian ducts present); testosterone → male (Wolffian persists); absence of testosterone → female (Müllerian persists)
GIT Histology — Recognisable Features by Segment (AN52.1)
Oesophagus:
- Epithelium: stratified squamous non-keratinised
- No villi, no crypts; has mucous glands in the submucosa (oesophageal glands proper)
- Muscularis externa: upper 1/3 = skeletal; middle 1/3 = mixed; lower 1/3 = smooth muscle
- No serosa — adventitia only (facilitates surgical approach but worsens anastomotic leaks)
Stomach — fundus vs pylorus:
| Feature | Fundus/Body | Pylorus |
|---|---|---|
| Glands | Gastric glands (straight, long) | Pyloric glands (coiled, short, mucous) |
| Key cells | Parietal cells (HCl + intrinsic factor), chief cells (pepsinogen), mucous neck cells | Mucous cells, G-cells (gastrin) |
| Surface | Gastric pits (shallow in fundus, deep in pylorus) |
Duodenum, Jejunum, Ileum — distinguishing features:
| Feature | Duodenum | Jejunum | Ileum |
|---|---|---|---|
| Villi | Broad, leaf-like | Tall, finger-like | Shorter, finger-like |
| Goblet cells | Fewer | Moderate | Many |
| Crypts of Lieberkühn | Present | Present | Present |
| Brunner's glands (submucosal, alkaline secretion — neutralise acid chyme) | Yes | No | No |
| Peyer's patches (lymphoid nodules in submucosa) | No | No | Yes |
Large intestine:
- No villi — only crypts (abundant goblet cells)
- Teniae coli (3 bands of longitudinal muscle — gather into haustrations)
- Appendix: many lymphoid follicles in the submucosa ('lymphoid organ of the gut')
Liver histology:
- Hepatic lobule (classical): central vein at centre; portal triads (portal vein + hepatic artery + bile duct) at periphery
- Hepatic plates: single-cell-thick plates of hepatocytes radiating from central vein
- Sinusoids: between hepatic plates; lined by Kupffer cells (resident macrophages), stellate cells (Ito cells — store vitamin A; activated in fibrosis)
- Portal acinus (functional unit): zone 1 (periportal — best O2, first affected in hepatitis), zone 3 (centrilobular — worst O2, affected in congestion/ischaemia)
- Space of Disse: between hepatocytes and sinusoidal endothelium — site of lymph formation
Pancreas:
- Exocrine (90%): acinar cells (zymogen granules at apex), ducts (centoacinar cells)
- Endocrine (islets of Langerhans): α-cells (glucagon), β-cells (insulin — most numerous), δ-cells (somatostatin)
Suprarenal (adrenal) gland:
- Cortex (mesodermal): zona glomerulosa (aldosterone), zona fasciculata (cortisol), zona reticularis (androgens) — "GFR = salt, sugar, sex"
- Medulla (neural crest): chromaffin cells (adrenaline + noradrenaline)

Figure: GIT Histology — Recognisable Features by Segment (AN52.1)

Figure: Duodenum, Jejunum, Ileum — distinguishing features:

Figure: Stomach — fundus vs pylorus:
Urinary and Reproductive Histology (AN52.2, AN52.3)
Kidney:
- Cortex: glomeruli + proximal and distal convoluted tubules + macula densa
- Medulla: loops of Henle + collecting ducts
- Glomerulus: capillary tuft within Bowman's capsule; basement membrane + podocytes (filtration barrier)
- Proximal tubule: simple cuboidal epithelium with dense brush border (microvilli) — most reabsorption occurs here
- Juxtaglomerular apparatus: macula densa (modified DCT cells, sense NaCl) + JG cells (renin secretion) + mesangium
Ureter: Transitional epithelium (urothelium), 2-layer muscularis in upper 2/3, 3-layer in lower 1/3.
Testis:
- Seminiferous tubules: Sertoli cells (supporting, blood-testis barrier) + spermatogenic cells (at different stages)
- Interstitium: Leydig cells (testosterone production)
- Clinical: Sertoli-cell-only syndrome = Leydig cells present but no spermatogenic cells → azoospermia
Ovary:
- Germinal epithelium (simple cuboidal/columnar), tunica albuginea (fibrous)
- Follicles: primordial → primary → secondary → Graafian follicle (antrum, cumulus oophorus, corona radiata)
- Corpus luteum: post-ovulation structure; granulosa cells → large luteal cells (progesterone); theca interna → small luteal cells (oestrogen) — appears as yellow, folded structure with large pale cells on histology (AN52.3)
- Corpus albicans: regressed corpus luteum → white fibrous scar
Cardio-oesophageal junction (AN52.3):
- Abrupt transition: stratified squamous epithelium (oesophagus) → simple columnar mucus-secreting epithelium (stomach)
- This junction is the site of Barrett's oesophagus (columnar metaplasia extends into the oesophagus from GORD)
- Histologically the Z-line (ora serrata): irregular, visible endoscopically as a pale-pink/salmon-coloured zone
Uterus:
- Endometrium: functional layer (shed each cycle) + basal layer; simple columnar epithelium; glands under hormonal control
- Myometrium: thick smooth muscle
- Perimetrium: serosa (peritoneum)

Figure: Urinary and Reproductive Histology (AN52.2, AN52.3)
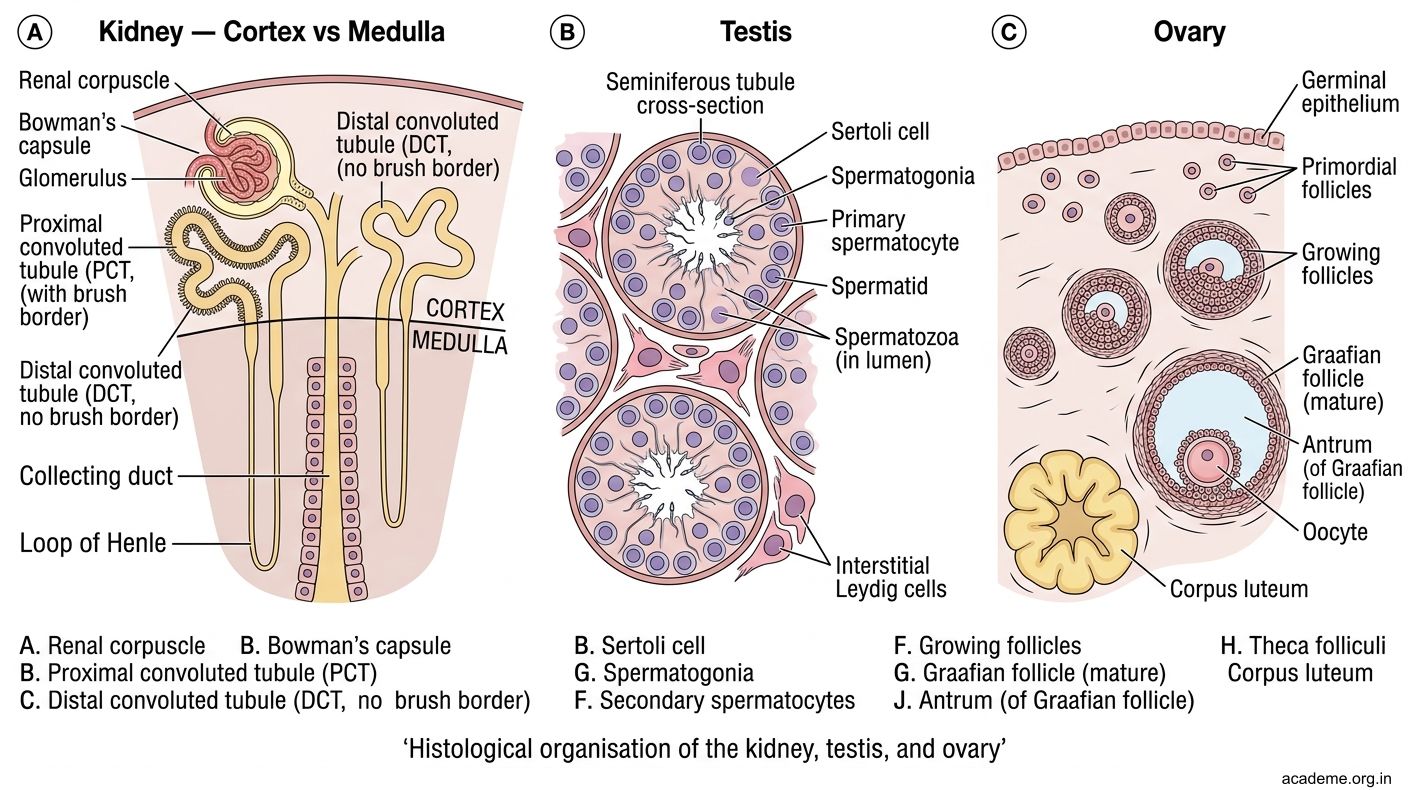
Figure: Urinary and Reproductive Histology (AN52.2, AN52.3)
Development of the Diaphragm and Congenital Diaphragmatic Hernia (AN52.5)
Diaphragm develops from 4 sources:
1. Septum transversum (central tendon — main contribution)
2. Pleuroperitoneal membranes (close the pleuroperitoneal canals)
3. Dorsal mesentery of oesophagus (crura and central part)
4. Body wall muscle (peripheral muscular part — myoblasts from cervical somites C3–C5)
Congenital Diaphragmatic Hernia (CDH):
- Failure of the pleuroperitoneal membrane to close → herniation of abdominal organs into the thorax
- Bochdalek hernia (most common, 90%): left postero-lateral defect (foramen of Bochdalek); left-sided in 85% (stomach + small bowel + spleen herniate into left chest)
- Morgagni hernia (rare, 2%): anterior defect (between costal and sternal origins of diaphragm); right-sided; contains transverse colon or omentum
Clinical presentation of Bochdalek hernia:
- Severe respiratory distress at birth (lungs compressed during development → pulmonary hypoplasia)
- Abdomen is scaphoid (contents in chest)
- Breath sounds absent on left; heart sounds shifted right
- CXR: bowel loops in left hemithorax, mediastinal shift
- Treatment: surgical repair (ECMO may be required for severe pulmonary hypertension)

Figure: Development of the Diaphragm and Congenital Diaphragmatic Hernia (AN52.5)
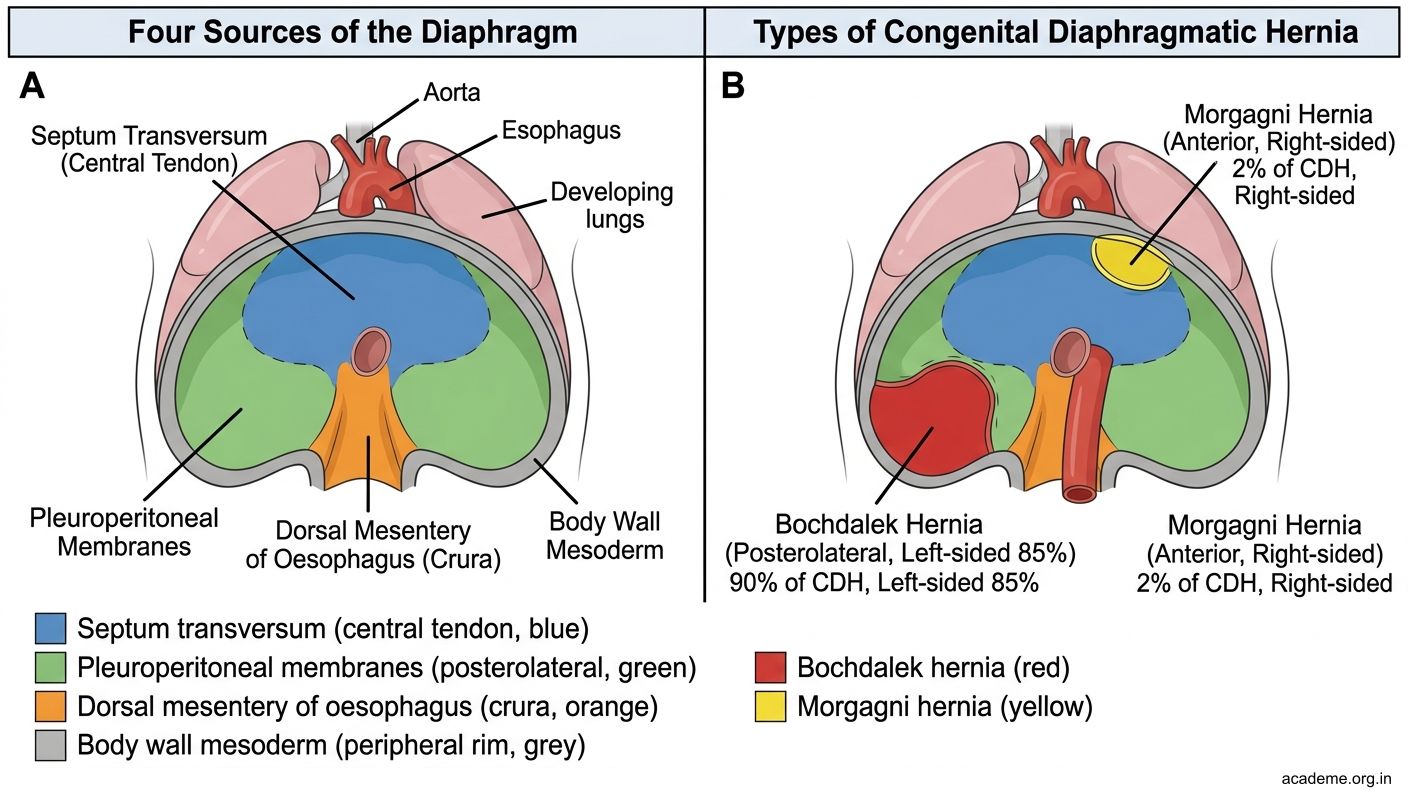
Figure: Development of the Diaphragm and Congenital Diaphragmatic Hernia (AN52.5)