Page 1 of 4
AN61.1-3 | Midbrain — SDL Guide
Learning Objectives
- Identify the external and internal features of the midbrain (AN61.1)
- Describe the internal features at the level of the superior and inferior colliculus (AN61.2)
- Describe the anatomical basis of Weber, Benedikt, and Parinaud syndromes (AN61.3)
INSTRUCTIONS
Divide the midbrain into tectum (dorsal), tegmentum (middle), and cerebral peduncles (ventral). Map each syndrome to the specific region and structure involved.
References
- BD Chaurasia's Human Anatomy, Vol. 3 — Head, Neck & Brain (Textbook)
- Inderbir Singh's Human Neuroanatomy (Textbook)
- Snell's Clinical Neuroanatomy — Midbrain (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 65-year-old man with known hypertension presents with sudden left-sided weakness of the arm and leg, and a RIGHT-sided drooping eyelid, dilated pupil, and outward deviation of the right eye. The right eye cannot look medially, superiorly, or inferiorly.
MRI brain: infarct in the right midbrain cerebral peduncle and right CN III fascicles.
How does a single midbrain lesion cause ipsilateral CN III palsy AND contralateral hemiplegia?
WHY THIS MATTERS
- Weber syndrome — classic crossed syndrome testing CN III anatomy relative to corticospinal tract in midbrain
- Parinaud syndrome — dorsal midbrain syndrome; caused by pineal gland tumours (germinomas) in Indian adolescents — a high-yield surgical case
- CN III palsy — critical to differentiate compressive (PCOM aneurysm, herniation) from ischaemic; the pupil is the key
- Vertical gaze control — located in the midbrain rostral interstitial MLF; essential for locked-in syndrome distinction from midbrain lesions
RECALL
Before we begin:
• The midbrain is the smallest brainstem segment, connecting the pons (below) to the diencephalon (above)
• It has an aqueduct of Sylvius (cerebral aqueduct) running through its center
• It contains CN III (oculomotor) and CN IV (trochlear) nuclei
• The cerebral peduncles contain the corticospinal and corticobulbar fibres
Part 1: External Features (AN61.1)
Dorsal Surface (Tectum):
• Superior colliculi (2) — visual reflex centres; light → pupils constrict; visual startle reflex
• Inferior colliculi (2) — auditory reflex centres; orientation to sound
• Together = corpora quadrigemina (quadrigeminal plate)
• Brachium of superior colliculus — connects superior colliculus to lateral geniculate body
• Brachium of inferior colliculus — connects inferior colliculus to medial geniculate body
• CN IV (trochlear) — only CN to exit from DORSAL brainstem; emerges below the inferior colliculus, then winds around the brainstem to the front

Figure: Part 1: External Features (AN61.1)
Ventral Surface:
• Cerebral peduncles (crus cerebri) — large bilateral ridges containing corticospinal (middle 3/5) and corticobulbar (inner 1/5) fibres + corticopontine fibres (outer 1/5 each side)
• Interpeduncular fossa — triangular depression between the two peduncles; contains interpeduncular cistern
• CN III rootlets emerge from the medial surface of the cerebral peduncle (oculomotor sulcus)
• Posterior perforated substance — in the interpeduncular fossa; small perforating arteries enter for midbrain supply

Figure: Part 1: External Features (AN61.1)
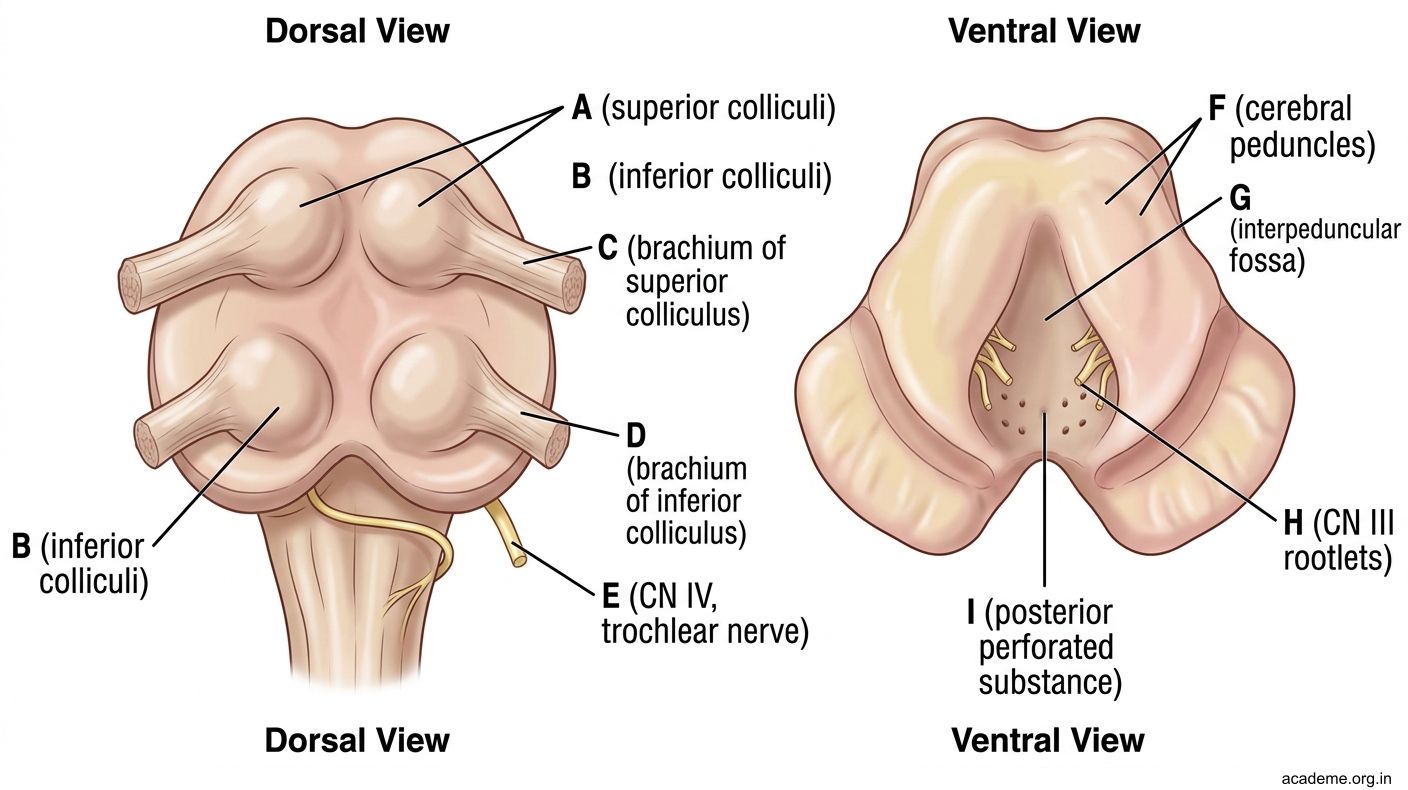
Figure: Part 1: External Features (AN61.1)
Part 2: Transverse Sections (AN61.2)
Level of the Inferior Colliculus:

Figure: Part 2: Transverse Sections (AN61.2)
Tectum (dorsal): Inferior colliculus — prominent auditory relay; projects to medial geniculate body via brachium
Tegmentum:
• CN IV nucleus — near the midline, just below the aqueduct (dorsal to MLF)
• Medial longitudinal fasciculus (MLF) — near midline
• Decussation of superior cerebellar peduncle — most important landmark at this level; both superior cerebellar peduncles (from dentate nuclei) cross each other here to reach the red nucleus and thalamus on the opposite side
• Lateral lemniscus — auditory fibres ascending to inferior colliculus
• Spinothalamic tract + medial lemniscus — lateral tegmentum
Basis (Crus cerebri): Corticospinal fibres (middle 3/5)
Level of the Superior Colliculus:
Tectum (dorsal): Superior colliculus — visual startle + pupil light reflex (pretectal nucleus at this level)
Tegmentum:
• CN III nucleus (oculomotor) — near midline, just ventral to the aqueduct
• Edinger-Westphal nucleus — adjacent to CN III nucleus; preganglionic parasympathetic → ciliary ganglion → constrictor pupillae + ciliary muscle (accommodation)
• Red nucleus — large, round, pigmented (iron); receives dentatorubral fibres (from dentate nucleus via superior cerebellar peduncle) + corticorubral fibres; gives rise to rubrospinal tract
• Substantia nigra — between tegmentum and basis; two parts: pars compacta (dopamine-producing) and pars reticulata (GABAergic output to thalamus + superior colliculus)
• MLF + Spinothalamic + Medial lemniscus — continue from below
• Cerebral aqueduct — surrounded by periaqueductal grey (PAG); important for pain modulation and descending opioid pathways
Basis: Corticospinal fibres (middle 3/5)
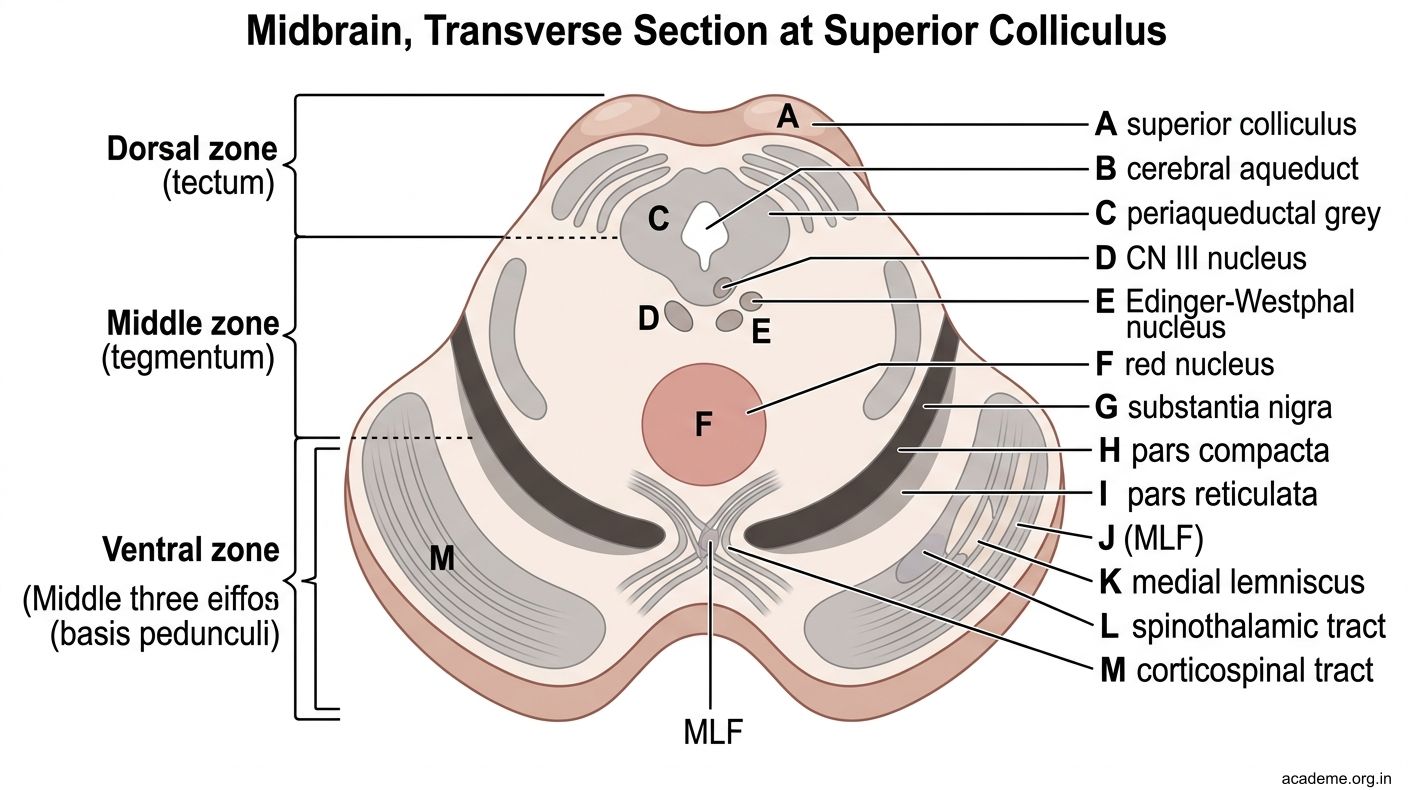
Figure: Part 2: Transverse Sections (AN61.2)

Figure: Level of the Superior Colliculus:
Part 3: Midbrain Clinical Syndromes (AN61.3)
Weber Syndrome (Ventral midbrain / Cerebral peduncle)
• Cause: Infarct of the cerebral peduncle (posterior communicating artery territory)
• Structures: CN III fascicles (exiting medial peduncle) + corticospinal tract (in the peduncle)
• Features:
- Ipsilateral CN III palsy (LMN): dilated fixed pupil (mydriasis), ptosis, eye deviated down-and-out, loss of medial/superior/inferior gaze on the affected side
- Contralateral hemiplegia (UMN): the corticospinal tract in the peduncle crosses in the medulla
• Patient in the hook = right Weber syndrome
Benedikt Syndrome (Dorsal tegmentum)
• Cause: Infarct of midbrain tegmentum (paramedian perforators)
• Structures: CN III fascicles + red nucleus (+ often medial lemniscus)
• Features:
- Ipsilateral CN III palsy (same as Weber)
- Contralateral involuntary movements (tremor, choreiform, athetosis) from red nucleus damage + contralateral sensory loss if medial lemniscus involved
- NO hemiplegia (corticospinal tract in basis pedunculi is spared)
Parinaud Syndrome (Dorsal midbrain / Tectal syndrome)
• Cause: Compression of the dorsal midbrain (superior colliculus + pretectal area) — most commonly by a pineal region tumour (germinoma, pineocytoma) in Indian adolescents and young adults; also hydrocephalus dilating the aqueduct
• Structures: Pretectal nucleus (pupillary light reflex) + rostral interstitial MLF (vertical gaze) + superior colliculi
• Features:
- Paralysis of upward gaze (vertical gaze palsy) — cannot look upward
- Pupillary light-near dissociation — pupils react to accommodation (near reflex) but NOT to direct light (selective pretectal nucleus damage)
- Convergence-retraction nystagmus — eyes attempt to look up but converge and retract instead
- Lid retraction (Collier's sign)
Summary:
| Syndrome | Location | CN III | Motor | Other |
|---|---|---|---|---|
| Weber | Cerebral peduncle | Ipsilateral palsy | Contralateral hemiplegia | — |
| Benedikt | Tegmentum | Ipsilateral palsy | No paralysis | Contralateral tremor/movement disorder |
| Parinaud | Tectum / pretectal | No CN III palsy | No paralysis | Upgaze palsy + light-near dissociation |

Figure: Part 3: Midbrain Clinical Syndromes (AN61.3)

Figure: Pupil-sparing CN III Palsy — Critical Distinction
SELF-CHECK — : Midbrain
In Weber syndrome, the contralateral hemiplegia results from damage to:
A. Red nucleus
B. Corticospinal tract in the cerebral peduncle (basis pedunculi)
C. Superior colliculus
D. Substantia nigra
Reveal Answer
Answer: B. Corticospinal tract in the cerebral peduncle (basis pedunculi)
The Edinger-Westphal nucleus is part of the CN III complex. It provides:
A. Somatic motor to extraocular muscles
B. Sympathetic supply to the dilator pupillae
C. Preganglionic parasympathetic fibres to the constrictor pupillae and ciliary muscle
D. Sensory fibres from the cornea
Reveal Answer
Answer: C. Preganglionic parasympathetic fibres to the constrictor pupillae and ciliary muscle
Parinaud syndrome is characterised by paralysis of upward gaze and pupillary light-near dissociation. The most common cause in Indian adolescents is:
A. Pineal region tumour (germinoma/pineocytoma)
B. Pontine haemorrhage
C. Bilateral temporal lobe infarcts
D. Anterior communicating artery aneurysm
Reveal Answer
Answer: A. Pineal region tumour (germinoma/pineocytoma)
CLINICAL PEARL
Pupil-sparing CN III Palsy — Critical Distinction
| Feature | Compressive CN III Palsy | Ischaemic CN III Palsy |
|---|---|---|
| Pupil | Involved (dilated, fixed) | SPARED (normal size, reactive) |
| Onset | Sudden; may have headache | Sudden; painless |
| Cause | PCOM aneurysm; transtentorial herniation | Diabetes, hypertension |
| Urgency | EMERGENCY — aneurysm may rupture | Less urgent; monitor |
Anatomical basis: Parasympathetic fibres (from Edinger-Westphal nucleus) run on the OUTER SURFACE of CN III. External compression (aneurysm, herniation) affects outer fibres first → pupil dilates early. Ischaemia damages the central core (somatic motor fibres) while sparing peripheral parasympathetic fibres → pupil spared.
Rule: Any painful CN III palsy with pupil involvement → rule out posterior communicating artery aneurysm urgently (CT angiography/MR angiography). Do not dismiss as ischaemic.
REFLECT
Return to the hook case:
- Why does the lesion in the RIGHT midbrain peduncle cause LEFT-sided weakness?
- Why is the RIGHT eye "down and out"? Which muscles are paralysed?
- If the same patient also had contralateral tremor/choreiform movements but NO hemiplegia, which syndrome would that be?
- In Parinaud syndrome, why can the pupils accommodate (near reflex) but not react to light?
Discussion: (1) Corticospinal crosses in medulla — right peduncle lesion → left hemiplegia. (2) Down and out = LR (CN VI) and SO (CN IV) unopposed after CN III palsy; ptosis (levator palpebrae = CN III); mydriasis (parasympathetics = CN III). (3) Benedikt syndrome (red nucleus + CN III; no basis involvement). (4) Pretectal nucleus mediates pupillary light reflex; near reflex goes directly to Edinger-Westphal via cortical pathway bypassing pretectal area — selectively spared.
KEY TAKEAWAYS
Key Takeaways — Midbrain
- Tectum: Superior colliculi (visual reflexes), Inferior colliculi (auditory)
- Tegmentum at inferior colliculus level: CN IV nucleus, decussation of superior cerebellar peduncle
- Tegmentum at superior colliculus level: CN III + Edinger-Westphal (parasympathetic), Red nucleus, Substantia nigra, PAG
- Basis pedunculi: Corticospinal (middle 3/5), corticopontine (outer 1/5 each), corticobulbar (inner 1/5 each)
- Weber: Peduncle → ipsi CN III + contra hemiplegia
- Benedikt: Tegmentum → ipsi CN III + contra movement disorder
- Parinaud: Tectum/pretectal → upgaze palsy + light-near dissociation (no CN III palsy)
- Substantia nigra dopamine pathway: SN → striatum; lost in Parkinson's disease