Page 1 of 4
AN59.1-4 | Pons — SDL Guide
Learning Objectives
- Identify the external features of the pons (AN59.1)
- Draw and label transverse sections of the pons at upper and lower levels (AN59.2)
- Describe cranial nerve nuclei in the pons with their functional groups (AN59.3)
- Describe the anatomical basis of pontine clinical conditions: locked-in syndrome, pontine haemorrhage, Foville, Raymond, and Millard-Gubler syndromes (AN59.4)
INSTRUCTIONS
The pons is divided into a ventral (basis pontis) and dorsal (pontine tegmentum) part. Learn them separately, then integrate the cranial nerve nuclei and tracts to understand the clinical syndromes.
References
- BD Chaurasia's Human Anatomy, Vol. 3 — Head, Neck & Brain (Textbook)
- Inderbir Singh's Human Neuroanatomy (Textbook)
- Snell's Clinical Neuroanatomy (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 50-year-old man with hypertension collapses in a Chennai hospital canteen. On examination: he is conscious, aware of surroundings, can blink in response to commands, but cannot speak, cannot move his arms or legs, cannot move his eyes horizontally. He can only move his eyes vertically and blink. All four limbs are completely paralysed (quadriplegia). He appears terrified but fully conscious.
MRI: massive haemorrhage in the pons (pontine haemorrhage).
This patient is completely aware but cannot communicate except through vertical eye movements — "locked-in syndrome." What structures in the pons are destroyed, and why are vertical eye movements spared?
WHY THIS MATTERS
Pontine anatomy is clinically important:
- Locked-in syndrome — rare but devastating; full consciousness with complete quadriplegia; vertical eye movements are the only communication channel
- Pontine haemorrhage — hypertensive bleed into the pons; high mortality; the "pin-point pupils" sign is pathognomonic
- Millard-Gubler and Foville syndromes — classic crossed brainstem syndromes tested in every Indian university examination
- Acoustic neuroma (vestibular schwannoma) — arises at the cerebellopontine angle; involves CN VII and VIII; most common intracranial tumour to affect young adults in India
- Internuclear ophthalmoplegia (INO) — MLF lesion in the pons; a hallmark of multiple sclerosis in young women
RECALL
Before we begin, recall:
- The pons lies between the medulla (below) and the midbrain (above)
- It forms the upper part of the floor of the 4th ventricle
- Cranial nerves V (trigeminal), VI (abducens), VII (facial), VIII (vestibulocochlear) have nuclei in or near the pons
- The pons connects to the cerebellum via the MIDDLE cerebellar peduncles (the largest)
Part 1: External Features (AN59.1)
Anterior (Ventral) Surface:
• Basilar groove — midline depression for the basilar artery
• Transverse pontine fibres (stria) and the middle cerebellar peduncles — prominent transverse ridges; fibres from the pontine nuclei cross to form the middle cerebellar peduncles (brachium pontis) connecting the pons to each cerebellar hemisphere
• Trigeminal nerve (CN V) — exits the anterior pons at the junction of its upper and lower thirds, on the lateral surface

Figure: Part 1: External Features (AN59.1)
Posterior Surface (floor of 4th ventricle — upper part):
• Facial colliculus — rounded elevation caused by the CN VII nerve fibres looping over the CN VI nucleus; in the upper floor of the 4th ventricle (lower pons)
• Median eminence — vertical ridge on each side of the midline
• Sulcus limitans — longitudinal groove separating the medial (efferent) from lateral (afferent) functional areas
• Locus coeruleus — pigmented area (melanin-containing noradrenergic neurons) visible through the 4th ventricular floor in the upper pons/lower midbrain region
• CN VI rootlets emerge anteriorly at the pontomedullary junction
• CN VII and VIII emerge at the cerebellopontine angle (lateral pontomedullary junction)

Figure: Part 1: External Features (AN59.1)
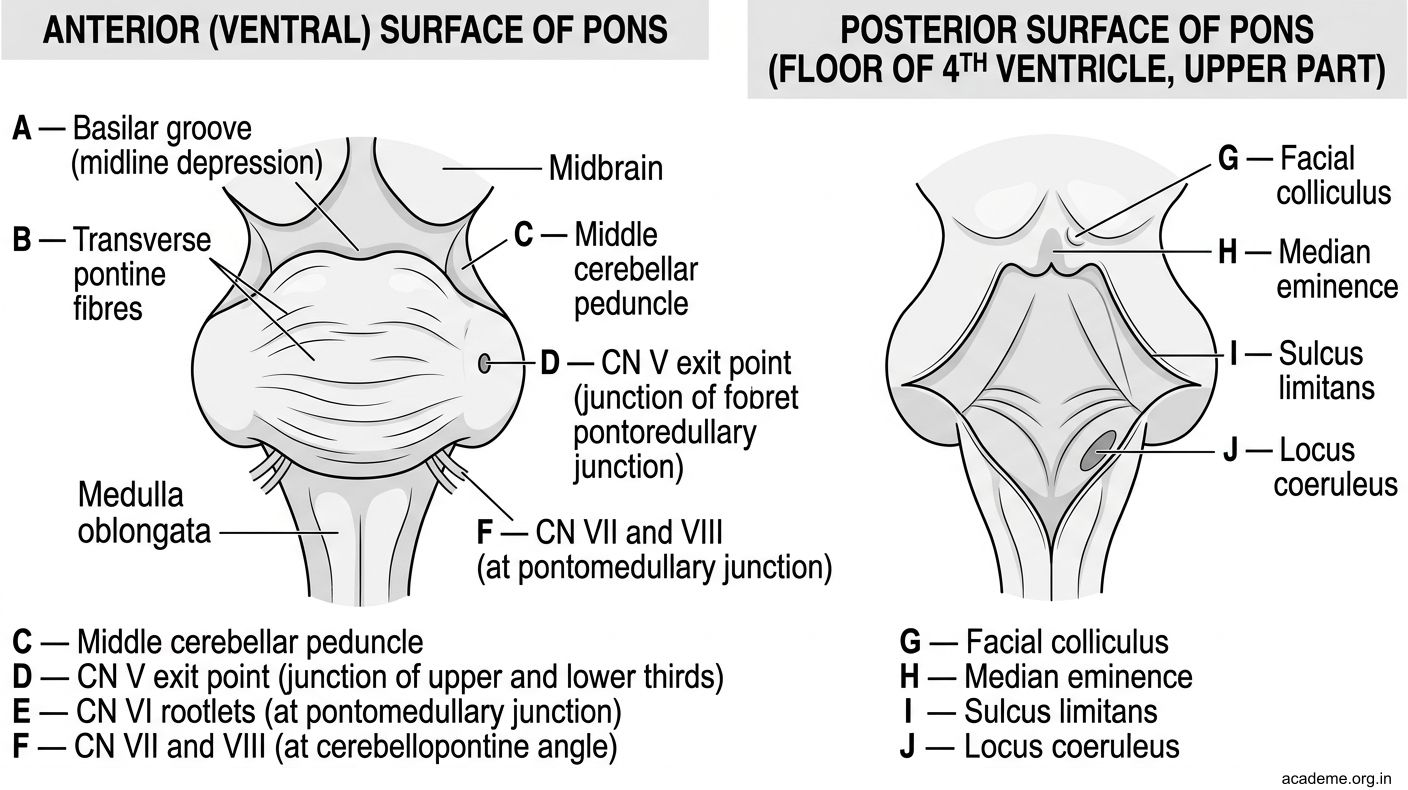
Figure: Part 1: External Features (AN59.1)
Part 2: Transverse Sections (AN59.2)
Lower Pontine Section (level of CN VI and VII)

Figure: Part 2: Transverse Sections (AN59.2)
The pons at this level is divided into:
Ventral part (Basis pontis):
• Longitudinal fibres — corticospinal (descending, scattered in bundles among the pontine nuclei) and corticobulbar fibres
• Transverse pontine fibres — pontocerebellar fibres (from pontine nuclei, cross midline, enter middle cerebellar peduncle)
• Pontine nuclei — grey matter scattered between the fibre bundles; relay for cerebrocerebellar pathway
Dorsal part (Pontine Tegmentum):
• CN VI nucleus (abducens) — near the midline in the floor of the 4th ventricle; motor to lateral rectus
• CN VII nucleus (facial motor) — ventrolateral to CN VI nucleus; motor to facial expression muscles
• Genu of CN VII — the facial nerve fibres loop posteriorly around the CN VI nucleus before exiting laterally → creates the facial colliculus visible on the 4th ventricle floor
• Medial longitudinal fasciculus (MLF) — runs near the midline; connects CN VI nucleus ↔ CN III nucleus (contralateral) for conjugate horizontal gaze
• Medial lemniscus — now horizontal strip in the dorsal tegmentum
• Spinothalamic tract — lateral tegmentum
• Superior olivary nucleus — auditory pathway relay; between CN VI and VII nuclei
Upper Pontine Section (level of CN V)
- CN V motor nucleus — medial; motor to muscles of mastication
- CN V main sensory nucleus (principal sensory nucleus) — lateral to motor; fine touch from face
- Mesencephalic nucleus of CN V — proprioception from jaw muscles (unique: 1st order neurons in the CNS, not in a peripheral ganglion)
- Medial lemniscus — continues as horizontal slab
- Locus coeruleus — beginning to appear at this upper level
- Middle cerebellar peduncle — dominant feature laterally
- Ventral: still has longitudinal corticospinal fibres + pontine nuclei
- The 4th ventricle narrows at this level
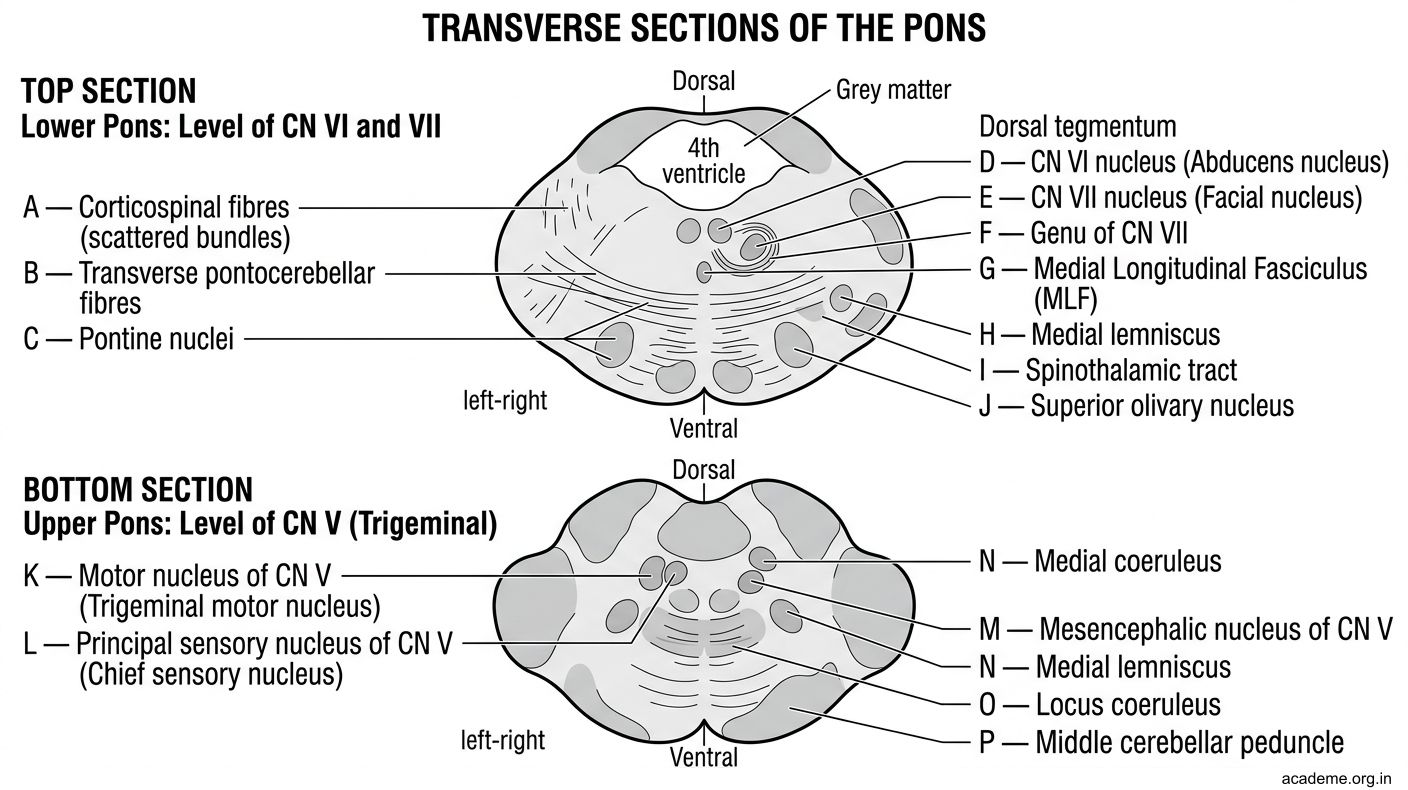
Figure: Part 2: Transverse Sections (AN59.2)

Figure: Upper Pontine Section (level of CN V)
Part 3: Cranial Nerve Nuclei in the Pons (AN59.3)
CN V — Trigeminal (4 nuclei, 3 in pons + 1 in medulla/cord)
| Nucleus | Location | Component | Function |
|---|---|---|---|
| Motor nucleus of CN V | Pons (upper) | SVE | Muscles of mastication |
| Principal (main) sensory nucleus | Pons (upper, lateral) | GSA | Fine touch from face |
| Mesencephalic nucleus | Midbrain | GSA | Proprioception from jaw muscles (masseters) |
| Spinal nucleus of CN V | Medulla → C2 cord | GSA | Pain and temperature from face |
CN VI — Abducens
| Component | Nucleus | Function |
|---|---|---|
| GSE (somatic motor) | CN VI nucleus (lower pons, medial) | Lateral rectus muscle → abduction of eye |
CN VII — Facial
| Component | Nucleus | Function |
|---|---|---|
| SVE (branchiomotor) | Facial motor nucleus (lower pons) | Muscles of facial expression |
| GVE (parasympathetic) | Superior salivatory nucleus | Submandibular + sublingual glands, lacrimal gland |
| SVA (taste) | Nucleus tractus solitarius (lower end) | Taste from anterior 2/3 tongue |
| GSA | Spinal nucleus CN V | Skin of ear (small area) |
CN VIII — Vestibulocochlear
| Division | Nucleus | Function |
|---|---|---|
| Cochlear | Cochlear nuclei (at pontomedullary junction) | Hearing; fibres decussate at level of pons as trapezoid body |
| Vestibular | Vestibular nuclei (4, at pontomedullary jx) | Balance; contribute to MLF for eye movements |

Figure: Part 3: Cranial Nerve Nuclei in the Pons (AN59.3)

Figure: CN VI — Abducens
Part 4: Pontine Clinical Syndromes (AN59.4)
1. Locked-in Syndrome
• Cause: Bilateral destruction of the basis pontis (corticospinal + corticobulbar fibres) — typically from pontine haemorrhage or basilar artery occlusion
• Features: Complete quadriplegia + anarthria (no speech) + horizontal gaze palsy (CN VI and PPRF destroyed)
• PRESERVED: Consciousness (reticular formation in tegmentum intact), VERTICAL eye movements (controlled by midbrain, not pons), blinking
• Communication: Only vertical eye movement or blinking
• Patient in the hook
2. Pontine Haemorrhage
• Cause: Hypertensive bleed into the pons; rupture of small basilar perforating arteries
• Classic signs: Pin-point pupils (bilateral, reactive to light) — sympathetic fibres descending destroyed + parasympathetic III intact; hyperthermia; quadriplegia; abnormal breathing; coma
• Pin-point pupils = pathognomonic of pontine haemorrhage
• High mortality (>80%)
3. Foville Syndrome (lower pontine tegmentum lesion)
• Structures: CN VI nucleus (or PPRF) + corticospinal tract + CN VII fascicles + medial lemniscus
• Features:
- Ipsilateral horizontal gaze palsy (CN VI nucleus / PPRF)
- Ipsilateral LMN facial palsy (CN VII)
- Contralateral hemiplegia (corticospinal)
- Contralateral sensory loss (medial lemniscus)
4. Raymond Syndrome (lower pons)
• Structures: CN VI fascicles + corticospinal tract only
• Features: Ipsilateral lateral rectus palsy (CN VI — eye cannot abduct ipsilateral) + Contralateral hemiplegia
5. Millard-Gubler Syndrome (lower pons)
• Structures: CN VI nucleus/fascicles + CN VII fascicles + corticospinal tract
• Features: Ipsilateral lateral rectus palsy (CN VI) + Ipsilateral LMN facial palsy (CN VII) + Contralateral hemiplegia
• More common than Raymond; facial palsy differentiates from Raymond
Summary Table:
| Syndrome | CN VI | CN VII | Motor (contra) |
|---|---|---|---|
| Raymond | Yes (fascicle) | No | Yes |
| Millard-Gubler | Yes | Yes (fascicle) | Yes |
| Foville | Gaze palsy (nucleus/PPRF) | Yes | Yes |

Figure: CN VIII — Vestibulocochlear

Figure: Part 4: Pontine Clinical Syndromes (AN59.4)

Figure: Internuclear Ophthalmoplegia (INO) — MLF Lesion
SELF-CHECK — : Pons
The facial colliculus on the floor of the 4th ventricle is formed by the facial nerve fibres looping over which nucleus?
A. CN VII motor nucleus
B. CN VI (abducens) nucleus
C. CN VIII cochlear nucleus
D. Superior olivary nucleus
Reveal Answer
Answer: B. CN VI (abducens) nucleus
Pin-point pupils in pontine haemorrhage result from:
A. Direct compression of CN III
B. Cerebellar herniation
C. Bilateral destruction of descending sympathetic fibres in the pontine tegmentum
D. Activation of Edinger-Westphal nucleus
Reveal Answer
Answer: C. Bilateral destruction of descending sympathetic fibres in the pontine tegmentum
The mesencephalic nucleus of CN V is unique among cranial nerve nuclei because:
A. Its first-order neurons are located within the CNS (not in a peripheral ganglion)
B. It is found only in the medulla
C. It provides taste sensation from the anterior tongue
D. It contains parasympathetic preganglionic neurons
Reveal Answer
Answer: A. Its first-order neurons are located within the CNS (not in a peripheral ganglion)
CLINICAL PEARL
Internuclear Ophthalmoplegia (INO) — MLF Lesion
The medial longitudinal fasciculus (MLF) connects the CN VI nucleus on one side to the CN III nucleus on the other side, coordinating horizontal conjugate gaze.
INO: Lesion of the MLF in the pons → on attempted horizontal gaze toward the side of the LESION, the IPSILATERAL eye (adducting eye) fails to adduct fully, while the contralateral eye shows horizontal nystagmus.
- Cause in young adults: Multiple sclerosis (bilateral INO = virtually diagnostic of MS)
- Cause in elderly: Brainstem stroke (usually unilateral INO)
- Test: Observe each eye during horizontal gaze — the adducting eye lags
Acoustic neuroma (vestibular schwannoma):
• Tumour of CN VIII Schwann cells at the cerebellopontine angle (CPA)
• Presents with: unilateral sensorineural deafness, tinnitus, and vestibular dysfunction
• Later: involves CN VII (facial weakness) and the pons (brainstem compression)
• Treated with microsurgery or stereotactic radiosurgery (Gamma Knife)
REFLECT
Return to the hook case — the locked-in patient:
- Explain why he cannot move his limbs (all four are paralysed). Which tracts in the pons are destroyed?
- Why can he move his eyes VERTICALLY but not HORIZONTALLY? Where is vertical gaze controlled?
- Why is he fully conscious despite a massive pontine haemorrhage? What part of the pons is relatively spared?
- If another patient has unilateral pontine lesion with ipsilateral CN VII palsy + ipsilateral lateral rectus palsy + contralateral hemiplegia, which syndrome is this?
Discussion: (1) Bilateral corticospinal tracts in basis pontis destroyed → quadriplegia. (2) Horizontal gaze = PPRF + CN VI nuclei in lower pons (destroyed). Vertical gaze = midbrain (rostral interstitial nucleus of MLF, riMLF — intact). (3) Reticular activating system is in the TEGMENTUM (dorsal pons); basis pontis lesion spares tegmentum → consciousness preserved. (4) Millard-Gubler syndrome (CN VI + CN VII ipsilateral + contralateral hemiplegia).
KEY TAKEAWAYS
Key Takeaways — Pons
- External features: Basilar groove (basilar artery), transverse fibres → middle cerebellar peduncles, facial colliculus (4th ventricle floor)
- Lower pons section: Basis pontis (corticospinal, pontine nuclei, transverse fibres) + Tegmentum (CN VI, CN VII genu, MLF, medial lemniscus)
- Upper pons section: CN V motor + principal sensory + mesencephalic nuclei; middle cerebellar peduncles dominant
- CN VII nuclei: Motor (SVE), Superior salivatory (GVE-parasympathetic), NTS (taste SVA), Spinal CN V (GSA)
- Syndromes: Locked-in (bilateral basis pontis) = quadriplegia + preserved vertical gaze + consciousness; Millard-Gubler (CN VI + VII ipsilateral + contralateral hemiplegia); Raymond (CN VI + contralateral hemiplegia); Foville (gaze palsy + CN VII + contralateral)
- Pin-point pupils = pontine haemorrhage (sympathetics destroyed bilaterally)