Page 1 of 6
AN62.1-6 | Cranial nerve nuclei & Cerebral hemispheres — SDL Guide
Learning Objectives
- Describe cranial nerve nuclei with their functional components (AN62.1)
- Describe surfaces, sulci, gyri, poles, and functional areas of the cerebral hemisphere with effects of damage (AN62.2)
- Describe the white matter of the cerebrum and effects of damage to the corpus callosum and internal capsule (AN62.3)
- Describe the basal ganglia, limbic lobe, and anatomical basis of Parkinson's disease, chorea, athetosis, and ballismus (AN62.4)
- Describe the thalamus, hypothalamus, epithalamus, metathalamus, and subthalamus (AN62.5)
- Describe the formation, branches, and distribution of the circle of Willis (AN62.6)
INSTRUCTIONS
This is the largest topic in the neuroanatomy block. Divide your study into 6 sessions matching the 6 competencies. Draw the medial and lateral surfaces of the brain from memory after studying the functional areas.
References
- BD Chaurasia's Human Anatomy, Vol. 3 — Head, Neck & Brain (Textbook)
- Inderbir Singh's Human Neuroanatomy (Textbook)
- Gray's Anatomy for Students — Cerebral Hemispheres (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
Three patients admitted to a Chennai neurology ward on the same day:
Patient A (72-year-old): Sudden onset inability to speak (aphasia) and right arm + face weakness; right homonymous hemianopia. BP: 190/110 mmHg.
Patient B (65-year-old): Pill-rolling resting tremor of both hands (right > left), stooped posture, shuffling gait, mask-like facies, cogwheel rigidity. Symptoms for 3 years, progressive.
Patient C (50-year-old): Sudden onset involuntary flinging movements of the left arm and leg (hemiballismus). BP: 160/100. MRI: small infarct in the right subthalamic nucleus.
Each patient's deficit maps to a specific region of the brain. Understanding the cerebral hemispheres, basal ganglia, and deep structures is the foundation of clinical neurology.
WHY THIS MATTERS
- Stroke — leading cause of adult disability in India; anatomy determines stroke territory and clinical deficit
- Parkinson's disease — affects ~3 million Indians; basal ganglia anatomy is the foundation of its pathophysiology and drug treatment
- Aphasia — Broca's and Wernicke's areas are tested in every MBBS examination and clinical case
- Internal capsule anatomy — guides CT/MRI interpretation of lacunar infarcts (the most common stroke type in Indian hypertensive patients)
- Circle of Willis — berry aneurysms at its junctions cause subarachnoid haemorrhage — a neurosurgical emergency
RECALL
Before we begin:
• The cerebrum has two hemispheres connected by the corpus callosum
• Each hemisphere has 4 lobes: frontal, parietal, temporal, occipital
• The grey matter (cortex) covers the white matter; deep grey nuclei = basal ganglia and thalamus
• Blood supply to the brain: internal carotid arteries (anterior circulation) + vertebral arteries (posterior circulation) → circle of Willis
Part 1: Cranial Nerve Nuclei — Functional Classification (AN62.1)
Functional Column Classification
Cranial nerve nuclei are organized into 7 functional columns (based on embryological derivation):
| Column | Abbreviation | Function | Example CNs |
|---|---|---|---|
| General somatic afferent | GSA | Touch, pain, temp, proprioception from body + face | CN V, VII, IX, X |
| General visceral afferent | GVA | Visceral sensation | CN VII, IX, X |
| Special visceral afferent | SVA | Taste, smell | CN I, VII, IX, X |
| Special somatic afferent | SSA | Vision, hearing, balance | CN II, VIII |
| General somatic efferent | GSE | Motor to striated muscles (somite-derived) | CN III, IV, VI, XII |
| General visceral efferent | GVE | Parasympathetic (smooth muscle, glands) | CN III, VII, IX, X |
| Special visceral efferent | SVE | Branchiomotor (pharyngeal arch muscles) | CN V, VII, IX, X, XI |
Complete CN Nucleus Summary:
CN III (Midbrain): CN III motor (GSE: EOM) + Edinger-Westphal (GVE: parasympathetic)
CN IV (Midbrain): CN IV nucleus (GSE: superior oblique)
CN V (Pons/Medulla/Cord): Motor (SVE: mastication) + Principal sensory (GSA: fine touch face) + Mesencephalic (GSA: jaw proprioception) + Spinal (GSA: pain/temp face)
CN VI (Lower pons): CN VI nucleus (GSE: lateral rectus)
CN VII (Lower pons): Facial motor (SVE: expression) + Superior salivatory (GVE: para) + NTS (SVA: taste ant 2/3 + GVA) + Spinal CN V (GSA)
CN VIII (Pontomedullary junction): Cochlear nuclei (SSA: hearing) + Vestibular nuclei (SSA: balance)
CN IX (Medulla): Nucleus ambiguus (SVE: stylopharyngeus) + Inferior salivatory (GVE: parotid) + NTS (GVA: carotid body + SVA: taste post 1/3) + Spinal CN V (GSA: ear skin)
CN X (Medulla): Nucleus ambiguus (SVE: pharynx/larynx) + Dorsal motor vagus (GVE: thoracoabdominal) + NTS (GVA: viscera + SVA: taste epiglottis) + Spinal CN V (GSA: ear skin)
CN XI: Cranial root: nucleus ambiguus (SVE). Spinal root: C1–C5 anterior horn (GSE: SCM + trapezius)
CN XII (Medulla): Hypoglossal nucleus (GSE: tongue)
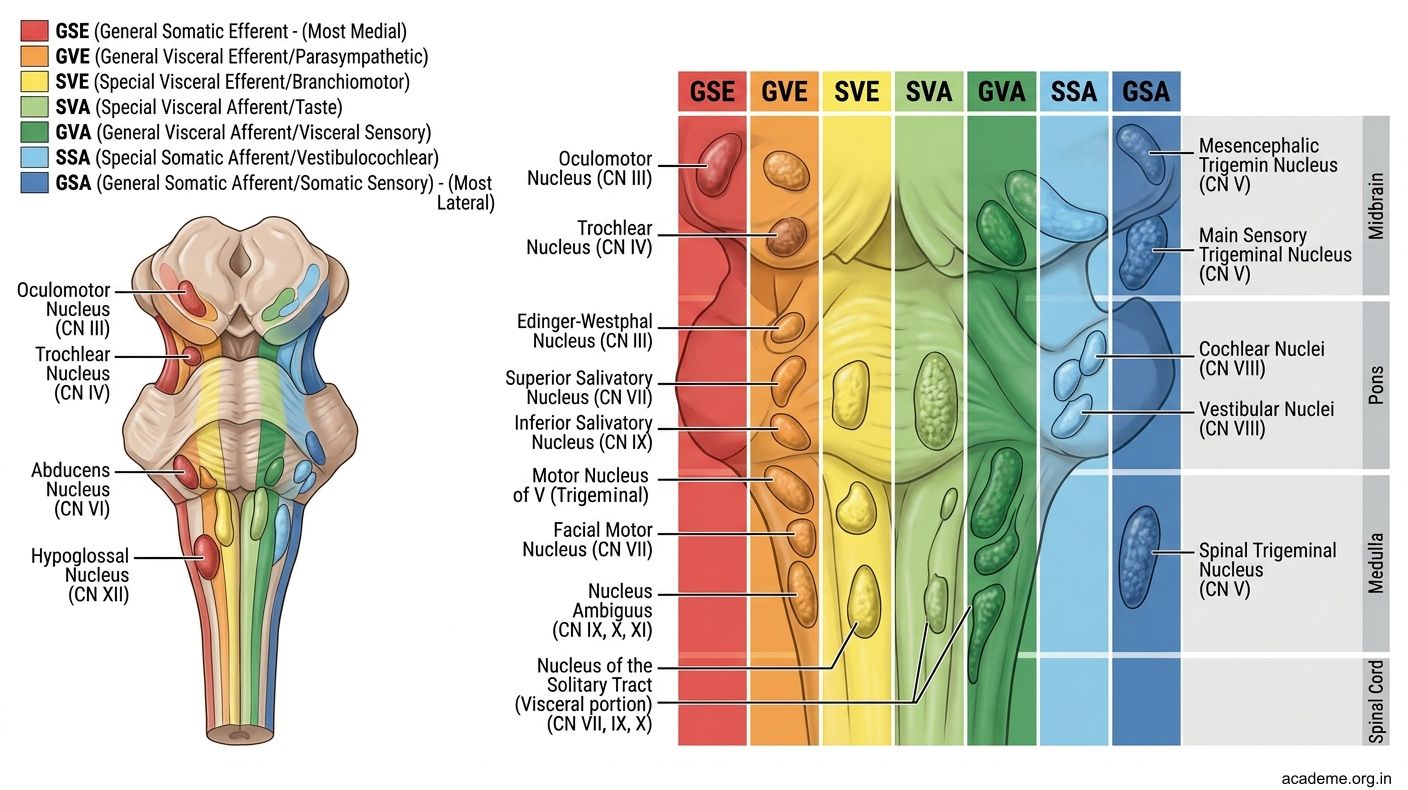
Figure: Part 1: Cranial Nerve Nuclei — Functional Classification (AN62.1)
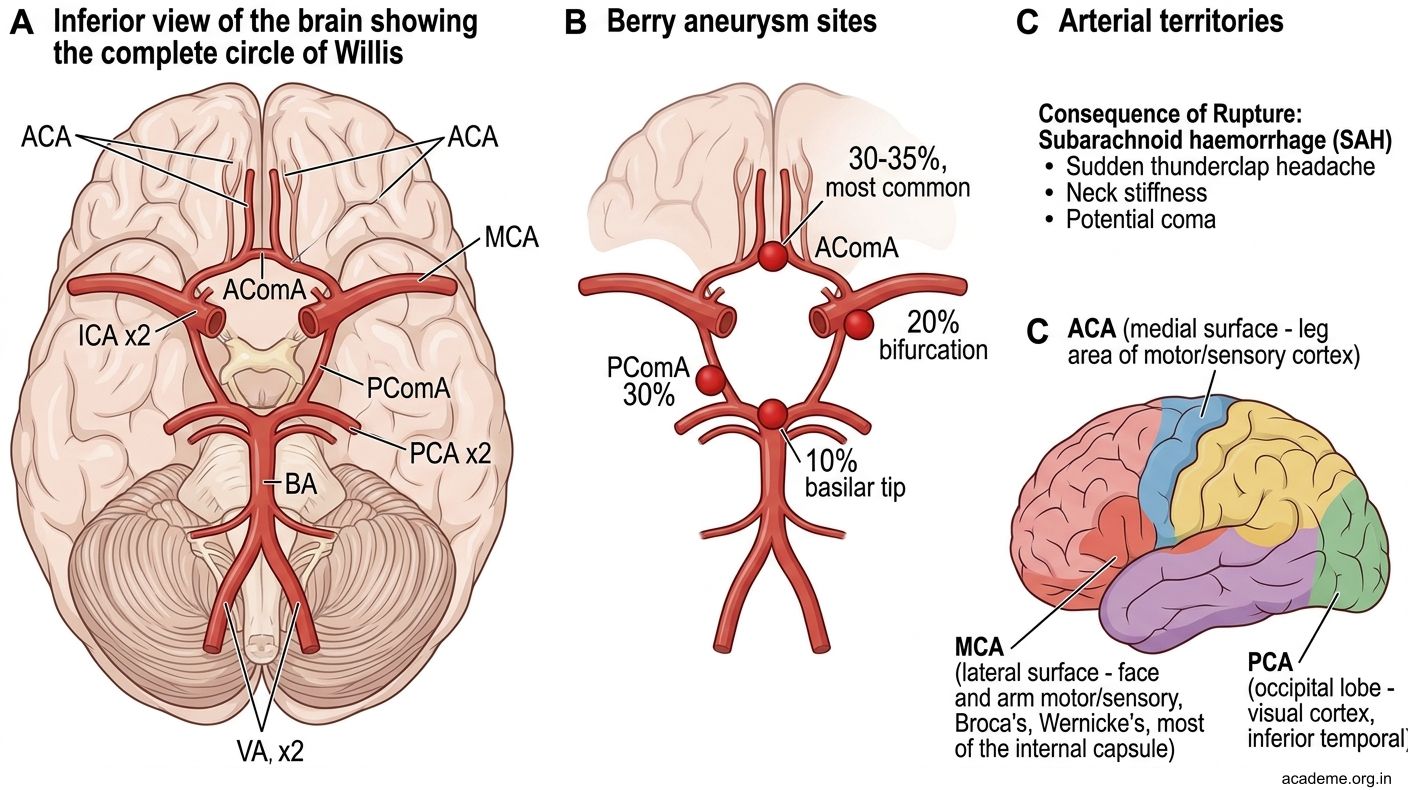
Figure: Complete CN Nucleus Summary:
Part 2: Cerebral Hemisphere — Surfaces, Lobes & Functional Areas (AN62.2)
Lobes and Bounding Sulci
| Lobe | Boundaries | Key Gyri |
|---|---|---|
| Frontal | Anterior to central sulcus; above lateral fissure | Precentral gyrus (primary motor), Broca's area (44,45 — left hemisphere) |
| Parietal | Behind central sulcus; above lateral fissure; anterior to parietooccipital sulcus | Postcentral gyrus (primary somatosensory), Superior/inferior parietal lobules |
| Temporal | Below lateral fissure | Superior temporal gyrus (Wernicke's area 22 — left; primary auditory cortex 41/42 — Heschl's gyrus) |
| Occipital | Posterior to parietooccipital sulcus | Calcarine sulcus (primary visual cortex area 17) |
| Limbic | Medial surface | Cingulate gyrus, parahippocampal gyrus, hippocampus (dentate gyrus + Ammon's horn) |
Functional Areas (Brodmann Areas):
| Area | Location | Function | Damage effect |
|---|---|---|---|
| Area 4 | Precentral gyrus | Primary motor cortex | Contralateral UMN weakness |
| Area 6 | Premotor + supplementary motor | Motor planning | Apraxia |
| Areas 44, 45 | Left inferior frontal gyrus | Broca's area (motor speech) | Broca's aphasia — non-fluent, understands but cannot speak |
| Areas 1,2,3 | Postcentral gyrus | Primary somatosensory | Contralateral sensory loss |
| Area 17 | Calcarine cortex (occipital) | Primary visual | Contralateral homonymous hemianopia |
| Areas 41, 42 | Heschl's gyrus (superior temporal) | Primary auditory | Rarely total deafness (bilateral representation) |
| Area 22 | Left superior temporal gyrus | Wernicke's area (speech comprehension) | Wernicke's aphasia — fluent but incomprehensible (jargon) |
Somatotopic Motor Homunculus:
• Primary motor cortex (area 4) has a somatotopic map — from medial to lateral: leg (medial, near falx) → trunk → arm → face (lateral)
• Cortical representation proportional to movement complexity (large hand and face representation)
• MCA territory = arm + face. ACA territory = leg
Effects of damage:
• Patient A (hook) = left MCA territory infarct: right arm + face weakness (motor cortex + internal capsule) + Broca's aphasia (area 44/45 in left inferior frontal) + right homonymous hemianopia (optic radiation through temporal/parietal lobe → primary visual cortex)
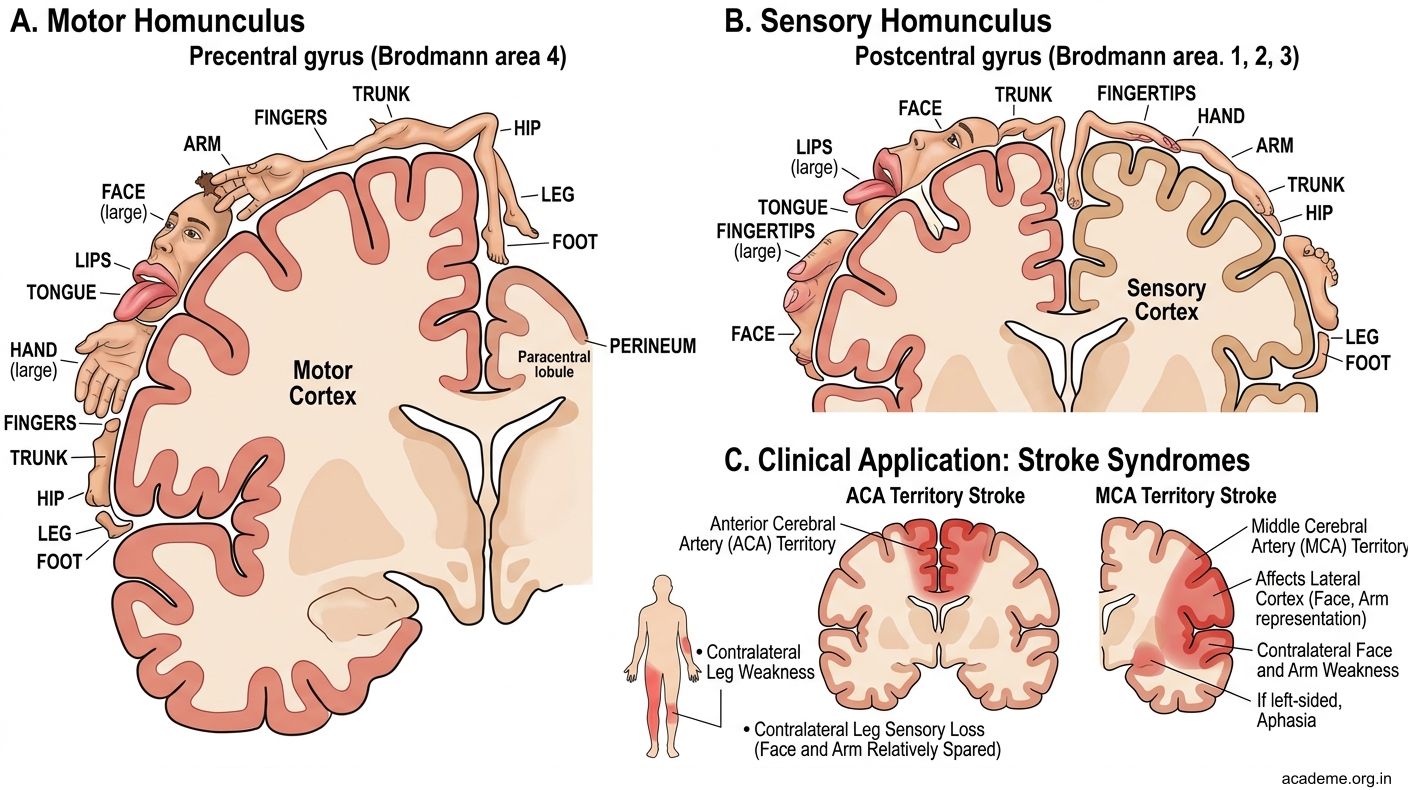
Figure: Lobes and Bounding Sulci
Part 3: White Matter & Internal Capsule (AN62.3)
Types of White Matter Fibres:
1. Commissural fibres — connect homologous areas in opposite hemispheres
- Corpus callosum (largest): genu (frontal lobes), body (parietal), splenium (occipital) + temporal
- Anterior commissure (temporal lobes + olfactory)
- Posterior commissure (pretectal area)
- Habenular commissure, Hippocampal commissure
2. Association fibres — connect areas within the SAME hemisphere
- Short U-fibres (adjacent gyri)
- Long: Superior longitudinal fasciculus, Uncinate fasciculus, Arcuate fasciculus (connects Broca and Wernicke = SPEECH), Cingulum
3. Projection fibres — connect cortex to subcortical structures (corona radiata → internal capsule → brainstem/cord)
- Internal capsule — the most clinically important white matter structure
Internal Capsule:
V-shaped on horizontal section (opens laterally):
| Part | Contents | Clinical |
|---|---|---|
| Anterior limb | Frontopontine + anterior thalamic radiation | Frontal functions |
| Genu | Corticobulbar fibres (face, head, neck) | UMN facial palsy if damaged |
| Posterior limb | Corticospinal (anterior 2/3: arm then leg) + somatosensory radiation (posterior 1/3) | Contralateral hemiplegia + sensory loss |
| Retrolenticular | Optic radiation (visual) | Homonymous hemianopia (contralateral) |
| Sublenticular | Auditory radiation + temporopontine | — |
Corpus callosum damage effects:
• Section of genu → alien hand syndrome + dementia-like features
• Section of splenium → alexia without agraphia (left visual cortex disconnected from speech areas)
• Agenesis of corpus callosum — often asymptomatic (congenital) but may cause seizures, intellectual disability
Internal capsule lacunar infarct:
The single most common stroke in Indian hypertensive patients. Small perforating artery (lenticulostriate) occlusion → pure motor stroke (posterior limb) or sensorimotor stroke. CT may be normal early — MRI DWI is the gold standard.
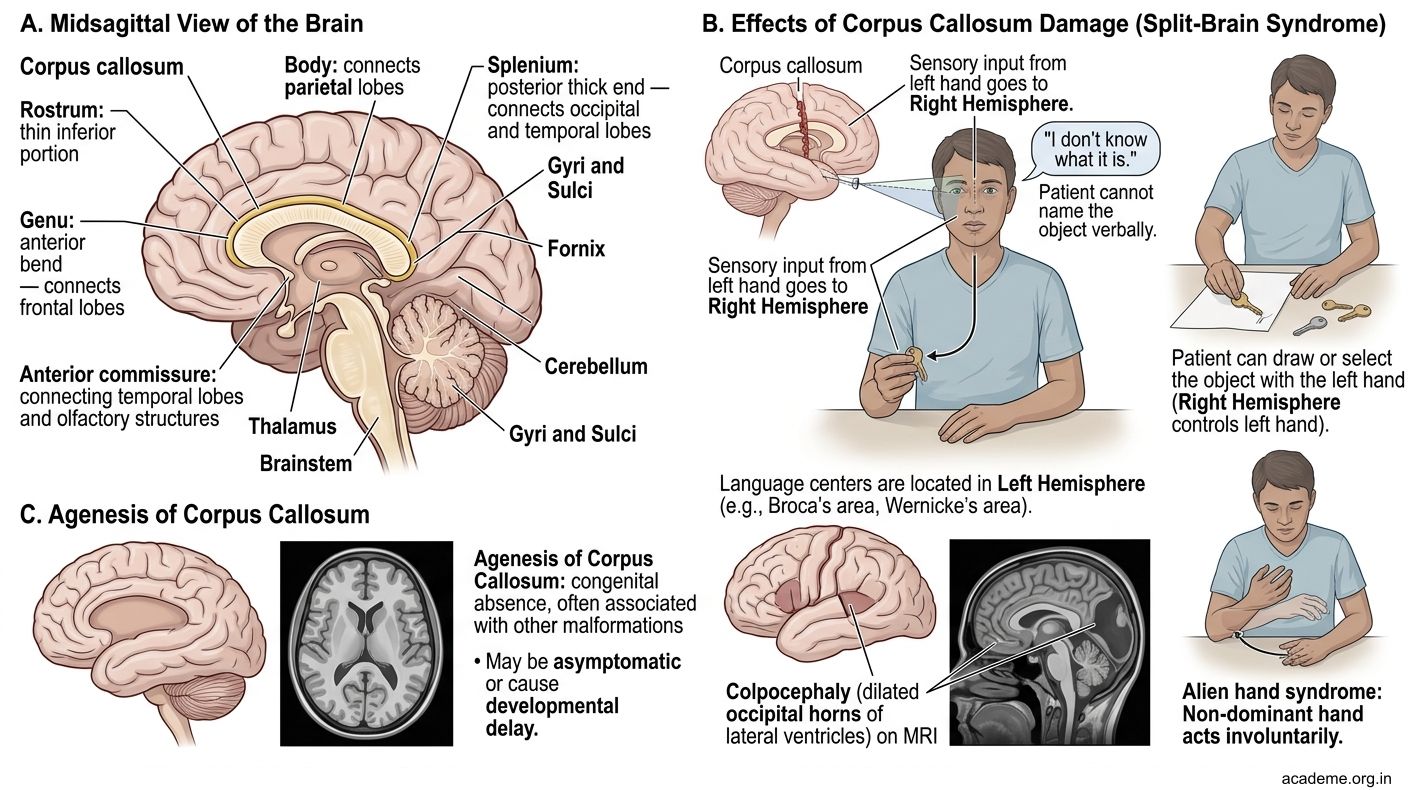
Figure: Types of White Matter Fibres:
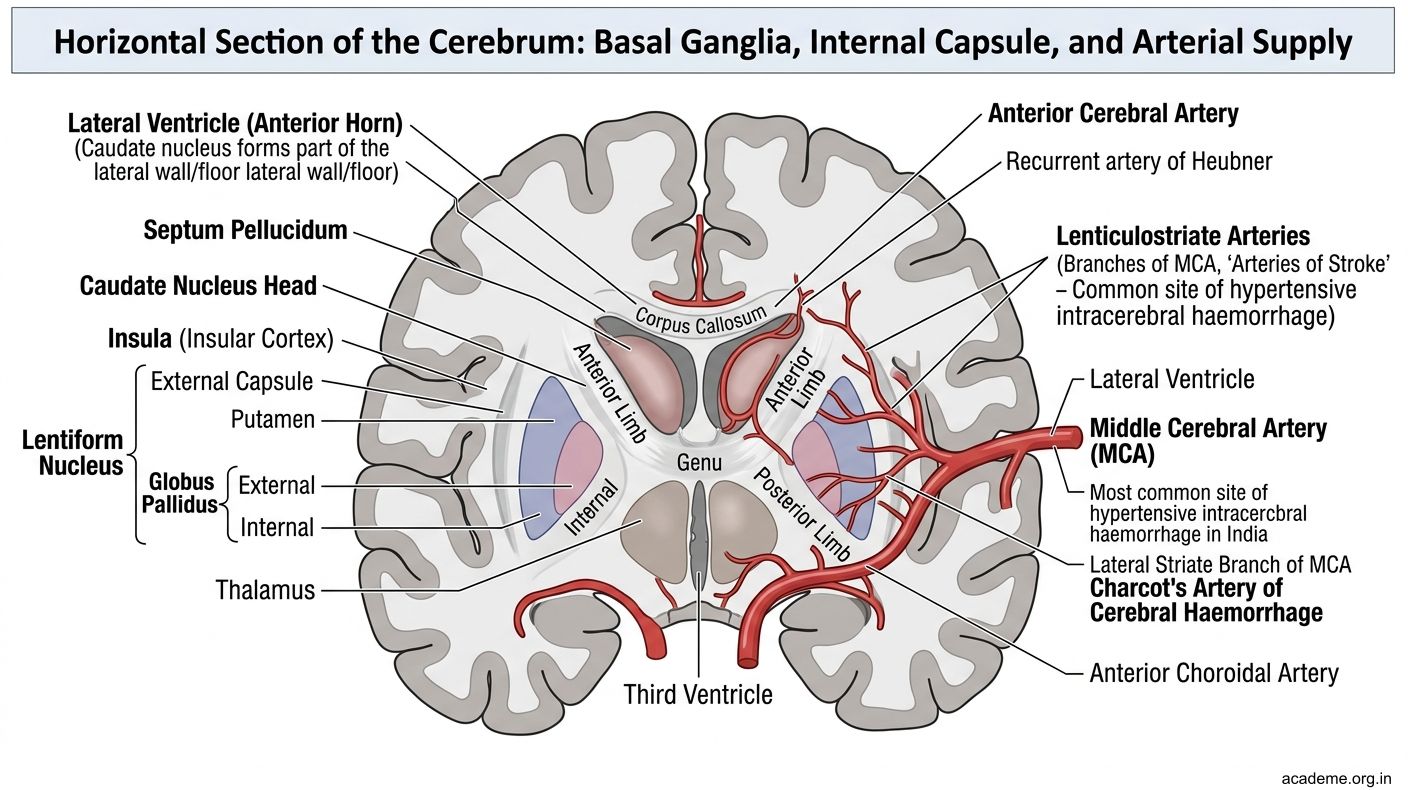
Figure: Internal Capsule: