Page 1 of 4
AN67.1-3 | Muscle histology — SDL Guide
Learning Objectives
- Describe and identify the three types of muscle tissue under the microscope (AN67.1)
- Classify muscle tissue and describe structure-function correlations (AN67.2)
- Describe the ultrastructure of muscle tissue including the sarcomere, T-tubules, and sarcoplasmic reticulum (AN67.3)
- Correlate muscle histology and ultrastructure with clinical conditions common in India
INSTRUCTIONS
The three types of muscle can be identified on a single feature: nucleus location and fibre striation. Make that your starting point on every muscle slide. Skeletal = peripheral nuclei, striated; Cardiac = central nucleus, striated, branched, intercalated discs; Smooth = central nucleus, NO striations, spindle-shaped.
References
- BD Chaurasia's Human Anatomy, Vol. 1 — Muscle Histology (Textbook)
- Junqueira's Basic Histology — Muscle Tissue, 16th Edition (Textbook)
- Robbins Basic Pathology — Chapter on Skeletal Muscle Disease (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 14-year-old boy from Vellore is brought to the paediatric neurology OPD. His mother reports he has difficulty climbing stairs and rising from the floor since age 10. On examination, he has proximal muscle weakness, calf pseudohypertrophy (enlarged calves that are actually weak), and a positive Gowers' sign (uses hands to climb up his own body to stand). Serum creatine kinase (CK) is markedly elevated at 18,000 U/L (normal <200). Genetic testing confirms deletion in the dystrophin gene.
A muscle biopsy from the left vastus lateralis is taken. The pathologist reports: "Variation in fibre size; fibre necrosis with phagocytosis; fibre regeneration (central nuclei); replacement of muscle fibres by fat and fibrous connective tissue."
Why do skeletal muscle fibres normally have peripheral nuclei? What happens when fibres undergo necrosis and regenerate — why do regenerating fibres have central nuclei? What is dystrophin and where in the ultrastructure does it sit?
Muscle histology is the gateway to understanding neuromuscular diseases — among the most challenging and emotionally demanding conditions seen in Indian paediatric neurology.
WHY THIS MATTERS
Muscle histology is directly relevant to clinical practice in India:
- Duchenne muscular dystrophy (DMD) — most common lethal muscular dystrophy in India; muscle biopsy is diagnostic; understanding normal muscle histology is essential for interpretation
- Cardiac muscle histology — basis for understanding myocardial infarction (MI) and cardiomyopathy; ischaemic heart disease is the leading cause of death in urban India
- Smooth muscle tumours — leiomyomas (uterine fibroids) are the most common benign tumour in Indian women; leiomyosarcomas are malignant smooth muscle tumours
- Rhabdomyolysis — crushing injuries (road accidents, marathon running in heat), statin therapy; very high CK; myoglobin damages kidneys; common in India
- NMC 2024 CBME (AN67.1–67.3) — microscopic identification plus ultrastructural knowledge of all three muscle types
RECALL
Before we begin, recall:
- Muscle tissue is derived from mesoderm (skeletal muscle from somites; cardiac from splanchnic mesoderm; smooth muscle from splanchnic mesoderm and neural crest)
- Key property: contractility — ability to shorten when stimulated, converting ATP chemical energy to mechanical work
- Basic mechanism: Actin + Myosin sliding filament model; calcium triggers troponin-tropomyosin complex to expose myosin binding sites on actin; myosin cross-bridges pull actin → sarcomere shortens
- Three types: Skeletal (voluntary, striated), Cardiac (involuntary, striated), Smooth (involuntary, non-striated)
- Terminology: Muscle cell = fibre; Plasma membrane of muscle = sarcolemma; Cytoplasm = sarcoplasm; ER of muscle = sarcoplasmic reticulum (SR)
Part 1: Identifying the Three Muscle Types (AN67.1)
Comparison table — the three muscle types on H&E:
| Feature | Skeletal muscle | Cardiac muscle | Smooth muscle |
|---|---|---|---|
| Shape | Long cylindrical fibres | Short branched cylinders | Spindle-shaped cells |
| Nucleus | MULTIPLE, peripheral (beneath sarcolemma) | 1–2, CENTRAL | 1, CENTRAL (elongated) |
| Striations | Yes (prominent cross-striations) | Yes (cross-striations) | NO striations |
| Branching | No | Yes — fibres branch and interdigitate | No |
| Intercalated discs | Absent | PRESENT — dark transverse lines | Absent |
| Size | Very large (10–100 µm diameter) | Medium (10–15 µm diameter) | Small (2–10 µm diameter) |
| Control | Voluntary (somatic motor neurons) | Involuntary (autonomic + intrinsic) | Involuntary (autonomic) |
| Regeneration | Limited (from satellite cells) | Essentially NONE (cardiomyocytes are terminally differentiated) | Yes (from smooth muscle cells and pericytes) |
On the histology slide — how to identify:
Skeletal muscle:
- Low power: parallel eosinophilic fibres with no branching
- High power: cross-striations (alternating dark A-bands and light I-bands); peripheral flattened nuclei (multiple per fibre)
- Connective tissue: endomysium (around each fibre), perimysium (around fascicles), epimysium (around whole muscle)
Cardiac muscle:
- Low power: branching fibres with intercalated discs (dark transverse bands — the diagnostic feature)
- High power: central oval nucleus; cross-striations; intercalated discs with step-like (staircase) outline
- Note: lipofuscin granules may be seen at the poles of the nucleus (wear-and-tear pigment in ageing hearts)
Smooth muscle:
- Low power: spindle-shaped cells packed together; no striations visible
- Longitudinal section: elongated cells with central elongated nucleus; looks like "cigar-shaped nuclei"
- Transverse section: circular profiles of varying sizes (cells cut at different levels); some show central nucleus, others appear as small circles without nucleus
- No connective tissue sheaths like skeletal muscle; reticular fibres surround individual smooth muscle cells

Figure: Part 1: Identifying the Three Muscle Types (AN67.1)

Figure: Part 1: Identifying the Three Muscle Types (AN67.1)

Figure: On the histology slide — how to identify:
Part 2: Classification and Structure-Function Correlation (AN67.2)
Skeletal Muscle Fibre Types — functional classification:
| Feature | Type I (Slow oxidative) | Type IIa (Fast oxidative) | Type IIb/IIx (Fast glycolytic) |
|---|---|---|---|
| Colour | Red (myoglobin-rich) | Red-pink | White (pale) |
| Speed | Slow twitch | Fast twitch | Fast twitch |
| Fatigue resistance | High (resistant) | Intermediate | Low (fatigable) |
| Energy source | Oxidative phosphorylation | Mixed | Glycolysis (anaerobic) |
| Mitochondria | Many | Intermediate | Few |
| Myoglobin | High | Intermediate | Low |
| Primary use | Posture maintenance, endurance | Mixed activities | Explosive bursts, sprinting |
| Examples | Soleus (postural), diaphragm | Mixed muscles | Gastrocnemius lateral head |
Clinical: Duchenne/Becker MD affect all fibre types (dystrophin lost from all fibres). Inflammatory myopathies (dermatomyositis, common in India) preferentially affect type II fibres. Denervation → all fibres in motor unit atrophy (angular atrophy).
Cardiac muscle — specialised features:
• Intercalated discs (the key cardiac-specific feature): Transverse portion = fascia adherens (mechanical coupling, holds cells together during contraction) + gap junctions at the lateral portions (electrical coupling, allows action potential to spread rapidly through myocardium — "functional syncytium")
• Pace-maker cells (SA node): Modified cardiac muscle cells; fewer myofibrils; spontaneous depolarisation (funny current If); no troponin
• Cardiac muscle has NO ability to regenerate after MI → fibrotic scar
Smooth muscle — distribution and function:
• Vascular smooth muscle — controls vessel diameter (blood pressure regulation); hypertension → hypertrophy
• Visceral (unitary) smooth muscle — GI tract, uterus, ureter, urinary bladder; cells electrically coupled via gap junctions → coordinated peristalsis; uterine smooth muscle (myometrium) hypertrophies massively during pregnancy under oestrogen stimulation
• Multi-unit smooth muscle — iris, ciliary body, piloerector muscles; each cell innervated independently; fine motor control

Figure: Part 2: Classification and Structure-Function Correlation (AN67.2)

Figure: Part 2: Classification and Structure-Function Correlation (AN67.2)
Part 3: Ultrastructure of Muscle (AN67.3)
Sarcomere — the contractile unit of striated muscle (skeletal and cardiac):

Figure: Part 3: Ultrastructure of Muscle (AN67.3)
- Definition: Sarcomere = the unit between two Z-lines; the repeating structural unit of the myofibril
- Bands and zones visible on EM:
- Z-line (Z-disc): Electron-dense disc where actin filaments are anchored; marks the boundary of each sarcomere
- I-band (light): Contains only actin filaments (plus titin); bisected by Z-line; shortens during contraction
- A-band (dark): Contains myosin filaments (thick) + overlapping actin filaments; does NOT change length during contraction (its overall length is constant)
- H-zone: Central pale zone within A-band; contains only myosin (no actin overlap); disappears during full contraction
- M-line: Dark line in centre of H-zone; cross-links myosin filaments
- Titin: Giant elastic protein connecting Z-line to M-line along myosin; acts as a molecular spring; mutations → hypertrophic cardiomyopathy (HCM)
Sarcomere length changes:
• Relaxed: ~2.5 µm; Contracted: ~1.5–2.0 µm; Stretched: up to ~3.6 µm
T-tubules and Sarcoplasmic Reticulum (SR) — the excitation-contraction coupling system:
- T-tubules (Transverse tubules): Invaginations of the sarcolemma that penetrate deep into the muscle fibre; transmit the action potential from the surface to the interior of the fibre rapidly and simultaneously
- Skeletal muscle: T-tubules at the A-I junction (two per sarcomere)
- Cardiac muscle: T-tubules at the Z-line (one per sarcomere, but wider/longer)
- Sarcoplasmic reticulum (SR): Modified smooth ER that surrounds each myofibril; stores calcium ions (Ca²⁺)
- Terminal cisternae (lateral sacs): enlarged ends of SR flanking the T-tubule
- Triad (skeletal muscle): T-tubule + two flanking terminal cisternae of SR = the triad
- Dyad (cardiac muscle): T-tubule + one flanking SR cisterna = the dyad
Excitation-contraction coupling sequence:
1. Action potential arrives at sarcolemma
2. AP travels down T-tubules to fibre interior
3. T-tubule depolarisation activates DHPRs (dihydropyridine receptors — voltage sensors) in T-tubule membrane
4. DHPRs activate RyR1/RyR2 (ryanodine receptors) in SR terminal cisternae → Ca²⁺ released into sarcoplasm
5. Ca²⁺ binds troponin C → conformational change in troponin-tropomyosin complex → myosin binding sites on actin exposed
6. Myosin head (ATPase) hydrolyses ATP → cross-bridge cycle → filament sliding → sarcomere shortens
7. Ca²⁺ pumped back into SR by SERCA (SR Ca²⁺ ATPase) → relaxation
Dystrophin (relevant to hook case):
• Large structural protein linking F-actin (cytoskeleton inside) to dystroglycan complex (outside) → sarcolemma
• Acts as "mechanical shock absorber" protecting sarcolemma from contraction-induced damage
• DMD: dystrophin absent → sarcolemma tears on every contraction → Ca²⁺ floods in → fibre necrosis
• Becker MD: dystrophin reduced/truncated → milder phenotype
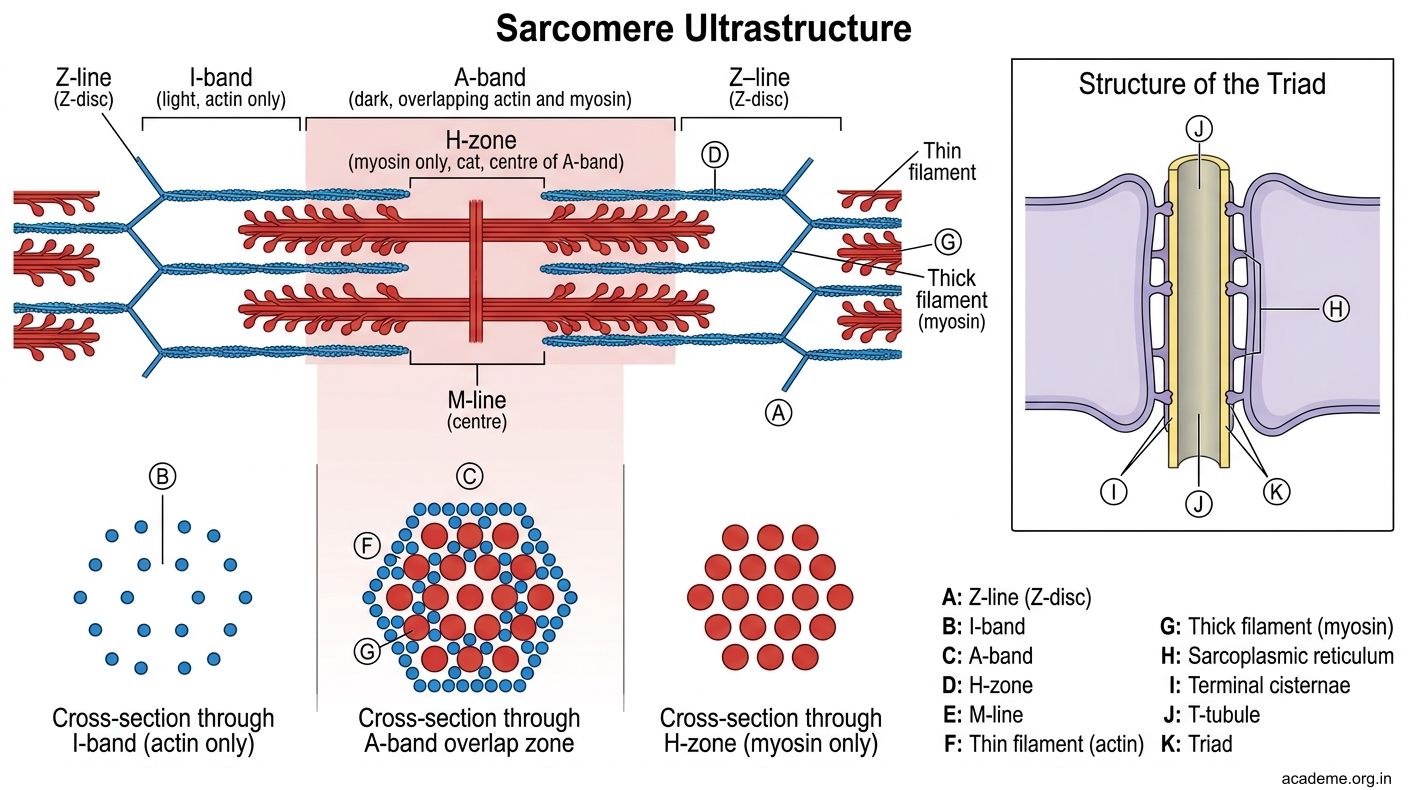
Figure: Part 3: Ultrastructure of Muscle (AN67.3)

Figure: Myocardial Infarction — Cardiac Muscle Cannot Regenerate

Figure: Timeline of MI on histology:

Figure: Timeline of MI on histology:

Figure: Key Takeaways — Muscle Histology (AN67.1–67.3)
SELF-CHECK — : Muscle Histology
On a H&E section, you see branched muscle fibres with a central nucleus and dark transverse bands (intercalated discs) at intervals. This tissue is:
A. Skeletal muscle (longitudinal section)
B. Cardiac muscle
C. Smooth muscle (longitudinal section)
D. Myoepithelial cell layer
Reveal Answer
Answer: B. Cardiac muscle
In the sarcomere, the zone that disappears completely during maximal muscle contraction (because actin and myosin filaments fully overlap) is:
A. A-band
B. Z-line
C. H-zone
D. I-band
Reveal Answer
Answer: C. H-zone
In Duchenne muscular dystrophy, muscle fibres undergo repeated necrosis and regeneration. Regenerating skeletal muscle fibres are identified histologically by:
A. Absence of cross-striations
B. Peripheral nuclei with abundant glycogen
C. Formation of intercalated discs
D. Central nuclei (internalized nuclei) and basophilic sarcoplasm (active protein synthesis)
Reveal Answer
Answer: D. Central nuclei (internalized nuclei) and basophilic sarcoplasm (active protein synthesis)
CLINICAL PEARL
Myocardial Infarction — Cardiac Muscle Cannot Regenerate
Cardiac muscle cells (cardiomyocytes) are terminally differentiated — they do NOT divide after birth. When killed by ischaemia (coronary artery occlusion):
Timeline of MI on histology:
| Time | Gross | Histology |
|---|---|---|
| 0–6 hours | No change visible | No change (EM: mitochondrial swelling) |
| 6–12 hours | Pallor | Wavy fibres at edge; contraction bands (hypercontracted sarcomeres) |
| 12–24 hours | Pallor, coagulation necrosis begins | Pyknotic nuclei, cytoplasmic eosinophilia (hypereosinophilic fibres = "ghost fibres") |
| 24–72 hours | Pallor | Neutrophil infiltration (peak at 48–72h) — acute inflammation |
| 3–7 days | Hyperaemia at margins | Macrophages replacing neutrophils; early granulation tissue |
| 7–21 days | Soft yellow infarct | Granulation tissue (fibroblasts + new capillaries); risk of cardiac rupture |
| >3 weeks | Grey-white scar | Dense collagenous scar (no cardiomyocytes replaced); permanent loss of contractile function |
Clinical relevance in India: Acute MI is the leading cause of death in Indian adults; 60% of MI deaths in India occur before hospitalisation. Troponin I/T (cardiac-specific contractile proteins) are the gold-standard biomarker of myocyte necrosis.
REFLECT
Return to the hook case — the 14-year-old with DMD and muscle biopsy showing "fibre necrosis with phagocytosis; regenerating fibres with central nuclei; replacement by fat and fibrous connective tissue":
- In a normal skeletal muscle fibre, nuclei are at the periphery (beneath the sarcolemma). Why do regenerating fibres have CENTRAL nuclei, and what cell type is responsible for muscle fibre regeneration?
- The biopsy also shows "fibre necrosis with phagocytosis" — which cells are phagocytosing the dead muscle fibres, and what does the ultrastructure of these cells look like?
- In the ultrastructure of dystrophic muscle (DMD), what happens to the sarcolemma during contraction, and why does Ca²⁺ influx lead to fibre necrosis?
- The calves are enlarged but weak (pseudohypertrophy). Looking at the biopsy description "replacement by fat and fibrous connective tissue" — what types of cells are producing the fat and fibrous tissue, and why does this cause apparent enlargement despite weakness?
Discussion: Satellite cells (adult muscle stem cells, normally quiescent under the basal lamina) are activated by necrosis → proliferate → myoblasts → fuse → new muscle fibre with central nuclei (nuclei move to periphery as maturation occurs). Macrophages phagocytose debris (abundant lysosomes, phagosomes). Dystrophin loss → sarcolemmal tears on every contraction → uncontrolled Ca²⁺ influx → protease activation → fibre death. Replacement by adipocytes + fibroblasts → pseudohypertrophy.
KEY TAKEAWAYS
Key Takeaways — Muscle Histology (AN67.1–67.3)
Identification on slide:
• Skeletal: long fibres, peripheral multiple nuclei, striated, NO intercalated discs
• Cardiac: branched, central 1–2 nuclei, striated, INTERCALATED DISCS present (diagnostic)
• Smooth: spindle-shaped, central single nucleus, NO striations
Classification:
• Skeletal type I (red, slow, oxidative, fatigue-resistant) vs IIb (white, fast, glycolytic, fatigable)
• Cardiac — functional syncytium via gap junctions at intercalated discs
• Smooth — unitary (visceral, gap-junction coupled) vs multi-unit (iris, piloerector)
Ultrastructure:
• Sarcomere: Z-A-I-H-M; A-band constant length; H-zone disappears in contraction; I-band and sarcomere shorten
• T-tubules: transmit AP to interior; at A-I junction (skeletal) or Z-line (cardiac)
• SR: Ca²⁺ store; terminal cisternae → triad (skeletal)/dyad (cardiac)
• EC coupling: AP → DHPR → RyR → Ca²⁺ → troponin C → cross-bridge cycle
• Dystrophin: actin → sarcolemma mechanical link; absent in DMD
Clinical:
• DMD: no dystrophin, sarcolemmal tears, Ca²⁺ influx, fibre necrosis; satellite cell regeneration (central nuclei)
• MI: cardiomyocytes cannot regenerate → scar (troponin biomarker)
• Smooth muscle leiomyoma (uterine fibroid) — most common benign tumour in Indian women