Page 1 of 4
AN68.1-3 | Nervous tissue histology — SDL Guide
Learning Objectives
- Describe and identify multipolar and unipolar neurons, ganglia, and peripheral nerve under the microscope (AN68.1)
- Describe the structure-function correlation of the neuron (AN68.2)
- Describe the ultrastructure of nervous tissue including neuronal organelles, myelin sheath, and axonal transport (AN68.3)
- Correlate nervous tissue histology with clinical conditions common in India
INSTRUCTIONS
Nervous tissue histology is the most complex chapter in histology. Focus first on the NEURON: identify its size, the Nissl substance (Nissl bodies) in the soma, and the long axon vs branching dendrites. Then examine supporting cells (neuroglia). Finally, understand the peripheral nerve structure — a nerve is NOT a single axon but a cable of many axons with connective tissue sheaths.
References
- BD Chaurasia's Human Anatomy, Vol. 3 — Neuroanatomy (Histology chapter) (Textbook)
- Junqueira's Basic Histology — Nerve Tissue, 16th Edition (Textbook)
- Kandel & Schwartz's Principles of Neural Science — Chapter on Neuron Structure (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 28-year-old man from Kanchipuram presents to the casualty with a 2-day history of tingling and numbness starting in both feet, rapidly ascending to involve the legs up to the knees. He had a bout of diarrhoea 3 weeks ago (confirmed Campylobacter jejuni infection). On examination, he has profound bilateral lower limb weakness (MRC grade 2/5), absent knee and ankle reflexes (areflexia), and preserved bladder function.
Nerve conduction studies show markedly prolonged distal motor latencies and reduced conduction velocities bilaterally. CSF shows albumino-cytological dissociation (elevated protein 280 mg/dL, cell count normal 4 cells/µL). Diagnosis: Guillain-Barré syndrome (GBS), acute inflammatory demyelinating polyneuropathy (AIDP).
The nerve conduction study abnormality indicates demyelination. What is myelin? Where is it produced? Why does demyelination slow nerve conduction so dramatically?
GBS is the most common acute flaccid paralysis in adults in India (polio is eradicated). Understanding the structure of the peripheral nerve is critical for any physician managing GBS.
WHY THIS MATTERS
Nervous tissue histology is foundational for neurology and neurosurgery — two rapidly growing specialties in India:
- GBS (Guillain-Barré syndrome) — post-infectious immune-mediated demyelinating neuropathy; peaks after Campylobacter, CMV, or Zika infections; understanding myelin structure explains treatment rationale (IVIG, plasmapheresis)
- Leprosy (Hansen's disease) — the most common cause of non-traumatic peripheral neuropathy in India; Mycobacterium leprae specifically infects Schwann cells → demyelination; peripheral nerve histology is diagnostic
- Alzheimer's disease — neurofibrillary tangles (tau protein aggregates in neuronal cytoplasm), senile plaques (amyloid β); axonal transport dysfunction
- Traumatic nerve injuries — road traffic accidents (India: highest RTA burden globally); Wallerian degeneration distal to injury; clinical grading (neurapraxia, axonotmesis, neurotmesis) depends on histological extent of damage
- NMC 2024 CBME (AN68.1–68.3) — microscopic identification plus ultrastructural knowledge of nervous tissue
RECALL
Before we begin, recall:
- Nervous tissue = neurons + neuroglia (supporting cells); derived from neuroectoderm (neural tube and neural crest)
- Neurons: Cannot divide (except olfactory neurons and hippocampal neurons); transmit electrical signals; highly metabolically active (25% of body's oxygen consumption)
- Neuroglia (CNS): Astrocytes, oligodendrocytes, microglia, ependymal cells
- Neuroglia (PNS): Schwann cells (myelinate peripheral axons), satellite cells (in dorsal root ganglia and autonomic ganglia)
- Myelin: Lipid-protein insulating sheath around axons; formed by oligodendrocytes (CNS) and Schwann cells (PNS); speeds up AP conduction by saltatory conduction at Nodes of Ranvier
Part 1: Identifying Neurons and Nerve Structures (AN68.1)
Neuron types — identification on histology slides:
Multipolar neuron (motor neuron — anterior horn cell):
• Large cell body (soma/perikaryon)
• Multiple dendrites radiating from soma (multiple poles)
• One long axon
• Nucleus: large, pale (euchromatic — actively transcribing), prominent nucleolus
• Cytoplasm: contains Nissl substance (rough ER + polyribosomes → stains blue with Nissl stain; cresyl violet or toluidine blue)
• Location: anterior horn of spinal cord, motor cranial nerve nuclei, autonomic ganglia
• On slide: large cell with prominent nucleus and nucleolus; surrounding smaller glial cells (satellite cells in ganglia)
Unipolar neuron (pseudounipolar sensory neuron):
• Actually pseudounipolar — one process that divides into central and peripheral branch
• Round cell body; one process (not visible as a long process in ganglia sections)
• Location: dorsal root ganglia (spinal ganglia), trigeminal ganglia, geniculate ganglion
• On slide: in dorsal root ganglion — round cells of varying sizes, each surrounded by a ring of satellite cells (capsule cells); between them: connective tissue
Ganglia — peripheral collections of neuron cell bodies:
• Spinal (dorsal root) ganglion: Pseudounipolar neurons + satellite cells; capsule of connective tissue; between neurons = myelinated nerve fibres
• Autonomic ganglion: Multipolar neurons; satellite cells less complete; connective tissue framework; post-ganglionic autonomic fibres pass through
Peripheral nerve (e.g., sciatic nerve cross-section):
• Multiple fascicles (bundles of nerve fibres) within a connective tissue framework
• Endoneurium: Fine reticular fibres + fibroblasts surrounding each individual axon
• Perineurium: Concentric layers of flattened perineurial cells (with tight junctions → blood-nerve barrier) surrounding each fascicle
• Epineurium: Dense irregular connective tissue surrounding the entire nerve; contains blood vessels (vasa nervorum), lymphatics, fat
• Inside a fascicle (high power): myelinated fibres (pale rings of myelin around central axon — myelin shrinks and appears as clear space in H&E), Schwann cell nuclei flattened at periphery; also unmyelinated fibres (grouped Remak bundles — axons embedded in a trough in Schwann cell cytoplasm without myelin)
Node of Ranvier:
• Gap in the myelin sheath between adjacent Schwann cells (PNS) or oligodendrocyte processes (CNS)
• Site of AP generation during saltatory conduction
• Each Schwann cell myelinates one internode (one segment between two nodes)

Figure: Part 1: Identifying Neurons and Nerve Structures (AN68.1)
Part 2: Structure-Function Correlation of the Neuron (AN68.2)
Neuronal compartments and their functional roles:

Figure: Part 2: Structure-Function Correlation of the Neuron (AN68.2)
Cell body (soma/perikaryon) — integrating and metabolic centre:
• Contains all synthetic machinery: rough ER (Nissl substance), Golgi apparatus, mitochondria, cytoskeleton
• Receives thousands of synaptic inputs on dendritic spines and soma
• Protein synthesis here (axon cannot synthesise proteins — no ribosomes in axon)
• Chromatolysis: dissolution of Nissl substance after axonal injury → cell body swells, nucleus moves peripherally; sign of neuronal "distress" and attempt at regeneration
Dendrites — receptive surface:
• Short branching processes that receive afferent signals
• Contain Nissl substance (RER) → can synthesise proteins locally
• Dendritic spines: small protrusions on dendrites = sites of excitatory synapses; spine morphology changes with learning (synaptic plasticity); loss of spines = Alzheimer's disease, depression
Axon (nerve fibre) — the transmitter:
• Single process; arises from the axon hillock (initial segment — site of AP generation, highest density of voltage-gated Na⁺ channels)
• Contains neurofilaments and microtubules (no ribosomes)
• Covered by myelin sheath (in myelinated fibres)
• Ends in terminal boutons (axon terminals → synaptic knobs)
Synapse — the functional unit of neural communication:
• Chemical synapse: Pre-synaptic terminal bouton → synaptic cleft (20 nm) → post-synaptic membrane
• Pre-synaptic terminal: many mitochondria (ATP for neurotransmitter synthesis + vesicle recycling); synaptic vesicles (store neurotransmitter)
• Synaptic vesicle types: small clear vesicles (ACh, glutamate, GABA); large dense-core vesicles (noradrenaline, peptides)
• Signal transmission: AP → Ca²⁺ influx (voltage-gated Ca²⁺ channels) → vesicle fusion → neurotransmitter release into synaptic cleft → binds post-synaptic receptors
Neurotransmitter-receptor pairs (selected clinical relevance):
| NT | Receptor | Pharmacological relevance in India |
|---|---|---|
| Acetylcholine | Nicotinic (nm junction), muscarinic (ANS) | Organophosphate poisoning (common in India — agricultural pesticides) → inhibits AChE → excess ACh → SLUDGE |
| GABA | GABA-A (ionotropic, Cl⁻), GABA-B | Benzodiazepines and alcohol enhance GABA-A → CNS depression; withdrawal → seizures |
| Dopamine | D1, D2 (striatum, limbic) | Parkinson's disease (dopamine deficiency), antipsychotics (D2 blockers) |
| Glutamate | NMDA, AMPA | Learning (LTP), excitotoxicity in stroke/TBI → NMDA receptor antagonists (memantine) |
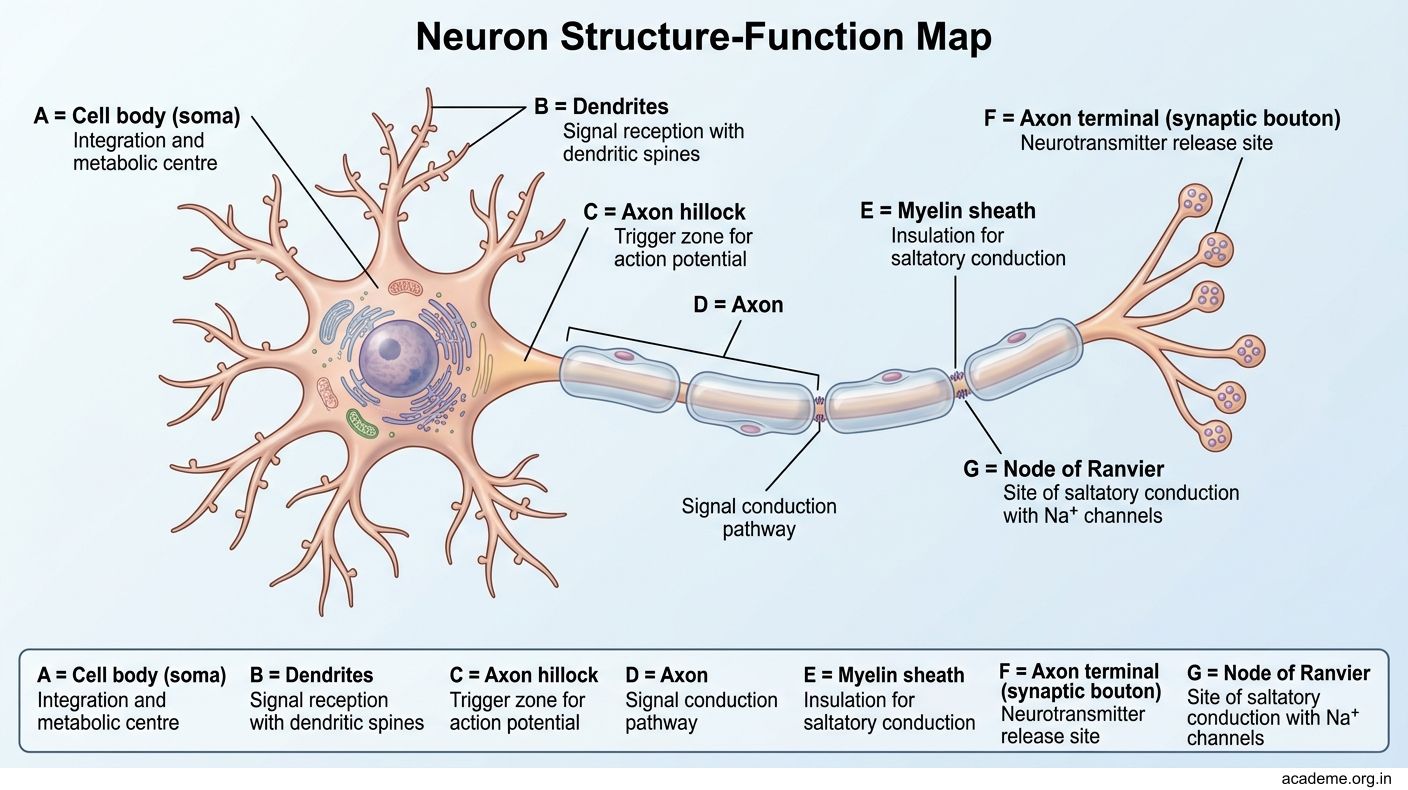
Figure: Part 2: Structure-Function Correlation of the Neuron (AN68.2)
Part 3: Ultrastructure of Nervous Tissue (AN68.3)
Ultrastructure of the neuron — key organelles:
- Nissl substance (rough ER + free polyribosomes): Most prominent in large motor neurons (anterior horn cells); absent in the axon hillock and axon; function: protein synthesis (neurotransmitter synthesising enzymes, membrane proteins, cytoskeletal proteins)
- Golgi apparatus: Extensive in neurons; processes and packages proteins for axonal transport; post-translational modifications
- Neurofilaments (intermediate filaments): Most abundant cytoskeletal element in axons; maintain axon diameter; phosphorylation determines axon calibre and CV; aggregation in Alzheimer's disease (neurofibrillary tangles = hyperphosphorylated tau protein)
- Microtubules: Run along axon length; rails for axonal transport; assembled from α/β-tubulin
- Lipofuscin granules: Yellow-brown residual bodies (undigested lysosomal material); accumulate with age in neurons; "wear and tear" pigment; prominent in cardiac muscle and neurons of ageing patients
Axonal transport — critical concept:
• Axon cannot synthesise proteins; all proteins made in soma must be transported down the axon
• Anterograde transport (soma → axon terminal):
- Fast anterograde (200–400 mm/day): Synaptic vesicles, membrane proteins, mitochondria; motor: kinesin (walks toward + end of microtubule)
- Slow anterograde (0.1–4 mm/day): Cytoskeletal proteins (neurofilaments, tubulin)
• Retrograde transport (axon terminal → soma): Nerve growth factors (NGF), viruses (herpes, rabies, polio), tetanus toxin; motor: dynein (walks toward − end = soma)
• Clinical: Herpes simplex virus travels retrogradely from skin → sensory ganglion (dorsal root ganglion) → remains latent; reactivation travels anterogradely → skin vesicles (herpes zoster = shingles)
Myelin sheath ultrastructure:
• PNS myelin (Schwann cell): Each Schwann cell wraps ONE axon segment; spiral wrapping of Schwann cell plasma membrane → compacted myelin (major dense lines where inner leaflets fuse; intraperiod lines where outer leaflets fuse)
• CNS myelin (oligodendrocyte): One oligodendrocyte myelinates up to 50 axons (multiple axon segments)
• Composition: 70% lipid (cholesterol, sphingomyelin, galactocerebroside) + 30% protein (MBP — myelin basic protein, PLP — proteolipid protein, MAG)
• Schmidt-Lantermann incisures: Funnel-shaped clefts in PNS myelin; residual Schwann cell cytoplasm channels
Wallerian degeneration — axon injury response:
• After axon is cut/crushed: the axon and myelin DISTAL to the injury degenerate → Schwann cells proliferate, phagocytose debris → Bands of Büngner (Schwann cell tubes) guide regenerating axon
• Axon regenerates at 1–4 mm/day
• CNS axons cannot regenerate (no Schwann cells; CNS has inhibitory myelin proteins — Nogo, MAG, OMgp; no Bands of Büngner)
Neuroglia — ultrastructure and function:
| Glial cell | Identifying features (EM/LM) | Function | Clinical |
|---|---|---|---|
| Astrocyte (fibrous/protoplasmic) | Star-shaped; GFAP-positive; end-feet on capillaries; EM: filament bundles | Blood-brain barrier (BBB) maintenance, K⁺ buffering, neurotransmitter uptake | Reactive gliosis (scar after CNS injury); astrocytoma |
| Oligodendrocyte | Small round nucleus; few cytoplasm; EM: myelin loops | CNS myelin formation | MS (immune attack on oligodendrocyte myelin); PML (JC virus attacks oligodendrocytes) |
| Microglia | Small, elongated nucleus; many processes; EM: lysosomes | CNS macrophage; activated in neuroinflammation | HIV encephalitis (microglial nodules); Alzheimer's neuroinflammation |
| Schwann cell (PNS) | Elongated nucleus; surrounds axon; EM: myelin spiral layers | PNS myelin + trophic support | Schwannoma (benign tumour); GBS (autoimmune attack on myelin); leprosy (M. leprae infects Schwann cells) |

Figure: Neurotransmitter-receptor pairs (selected clinical relevance):

Figure: Part 3: Ultrastructure of Nervous Tissue (AN68.3)

Figure: Neuroglia — ultrastructure and function:

Figure: Leprosy — Schwann Cell Invasion and Peripheral Neuropathy

Figure: Types and histology:

Figure: Key Takeaways — Nervous Tissue Histology (AN68.1–68.3)
SELF-CHECK — : Nervous Tissue
On a histology section of a spinal ganglion (dorsal root ganglion), you see round cells of varying sizes, each surrounded by a ring of flattened cells. The surrounding flattened cells are:
A. Oligodendrocytes
B. Satellite (capsule) cells
C. Microglia
D. Astrocytes
Reveal Answer
Answer: B. Satellite (capsule) cells
In Guillain-Barré syndrome, autoantibodies attack the myelin sheath of peripheral nerves. The cells that produce peripheral nerve myelin and are targeted in AIDP are:
A. Oligodendrocytes
B. Astrocytes
C. Schwann cells
D. Microglial cells
Reveal Answer
Answer: C. Schwann cells
The tetanus toxin (produced by Clostridium tetani at a wound site) travels from the peripheral nerve terminal to the spinal cord via which axonal transport mechanism?
A. Retrograde fast axonal transport (dynein motor along microtubules)
B. Anterograde fast axonal transport (kinesin motor)
C. Slow anterograde transport (cytoskeletal proteins)
D. Passive diffusion through the axoplasm
Reveal Answer
Answer: A. Retrograde fast axonal transport (dynein motor along microtubules)
CLINICAL PEARL
Leprosy — Schwann Cell Invasion and Peripheral Neuropathy
Leprosy (Hansen's disease) is caused by Mycobacterium leprae — the only known bacterium that infects peripheral nerves. India accounts for ~55% of global leprosy burden.
Why M. leprae targets Schwann cells:
• M. leprae binds to α-dystroglycan on the Schwann cell surface via its G domain of laminin-α2 (LAM2)
• Enters Schwann cells → demyelination (PGL-1 antigen triggers autoimmune response) → axonal degeneration
Types and histology:
| Type | Nerve histology | Clinical |
|---|---|---|
| Tuberculoid leprosy (TT) | Epithelioid granulomas WITHIN the nerve; severe fibrosis; few bacilli (paucibacillary) | Thickened nerve (palpable), anaesthesia in defined patch, few lesions |
| Lepromatous leprosy (LL) | Schwann cells packed with M. leprae (Virchow cells = foam cells); minimal host response (multibacillary) | Diffuse nerve thickening; loss of sensation (glove-and-stocking); leonine facies |
Palpable peripheral nerves = DIAGNOSTIC of leprosy in India:
• Great auricular nerve (behind sternomastoid)
• Ulnar nerve (behind medial epicondyle)
• Common peroneal nerve (around fibular head)
• Radial cutaneous nerve (wrist)
Treatment: Multi-drug therapy (rifampicin + dapsone + clofazimine). Reactions: Type 1 (reversal, cell-mediated) and Type 2 (ENL, immune complex) — treated with corticosteroids.
REFLECT
Return to the hook case — the GBS patient with post-Campylobacter demyelinating polyneuropathy:
- The nerve conduction study shows prolonged distal motor latencies and reduced conduction velocities. Based on the ultrastructure of myelin and saltatory conduction, explain WHY demyelination slows conduction velocity.
- The attack is "acute inflammatory demyelinating" — which cells produce peripheral nerve myelin (name them), and what do they look like on EM (describe their key ultrastructural feature)?
- CSF shows elevated protein but normal cell count (albumino-cytological dissociation). Proteins leak into the CSF because inflammation at the nerve roots breaks down the blood-nerve barrier. Which cells form the blood-nerve barrier (perineurial cells or astrocytes in the PNS), and what junctions seal this barrier?
- After successful treatment and recovery, peripheral nerve myelin can regenerate (unlike CNS). What are the "Bands of Büngner," and which cells form them as a scaffold for regenerating axons?
Discussion: Myelin insulates the axon and enables saltatory conduction (AP jumps between Nodes of Ranvier → much faster than continuous conduction). Without myelin, AP must conduct continuously along the entire axon membrane → very slow. Schwann cells produce PNS myelin; EM shows spiral layered plasma membrane wrapping (major dense lines + intraperiod lines). Blood-nerve barrier formed by perineurial cells with tight junctions. Bands of Büngner = proliferating Schwann cells filling the endoneurial tube after Wallerian degeneration → guide regenerating axon.
KEY TAKEAWAYS
Key Takeaways — Nervous Tissue Histology (AN68.1–68.3)
Identifying structures on slide:
• Multipolar neuron (anterior horn): large cell, pale nucleus, prominent nucleolus, Nissl substance (blue granules with Nissl stain)
• Pseudounipolar neuron in DRG: round cells of varying sizes, each with satellite cell ring
• Peripheral nerve cross-section: fascicles within epineurium; perineurium around each fascicle; myelinated axons = clear rings (myelin shrinkage) with axon inside; Schwann cell nuclei at periphery
Structure-function:
• Soma = synthesis centre; dendrites = receptive; axon = transmitter; synapse = communication unit
• Nissl substance (RER + ribosomes) — absent in axon; chromatolysis after injury
• Synaptic vesicles: small clear (fast NT: ACh, Glu, GABA); large dense-core (peptides, NA)
Ultrastructure:
• Axonal transport: anterograde (kinesin, fast 400 mm/day for vesicles); retrograde (dynein — viruses, toxins, NGF travel this route)
• Myelin (PNS): Schwann cell spiral wrap; one cell per internode; Nodes of Ranvier between
• Myelin (CNS): oligodendrocyte; one cell for up to 50 axon segments
• Wallerian degeneration: axon + myelin distal to injury degrade; Bands of Büngner guide regeneration (PNS only)
Clinical:
• GBS: post-infectious autoimmune demyelination of PNS (Schwann cells) → flaccid paralysis
• Leprosy: M. leprae infects Schwann cells → palpable thickened nerves, anaesthesia
• Tetanus toxin: retrograde axonal transport (dynein)
• Alzheimer's: neurofibrillary tangles (tau), amyloid plaques, dendritic spine loss