Page 1 of 4
AN55.1-2 | Surface marking — SDL Guide
Learning Objectives
- Demonstrate and describe the surface marking of regions and planes of the abdomen, superficial inguinal ring, deep inguinal ring, McBurney's point, renal angle, and Murphy's point (AN55.1)
- Demonstrate the surface projections of the stomach, liver, fundus of gall bladder, spleen, duodenum, pancreas, ileocaecal junction, kidneys, and root of mesentery (AN55.2)
INSTRUCTIONS
Read each section in order. Bold terms (like this) are key vocabulary. Attempt the self-check questions before revealing answers. Use your own abdomen to locate each surface marking as you read.
References
- BD Chaurasia's Human Anatomy — Surface Anatomy chapter (Textbook)
- Gray's Anatomy for Students — Abdomen surface anatomy (Textbook)
- NMC UG CBUC 2024, Competencies AN55.1–AN55.2 (Curriculum)
Version 1.0 | Academe Content Engine v2
CLINICAL SCENARIO
You are the intern on call. A 24-year-old engineering student from IIT Madras arrives in the casualty at 10 PM with pain that started at the umbilicus and has now shifted to the right lower abdomen. You press at a specific point on his abdomen — two-thirds of the way from the umbilicus to the right anterior superior iliac spine — and he winces in pain.
That point is McBurney's point. You've just localised his appendix.
Surface marking is not a memory exercise — it is the foundation of every clinical examination you will ever perform.
WHY THIS MATTERS
Surface marking of abdominal organs allows you to:
• Localise pain — right iliac fossa pain → appendix; right hypochondrium → gallbladder
• Perform clinical examination — percussion over liver/spleen boundaries
• Interpret imaging — know where to look on X-ray or ultrasound
• Guide clinical procedures — needle placement for paracentesis, renal biopsy, nerve blocks
The NMC CBUC 2024 requires you to demonstrate (not just describe) these surface markings (AN55.1–AN55.2). You will be examined clinically on a live patient or mannequin.
RECALL
From your earlier study, you know:
• The abdomen is divided into 9 regions by two horizontal (subcostal, transtubercular) and two vertical (midclavicular) planes
• Or 4 quadrants by the median sagittal plane and the transumbilical plane
• The transpyloric plane (L1) passes through the pylorus and the 9th costal cartilage tips
• The inguinal canal runs from the deep inguinal ring to the superficial inguinal ring
In this module we translate that internal anatomy to external surface landmarks.
Abdominal Regions, Planes, and Reference Points
Nine-region system — two horizontal planes + two vertical (midclavicular) planes:

Figure: Abdominal Regions, Planes, and Reference Points
Horizontal planes:
1. Subcostal plane — through the lowest point of the costal margin (10th costal cartilage) — at L3 vertebral level. Separates epigastrium from umbilical region.
2. Transtubercular (intertubercular) plane — through the iliac tubercles (5 cm posterior to ASIS on iliac crest) — at L5 vertebral level. Separates umbilical from hypogastric/pubic region.
Vertical planes: Two midclavicular lines — through midpoints of the clavicles, passing medial to the nipple and ASIS.
Nine regions (right to left, top to bottom):
• Row 1: Right hypochondrium | Epigastrium | Left hypochondrium
• Row 2: Right lumbar (flank) | Umbilical | Left lumbar (flank)
• Row 3: Right iliac fossa | Hypogastric (pubic) | Left iliac fossa
Four-quadrant system: Simpler — right upper quadrant (RUQ), left upper quadrant (LUQ), right lower quadrant (RLQ), left lower quadrant (LLQ). Formed by the transumbilical plane (L3–L4) and the median plane.
The Transpyloric Plane (Addison's) — L1:
Halfway between jugular notch and pubic symphysis. Passes through:
• Pylorus of stomach, 1st part of duodenum
• Hilum of left kidney (right kidney hilum slightly lower)
• Origin of superior mesenteric artery (SMA)
• Neck of pancreas
• Duodenojejunal flexure
• Fundus of gall bladder tip (when distended)
• 9th costal cartilage tips
• Termination of spinal cord (conus medullaris, L1–L2)
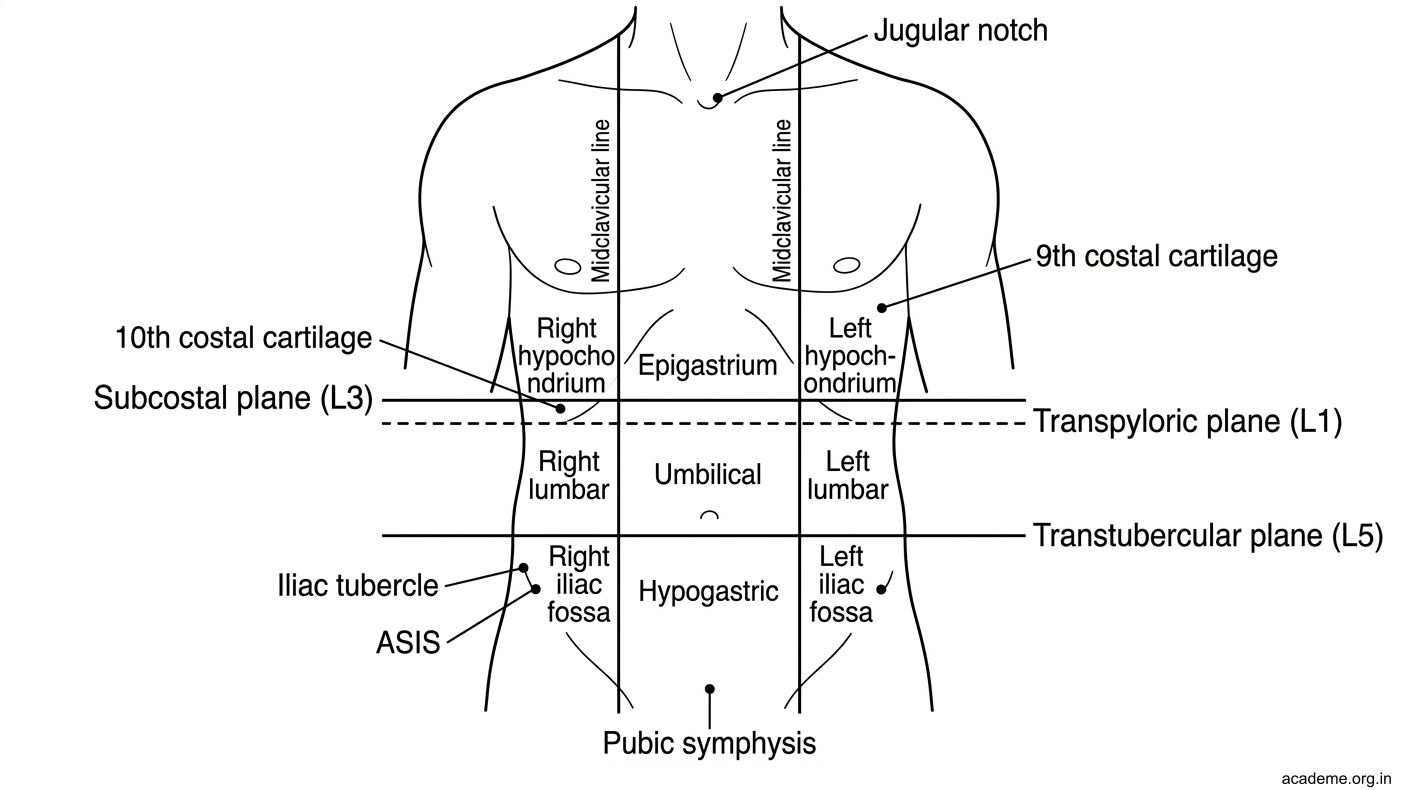
Figure: Abdominal Regions, Planes, and Reference Points
Key Surface Points: Inguinal Rings, McBurney's, Renal Angle, Murphy's
Superficial Inguinal Ring:
A triangular gap in the external oblique aponeurosis, 1 cm superior and lateral to the pubic tubercle. Feel the pubic tubercle (prominence at the medial end of inguinal ligament) → move 1 cm up and out. Transmits: spermatic cord (males), round ligament (females). Site of direct/indirect inguinal hernia emergence.
Deep Inguinal Ring:
1.5 cm above the midpoint of the inguinal ligament (midpoint of inguinal ligament = halfway between ASIS and pubic tubercle). It is an opening in the transversalis fascia. The inferior epigastric vessels are medial to the ring — used to distinguish indirect (lateral to vessels = through deep ring) from direct hernias (medial to vessels).
McBurney's Point:
The surface projection of the appendix base (where it joins the caecum at the ileocaecal junction area). Located at the junction of the lateral one-third and medial two-thirds of the line from the right ASIS to the umbilicus.
Formula: 1/3 from ASIS → umbilicus = McBurney's point.
Tenderness at McBurney's point in right iliac fossa pain = McBurney's sign (acute appendicitis).
Rebound tenderness at McBurney's point = Blumberg's sign.
Renal Angle (Costovertebral Angle):
The angle between the 12th rib and the lateral border of the erector spinae (sacrospinalis) muscle at the back. The kidney lies deep to this angle. Tenderness on firm percussion in the renal angle indicates renal pathology (pyelonephritis, perinephric abscess, renal colic with ureteric stone at PUJ). Also called Murphy's kidney punch sign (though Murphy's sign classically refers to gallbladder — see below).
Murphy's Point (Gallbladder):
Intersection of the right midclavicular line with the right costal margin (approximately 9th costal cartilage level). The fundus of the gall bladder lies at this point.
Murphy's sign = place hand at Murphy's point and ask patient to inhale deeply → pain/inspiratory arrest as the inflamed gall bladder descends to meet the examining hand = acute cholecystitis.
SELF-CHECK
You are examining a patient with right iliac fossa pain. You locate the right ASIS and the umbilicus. Where exactly is McBurney's point?
A. Halfway between ASIS and umbilicus
B. One-third of the way from the right ASIS to the umbilicus (lateral 1/3)
C. One-third of the way from the umbilicus to the right ASIS (lateral 1/3 from ASIS = medial 2/3 from umbilicus)
D. Directly below the umbilicus on the right side
Reveal Answer
Answer: C. One-third of the way from the umbilicus to the right ASIS (lateral 1/3 from ASIS = medial 2/3 from umbilicus)
McBurney's point = junction of the lateral 1/3 and medial 2/3 of the line from the right ASIS to the umbilicus. In other words, starting from the ASIS, go 1/3 of the way toward the umbilicus. Starting from the umbilicus, go 2/3 of the way toward the ASIS. This is the surface marking of the base of the appendix.
Surface Projections: Liver, Gall Bladder, Stomach, Spleen
Liver:
• Upper border: Right midclavicular line at 5th intercostal space (5th rib) — right side, slightly lower on left.
• Lower border: Right costal margin (right midclavicular line). Normally the lower border is just palpable at/below the right costal margin on deep inspiration.
• In children: liver normally extends 1–2 cm below the costal margin (normal variant).
• Clinically: Hepatomegaly = liver palpable >2 cm below costal margin in adults. Percussion dullness from 5th rib to costal margin.

Figure: Surface Projections: Liver, Gall Bladder, Stomach, Spleen
Fundus of Gall Bladder:
• Junction of the right midclavicular line with the right costal margin (approximately level of 9th costal cartilage / Murphy's point).
• When distended (hydrops, empyema) → may be palpable as a smooth, ovoid mass below the liver.
• Courvoisier's sign: Palpable, non-tender, distended gall bladder + jaundice → malignant biliary obstruction (NOT gallstones, because gallstones cause fibrosis/small gallbladder).
Stomach:
• Cardiac orifice: behind left 7th costal cartilage, 2.5 cm from midline at the level of T10/T11.
• Pylorus: transpyloric plane (L1), 2.5 cm to the right of the midline.
• Greater curvature: roughly from left 5th intercostal space (fundus) to the right, curving downward.
• Gastric area: left hypochondrium + epigastrium.
• Surface: fundus is under the left dome of the diaphragm → left 5th–9th rib area.
Spleen:
• Surface projection: 9th, 10th, 11th ribs in the left posterior axillary line.
• Long axis of spleen corresponds to the 10th rib.
• Lies in the left hypochondrium, posterior, separated from 9th–11th ribs by the diaphragm.
• Not normally palpable (must enlarge to >2× normal size before becoming palpable across the costal margin).
• Splenomegaly: Palpable below the left costal margin, moving toward right iliac fossa.
• Tip of spleen is level with the anterior end of the 10th intercostal space (above the 10th rib).

Figure: Surface Projections: Liver, Gall Bladder, Stomach, Spleen
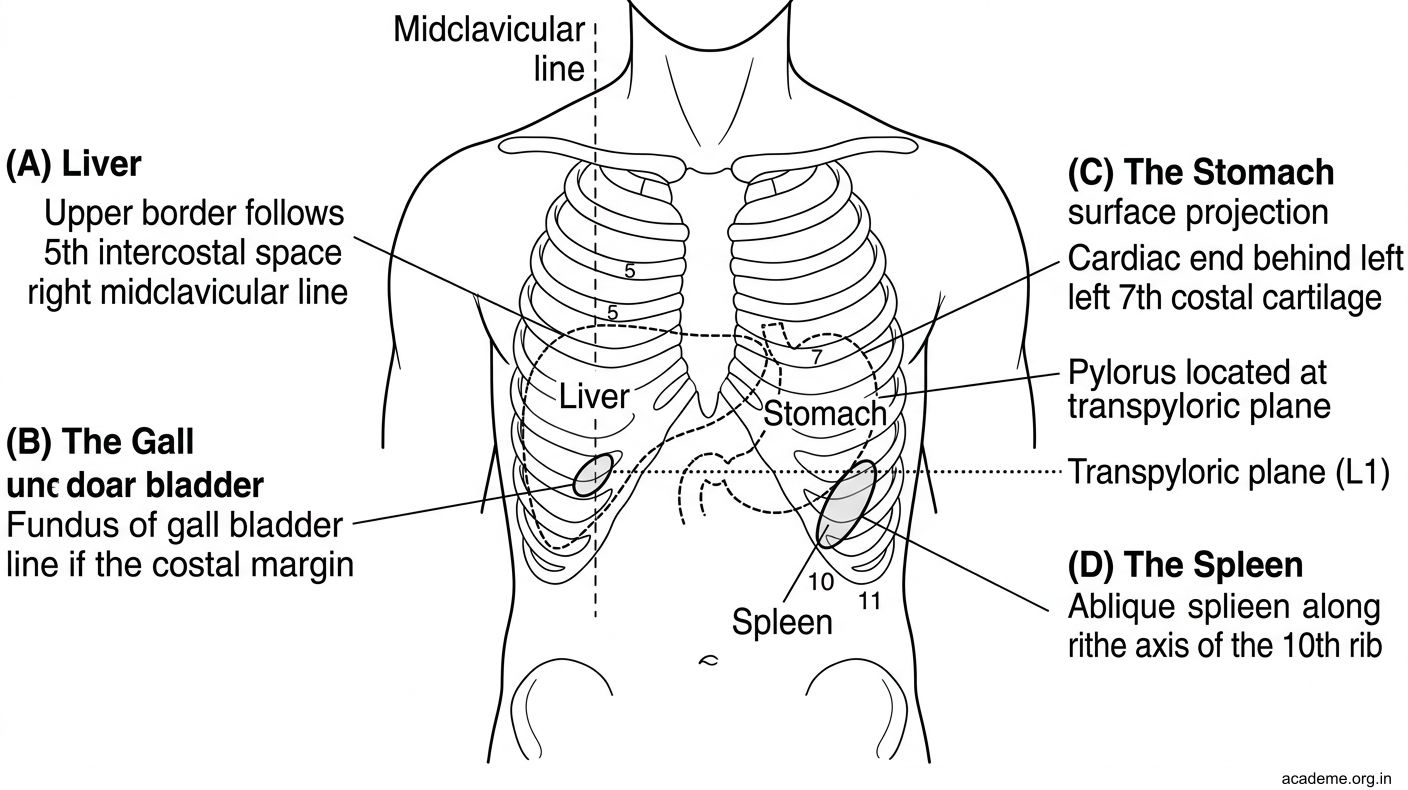
Figure: Surface Projections: Liver, Gall Bladder, Stomach, Spleen
Surface Projections: Kidneys, Duodenum, Pancreas, Ileocaecal Junction, Mesentery
Kidneys:
• Right kidney: upper pole T12, lower pole L3. The right kidney is slightly lower than the left (displaced by the liver).
• Left kidney: upper pole T11–T12, lower pole L2–L3.
• Hilum of left kidney at transpyloric plane (L1); right hilum at L1–L2.
• Surface (posterior): From 12th rib (medial portion), down to just above iliac crest. Partially covered by 11th and 12th ribs posteriorly.
• Anterior surface: Upper pole covered by rib ends; lower pole is in the lumbar region.

Figure: Surface Projections: Kidneys, Duodenum, Pancreas, Ileocaecal Junction, Mesentery
Duodenum:
• 1st part (superior): transpyloric plane (L1), 2.5 cm right of midline → curves downward.
• 2nd part (descending): right side, L1–L3, alongside the head of pancreas.
• 3rd part (horizontal): L3, crosses midline.
• 4th part (ascending): L2, at the duodenojejunal flexure = transpyloric plane, 2.5 cm left of midline.
Pancreas:
• Head: Right of midline, in the curve of the duodenum (C-loop), at L2.
• Neck: Transpyloric plane (L1), overlies the portal vein formation (SMV + splenic vein).
• Body: Crosses the midline, at L1–L2.
• Tail: Reaches the hilum of the spleen, in the lienorenal ligament.
• Surface projection: obliquely, from right iliac fossa diagonal to left hypochondrium (roughly at L1).
Ileocaecal Junction:
• McBurney's point area — right iliac fossa, medial 2/3 of ASIS–umbilicus line.
• More precisely, the ileocaecal valve is at the junction of the terminal ileum and caecum, in the right iliac fossa.
Root of Mesentery:
• Runs from the duodenojejunal flexure (L2, left of midline) obliquely downward to the right to the right sacroiliac joint.
• Length approximately 15 cm.
• This oblique line (left → right, upward → downward) demarcates the posterior attachment of the small intestinal mesentery.

Figure: Surface Projections: Kidneys, Duodenum, Pancreas, Ileocaecal Junction, Mesentery
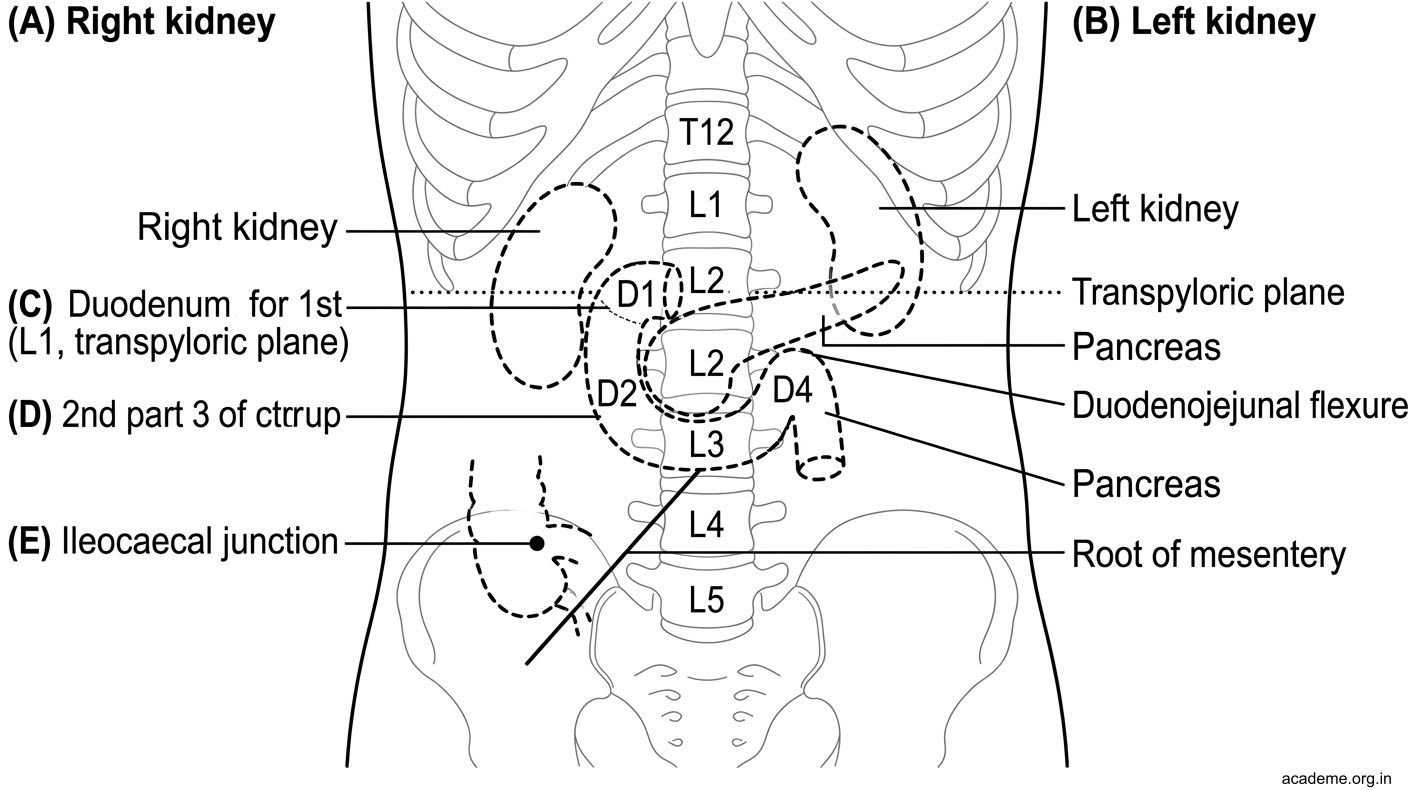
Figure: Surface Projections: Kidneys, Duodenum, Pancreas, Ileocaecal Junction, Mesentery

Figure: AN55 Surface Marking — Key Points:
SELF-CHECK
During examination, you percuss for the upper border of the liver in the right midclavicular line. At which intercostal space do you expect to find the upper border of liver dullness?
A. 2nd intercostal space
B. 4th intercostal space
C. 5th intercostal space
D. 7th intercostal space
Reveal Answer
Answer: C. 5th intercostal space
The upper border of the liver in the right midclavicular line is at the 5th intercostal space (5th rib). Above this, there is lung resonance. Below this, there is liver dullness down to the right costal margin. This defines the normal liver span (approximately 6–12 cm in the MCL by percussion).
SELF-CHECK
A patient has jaundice and a palpable, non-tender, smooth gall bladder. According to Courvoisier's law, this most likely indicates:
A. Acute cholecystitis due to gallstones
B. Malignant obstruction of the common bile duct (e.g., carcinoma of the head of pancreas)
C. Viral hepatitis causing intrahepatic cholestasis
D. Mirizzi syndrome (stone in cystic duct compressing CBD)
Reveal Answer
Answer: B. Malignant obstruction of the common bile duct (e.g., carcinoma of the head of pancreas)
Courvoisier's law: a palpable, non-tender, distended gall bladder in the presence of jaundice is unlikely to be due to gallstones (which cause fibrosis and a shrunken, non-distensible gall bladder). It suggests malignant obstruction distal to the cystic duct — most commonly carcinoma of the head of the pancreas, cholangiocarcinoma, or periampullary carcinoma. This is a classic surgical signs question.
CLINICAL PEARL
Lanz Point vs McBurney's Point:
Both are used to localise the appendix. McBurney's point is the classic landmark (1/3 from right ASIS toward umbilicus). Lanz's point is the junction of the right 1/3 and middle 1/3 of the line between the two ASIS (anterior superior iliac spines) — another appendix surface marking. In clinical practice, McBurney's is used more widely.
Spleen vs Left Kidney on examination:
Both are in the left hypochondrium. Key differences: Spleen has a notch on its medial border, moves downward-right on inspiration, is dull to percussion, and you cannot "get above" it (extends to ribs 9–11). The kidney moves vertically on respiration, has a resonant percussion note (gas-filled bowel in front), is in the loin (more posterior/lateral), and is ballottable. Surface marking helps: spleen = 9th–11th rib area; kidney = T12–L3 (more inferior and posterior).
REFLECT
You are about to examine a patient with abdominal pain in the outpatient clinic. Without touching the patient, describe how you would use surface landmarks alone to hypothesise which organ is the source of pain in: (1) right hypochondriac pain, (2) right iliac fossa pain, (3) central lower abdominal pain, (4) left flank pain. What surface markings would you check on examination?
KEY TAKEAWAYS
AN55 Surface Marking — Key Points:
Planes and Regions (AN55.1):
• Subcostal plane (L3) + transtubercular plane (L5) + 2 midclavicular lines = 9 regions
• Transumbilical plane (L3–L4) + median plane = 4 quadrants
Key Points (AN55.1):
• Superficial inguinal ring: 1 cm above and lateral to pubic tubercle (external oblique aponeurosis)
• Deep inguinal ring: 1.5 cm above midpoint of inguinal ligament (transversalis fascia)
• McBurney's point: 1/3 from right ASIS toward umbilicus (appendix base)
• Renal angle: 12th rib + lateral border of erector spinae (costovertebral angle)
• Murphy's point: right MCL + right costal margin (gall bladder fundus)
Organ Projections (AN55.2):
• Liver: 5th rib (right MCL) → right costal margin
• Gall bladder fundus: right MCL + costal margin (Murphy's point)
• Stomach: cardiac orifice at T10/11, pylorus at L1; fundus under left dome of diaphragm
• Spleen: 9th–11th ribs, left posterior axillary line; long axis = 10th rib
• Right kidney: T12–L3; Left kidney: T11/12–L2/3; hila at transpyloric plane
• Duodenum: 1st part at transpyloric plane; 2nd part L1–L3; 3rd part at L3; DJ flexure L2
• Pancreas: head at L2 (right), neck at L1, tail reaches splenic hilum
• Ileocaecal junction: right iliac fossa (McBurney's region)
• Root of mesentery: DJ flexure (L2, left) → right sacroiliac joint
Clinical signs:
• McBurney's sign = tenderness at McBurney's point = appendicitis
• Murphy's sign = inspiratory arrest on palpation at Murphy's point = cholecystitis
• Courvoisier's sign = palpable non-tender GB + jaundice = malignant obstruction