Page 1 of 4
AN79.1-6 | 3rd to 8th week of development — SDL Guide
Learning Objectives
- Describe the formation and fate of the primitive streak (AN79.1)
- Describe the formation and fate of the notochord (AN79.2)
- Describe the process of neurulation and neural tube formation (AN79.3)
- Describe the development of somites and intra-embryonic coelom (AN79.4)
- Explain the embryological basis of congenital malformations, nucleus pulposus, sacrococcygeal teratomas, and neural tube defects (AN79.5)
INSTRUCTIONS
This module covers the most critical embryological period — the 3rd to 8th weeks when all major organ systems are laid down. Study with diagrams of the trilaminar disc and neural tube formation. Most congenital defects originate in this period.
References
- Inderbir Singh's Human Embryology, 11th Ed. — Chapters 4–6 (Textbook)
- Langman's Medical Embryology, 14th Ed. — Chapters 3–5 (Textbook)
- T.W. Sadler's Langman's Medical Embryology — Gastrulation and Neurulation (Textbook)
Version 1.0 | Academe Content Engine v2, MGMCRI Department of Anatomy
CLINICAL SCENARIO
A 26-year-old primigravida from Chennai presents at 20 weeks of gestation for a routine anomaly scan. The sonologist reports: "A large posterior midline mass at the lumbosacral region measuring 6×5 cm, with mixed solid and cystic components, extending externally. Neural tube appears open at the lumbosacral level. Fetal head shows a 'lemon sign' on axial view (anterior scalloping of frontal bones) and a 'banana sign' (cerebellar herniation)."
The obstetrician explains to the family: "Your baby has a myelomeningocele — a neural tube defect. This occurred during the 3rd–4th week of development when the neural tube failed to close."
What is the neural tube? How does it form? Why does this defect occur in the lumbosacral region? What is the significance of the lemon and banana signs?
This module traces the events of the 3rd to 8th weeks — the period when a simple disc of cells transforms into a recognisable embryo with all organ systems initiated.
WHY THIS MATTERS
The 3rd–8th week embryology is directly relevant to Indian clinical practice:
- Neural tube defects (NTDs) — India has one of the highest NTD burdens globally; spina bifida and anencephaly are detected on routine anomaly scans; folic acid supplementation (0.4–5 mg/day periconceptionally) prevents ~70% of NTDs
- Sacrococcygeal teratoma — a neonatal tumour arising from remnants of the primitive streak; diagnosed on antenatal ultrasound; requires urgent surgical excision after birth
- Nucleus pulposus — the central jelly-like core of intervertebral discs is a remnant of the notochord; herniation (disc prolapse — "slipped disc") is extremely common in India, causing sciatica; understanding its embryological origin explains its tissue properties
- NMC 2024 CBME — AN79.1–79.5 are core competencies; questions on primitive streak, notochord, neurulation, and congenital anomalies feature in university examinations and NEET-PG
- Folic acid policy — Indian government's supplementation programme is based on understanding the embryological timing of NTDs
RECALL
Before we begin, recall:
- At the end of the 2nd week, the embryo is a bilaminar disc consisting of two layers: epiblast (dorsal) and hypoblast (ventral), embedded in the endometrium
- The amniotic cavity lies above the epiblast; the primary yolk sac (exocoelomic cavity) lies below the hypoblast
- The cranial end of the embryo develops faster than the caudal end (cephalocaudal gradient)
- Teratogens are agents that cause congenital abnormalities; they are most dangerous during the 3rd–8th weeks (the critical period of organogenesis)
Part 1: Primitive Streak — Formation and Fate (AN79.1)
The Primitive Streak

Figure: Part 1: Primitive Streak — Formation and Fate (AN79.1)
Formation (Day 14–15, 3rd week):
The primitive streak appears as a thickening of the epiblast in the caudal midline of the embryonic disc. It is the first landmark of the 3rd week and establishes the body axes:
• Cranial–caudal axis (head–tail direction)
• Left–right axis (bilateral symmetry)
• Dorsal–ventral axis
Structure:
• Primitive streak — midline thickening in caudal epiblast
• Primitive node (Hensen's node) — cranial thickening at the cranial end of the streak; the organiser of the entire embryo
• Primitive groove — central depression along the streak through which cells invaginate
• Primitive pit — depression at the centre of the primitive node
Gastrulation — The Process:
Cells from the epiblast migrate toward the primitive streak, ingress through the primitive groove, and spread laterally and cranially between the epiblast (ectoderm) and hypoblast (endoderm) to form the intraembryonic mesoderm:
| Layer | Origin | Future |
|---|---|---|
| Ectoderm | Epiblast cells remaining on surface | Skin, nervous system, sense organs |
| Mesoderm | Epiblast cells that migrate through the streak | Muscles, skeleton, connective tissue, cardiovascular system, kidneys, gonads |
| Endoderm | Epiblast cells that replace the hypoblast | Gut epithelium, liver, pancreas, lungs, bladder lining |
Thus, gastrulation converts the bilaminar disc → trilaminar disc (ectoderm + mesoderm + endoderm).
Fate of the Primitive Streak:
• The streak regresses caudally as gastrulation proceeds (3rd–4th weeks)
• By the 4th week, only a small caudal remnant remains (Müller's tubercle region)
• By the end of the 4th week, the primitive streak disappears entirely
Clinical Significance:
• Sacrococcygeal teratoma — if the primitive streak fails to regress completely, remnant pluripotent cells persist in the presacral/sacrococcygeal region → form a teratoma (tumour containing derivatives of all three germ layers: hair, teeth, neural tissue, cartilage)
- Most common solid tumour in neonates (1 in 35,000 births)
- Diagnosed on antenatal ultrasound as a large sacrococcygeal mass
- 80% benign at birth; becomes malignant if not excised early → urgent surgical excision in the neonatal period
• Situs inversus — Hensen's node controls L–R asymmetry via cilia-driven nodal flow; defects → situs inversus (heart and liver on opposite sides); associated with Kartagener syndrome (immotile cilia)
• Conjoined twins — incomplete separation of the primitive streak in identical twins
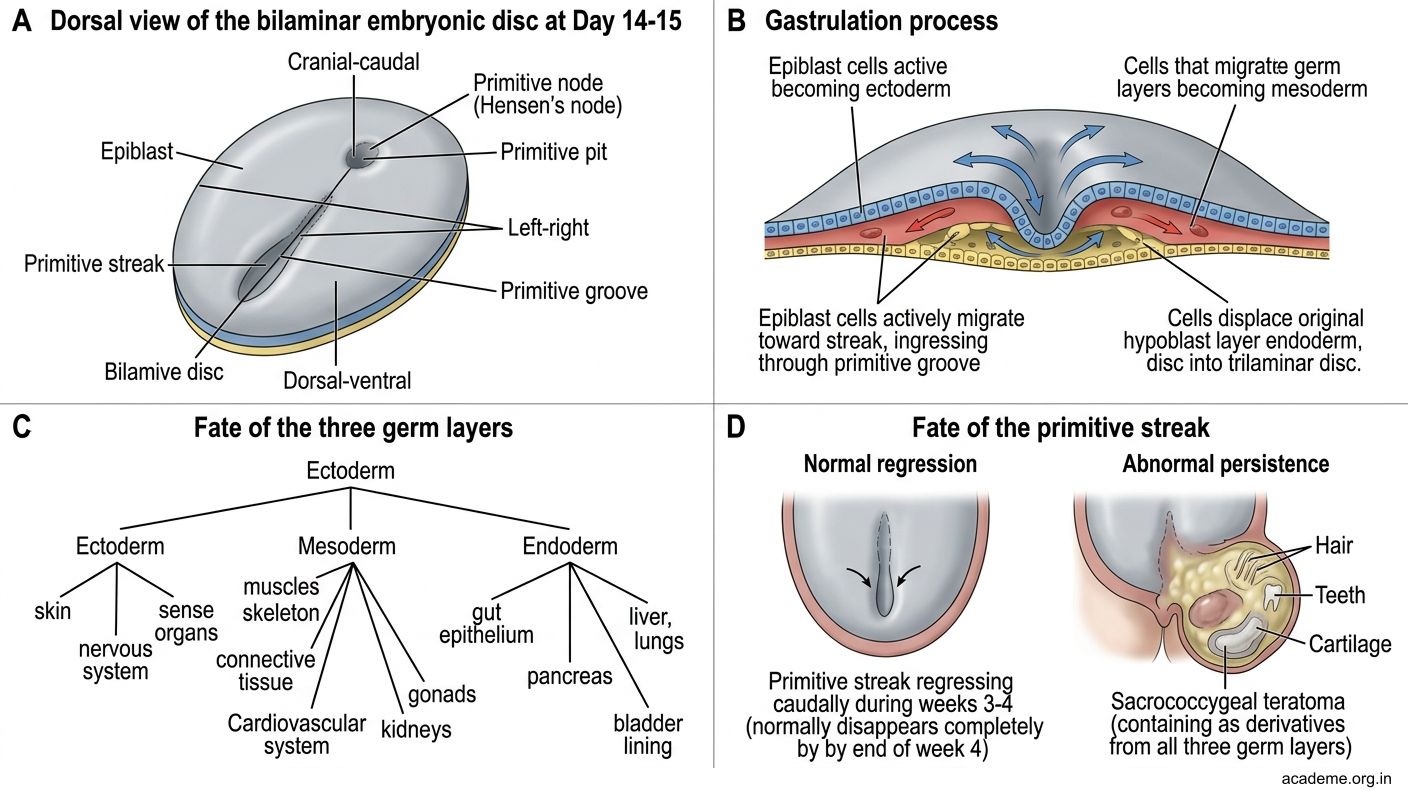
Figure: Part 1: Primitive Streak — Formation and Fate (AN79.1)
Part 2: Notochord — Formation and Fate (AN79.2)
The Notochord

Figure: Part 2: Notochord — Formation and Fate (AN79.2)
Formation (Days 16–22, 3rd week):
• Cells from the primitive node migrate cranially in the midline (between ectoderm and endoderm) to form the notochordal process
• The notochordal process initially forms a hollow tube, then becomes solid → the definitive notochord
• The notochord extends from the oropharyngeal membrane (cranially) to the cloacal membrane (caudally)
Functions of the Notochord:
1. Defines the central axis — establishes the longitudinal axis of the embryo; vertebral column forms around it
2. Induces neurulation — induces the overlying ectoderm to form the neural plate (a critical inductive signal)
3. Determines vertebral body formation — the sclerotome (from somites) condenses around the notochord to form vertebral bodies; the notochord becomes enclosed within the vertebral bodies
Fate of the Notochord:
• The notochord is progressively surrounded and incorporated into the developing vertebral column
• Within each vertebral body, the notochord degenerates completely
• At each intervertebral disc, the notochord persists and expands → forms the nucleus pulposus (the gelatinous core of the intervertebral disc)
• The nucleus pulposus is surrounded by the annulus fibrosus (from sclerotome mesenchyme)
Clinical Significance:
• Disc prolapse (Herniated Nucleus Pulposus — HNP / "slipped disc"):
- The nucleus pulposus is the notochordal remnant; it has a high water content (80% water at birth, decreasing with age)
- With aging and mechanical stress → the annulus fibrosus develops radial tears → nucleus pulposus herniates posterolaterally
- Compresses nerve roots (lumbar L4–L5, L5–S1 most common) → sciatica (radiating leg pain)
- Extremely common in India: lumbar disc prolapse causes low back pain + sciatica
- L4–L5 disc prolapse → L5 root compression → foot drop + sensory loss on dorsum of foot
- L5–S1 disc prolapse → S1 root compression → absent ankle jerk + sensory loss on sole
• Chordoma — rare malignant tumour arising from notochordal remnants; occurs at the clivus (base of skull) or sacrococcygeal region (the two ends of the notochordal axis where remnants may persist)
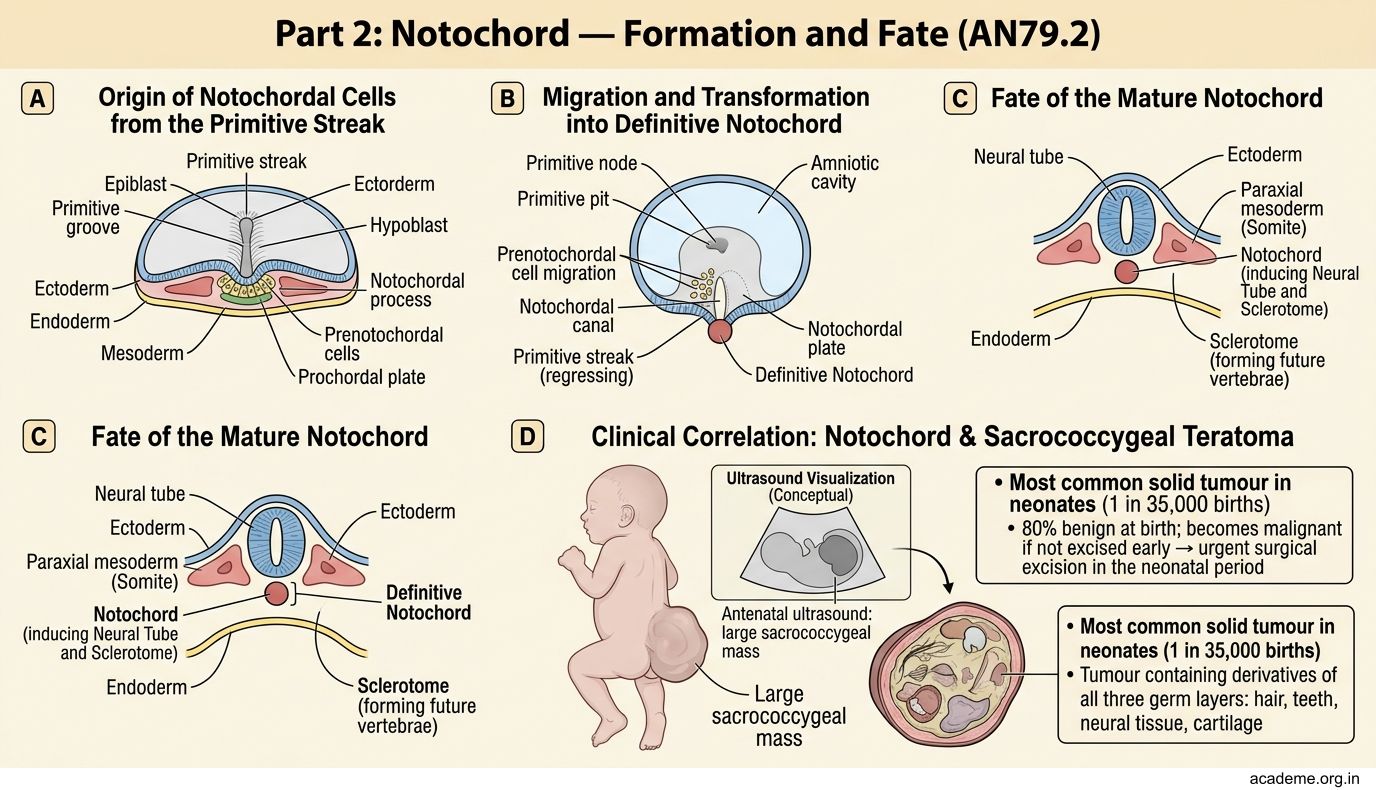
Figure: Part 2: Notochord — Formation and Fate (AN79.2)
Part 3: Neurulation — Formation of the Neural Tube (AN79.3)
Neurulation (3rd–4th weeks)

Figure: Part 3: Neurulation — Formation of the Neural Tube (AN79.3)
Neurulation is the process by which the neural plate folds to form the neural tube — the precursor of the brain and spinal cord.
Steps:
1. Neural plate induction (Day 18): The notochord induces the overlying ectoderm → thickens to form the neural plate (a flat sheet of neuroectoderm, widest cranially)
2. Neural folds (Day 20–22): The lateral edges of the neural plate elevate as neural folds; the central region deepens into the neural groove
3. Neural tube closure (Days 22–26): The neural folds fuse in the midline, starting at the mid-cervical region (future C3–C4) and proceeding simultaneously cranially and caudally (like a zipper)
- Anterior (cranial) neuropore closes on Day 25
- Posterior (caudal) neuropore closes on Day 27
4. Neural crest cells migrate away from the neural folds as fusion occurs
Neural Tube → CNS:
| Region | Derivative |
|---|---|
| Cranial neural tube | Brain (3 primary vesicles: prosencephalon, mesencephalon, rhombencephalon) |
| Caudal neural tube | Spinal cord |
Neural Crest Cells (the 4th germ layer):
• Derived from the neural folds; migrate extensively throughout the embryo
• Form: Dorsal root ganglia, autonomic ganglia, Schwann cells, melanocytes, craniofacial cartilage and bone, adrenal medulla (chromaffin cells), C-cells of thyroid, odontoblasts
Neural Tube Defects (NTDs) — Clinical Significance (AN79.5):
| Type | Mechanism | Clinical Presentation |
|---|---|---|
| Anencephaly | Anterior neuropore fails to close (Day 25) | Absence of cranial vault and brain; incompatible with life; 50% detected by elevated AFP + ultrasound |
| Spina bifida occulta | Posterior arch of a vertebra (usually L5/S1) fails to close; spinal cord normal | Dimple/tuft of hair over lumbosacral region; mostly asymptomatic |
| Meningocele | Posterior neuropore fails to close; meninges herniate through bony defect | Midline cystic swelling, neural elements intact inside canal; better prognosis |
| Myelomeningocele | Posterior neuropore fails to close; meninges + spinal cord herniate through defect | Exposed neural tissue/sac; leads to paralysis below level, bladder/bowel dysfunction, Chiari II malformation |
| Encephalocele | Defect in cranial vault; brain + meninges herniate | Midline posterior skull mass; may cause hydrocephalus |
Chiari II Malformation (Arnold-Chiari):
• Accompanies most myelomeningoceles
• Cerebellar tonsils herniate through foramen magnum → CSF flow obstruction → hydrocephalus
• "Lemon sign" on US = frontal bone scalloping from CSF pressure; "Banana sign" = cerebellar herniation
Prevention of NTDs:
• Periconceptional folic acid (0.4–5 mg/day) — reduces NTDs by 70%; folic acid is required for neural tube closure
• All women planning pregnancy in India should begin folic acid ≥1 month before conception and continue through the 1st trimester
• NTD prevalence in India: ~3–4 per 1,000 births (higher than Western countries) due to inadequate folic acid intake
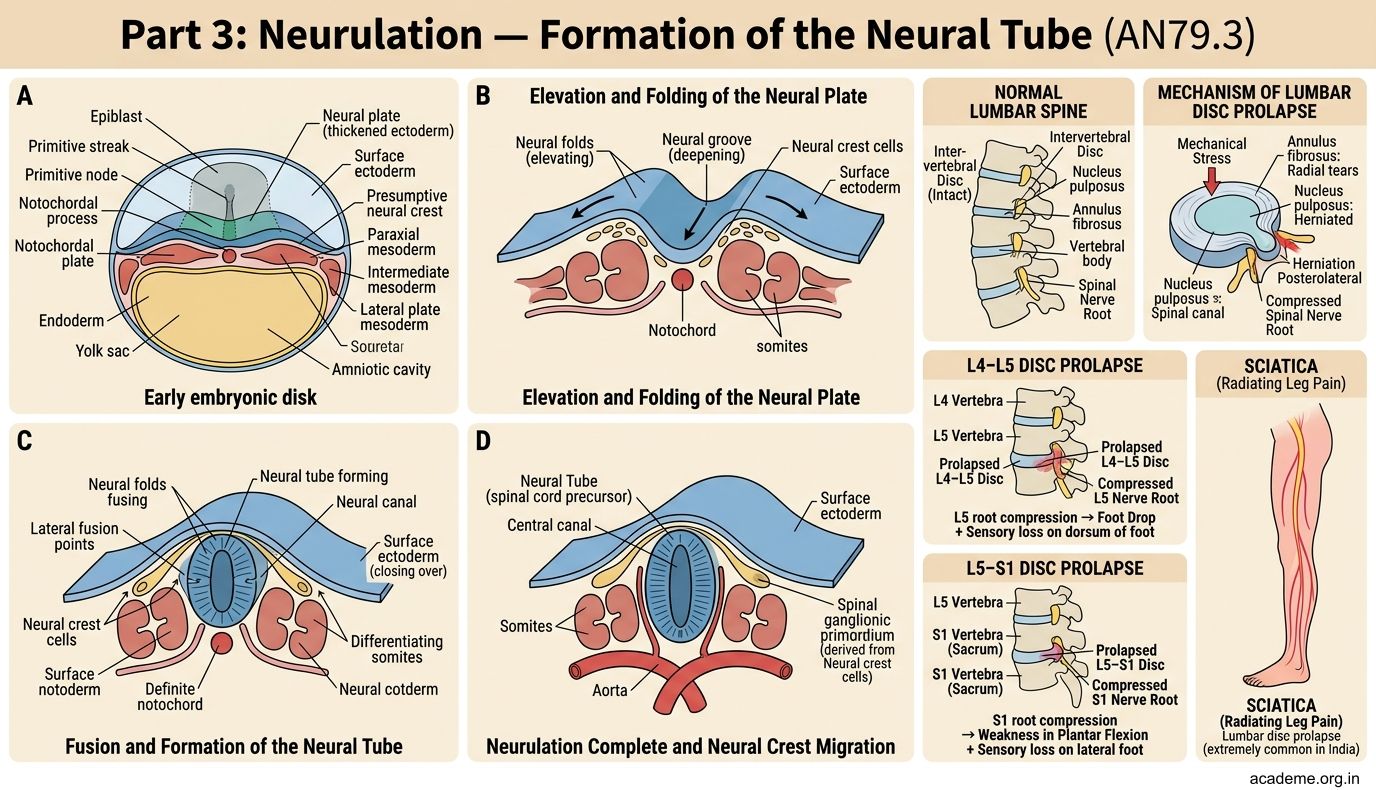
Figure: Part 3: Neurulation — Formation of the Neural Tube (AN79.3)

Figure: Neural Tube → CNS:
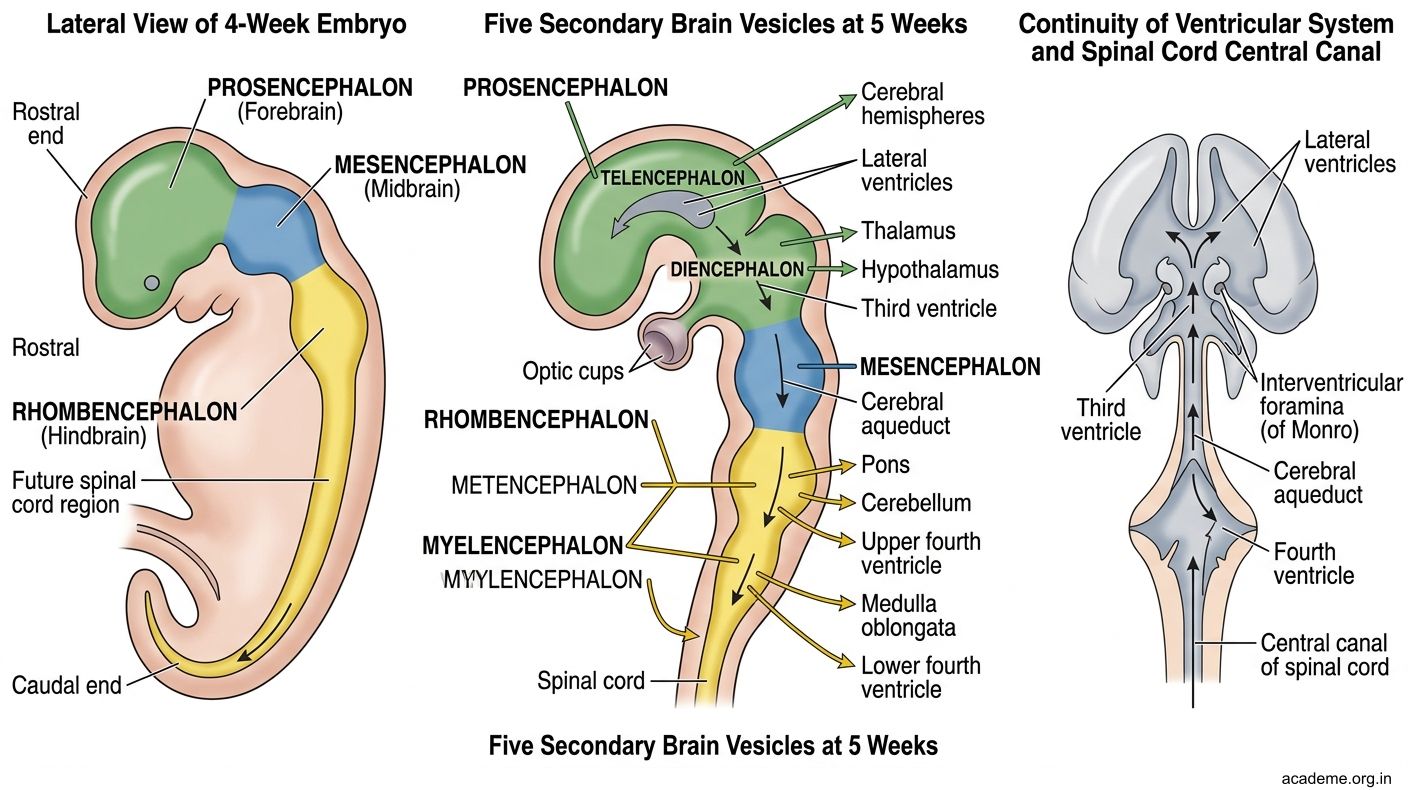
Figure: Neural Tube → CNS:
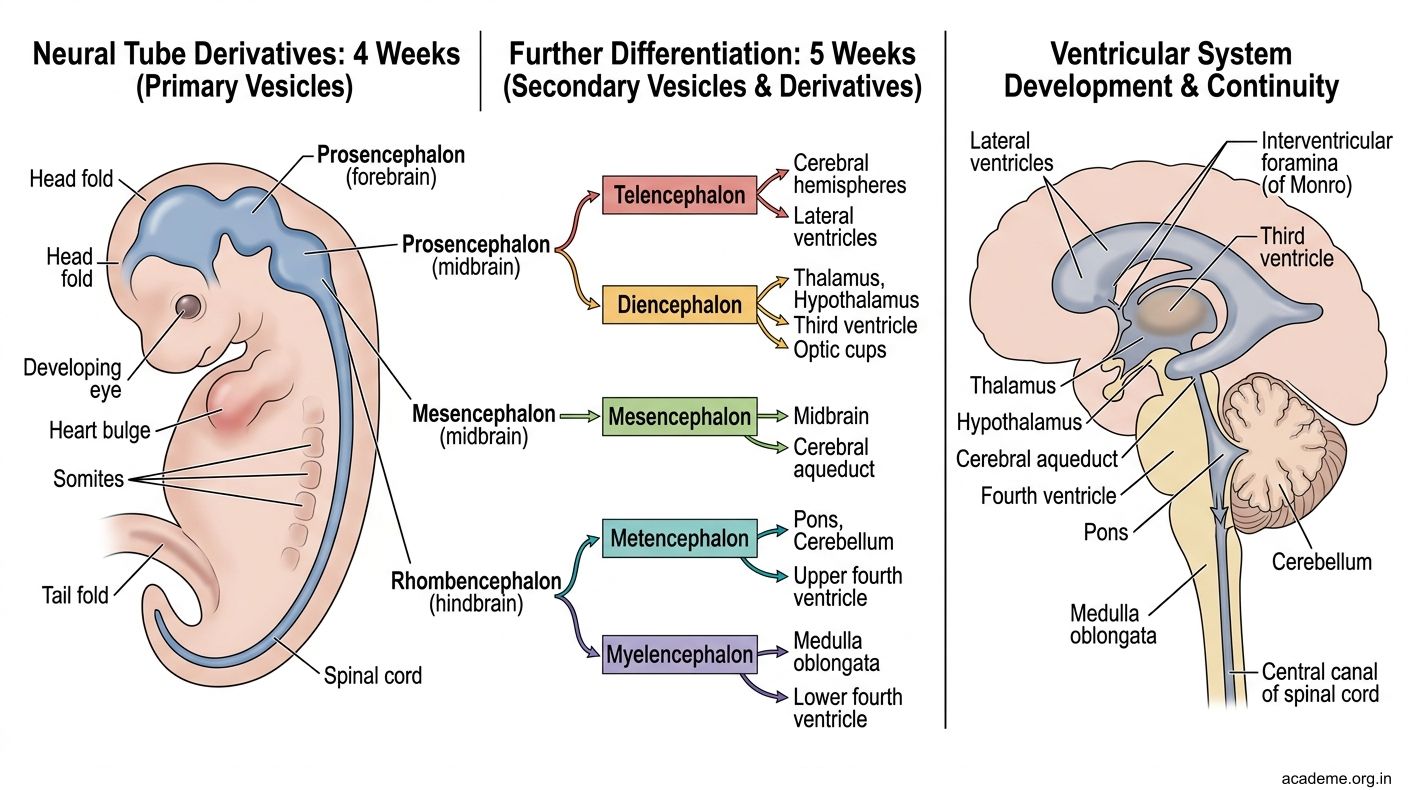
Figure: Neural Tube → CNS:

Figure: Neural Tube Defects (NTDs) — Clinical Significance (AN79.5):
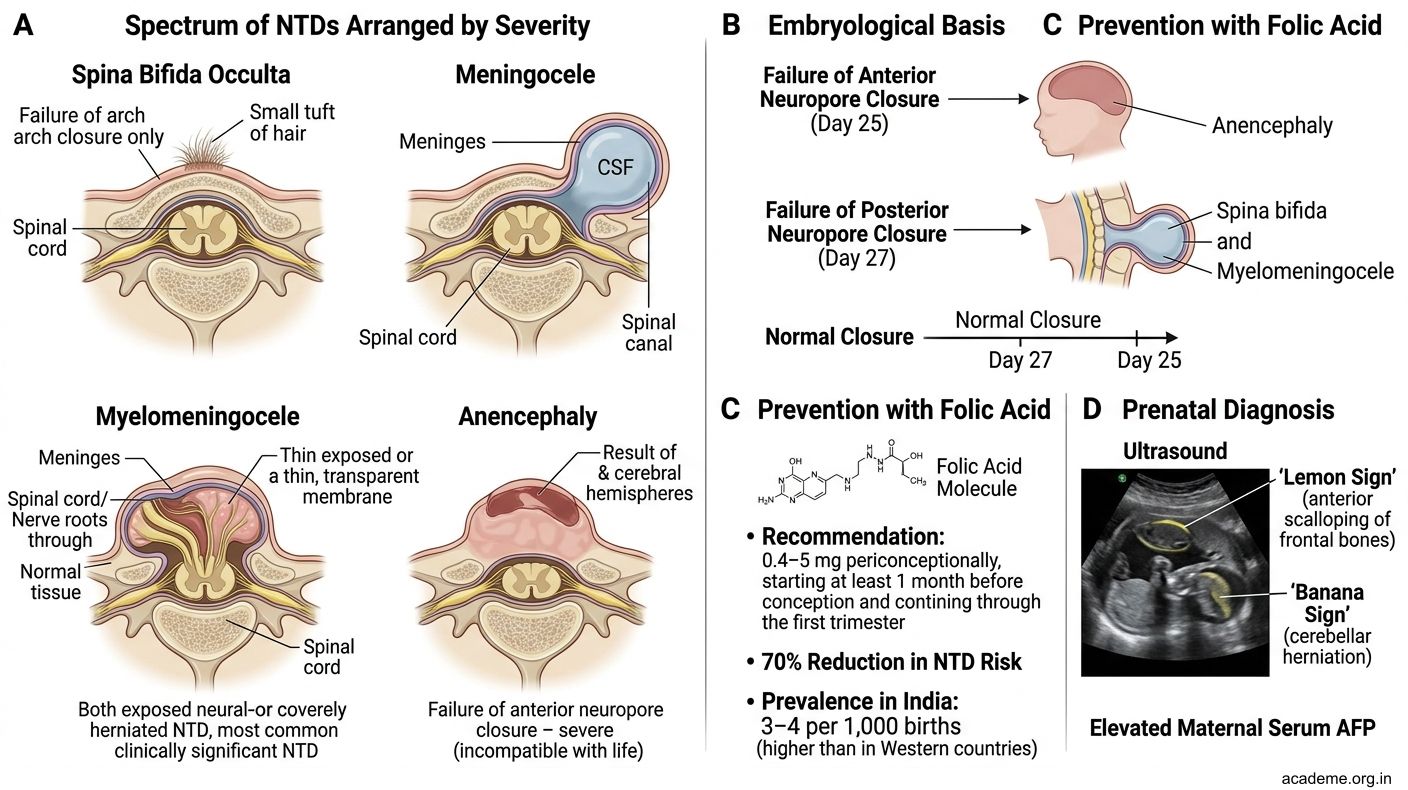
Figure: Neural Tube Defects (NTDs) — Clinical Significance (AN79.5):
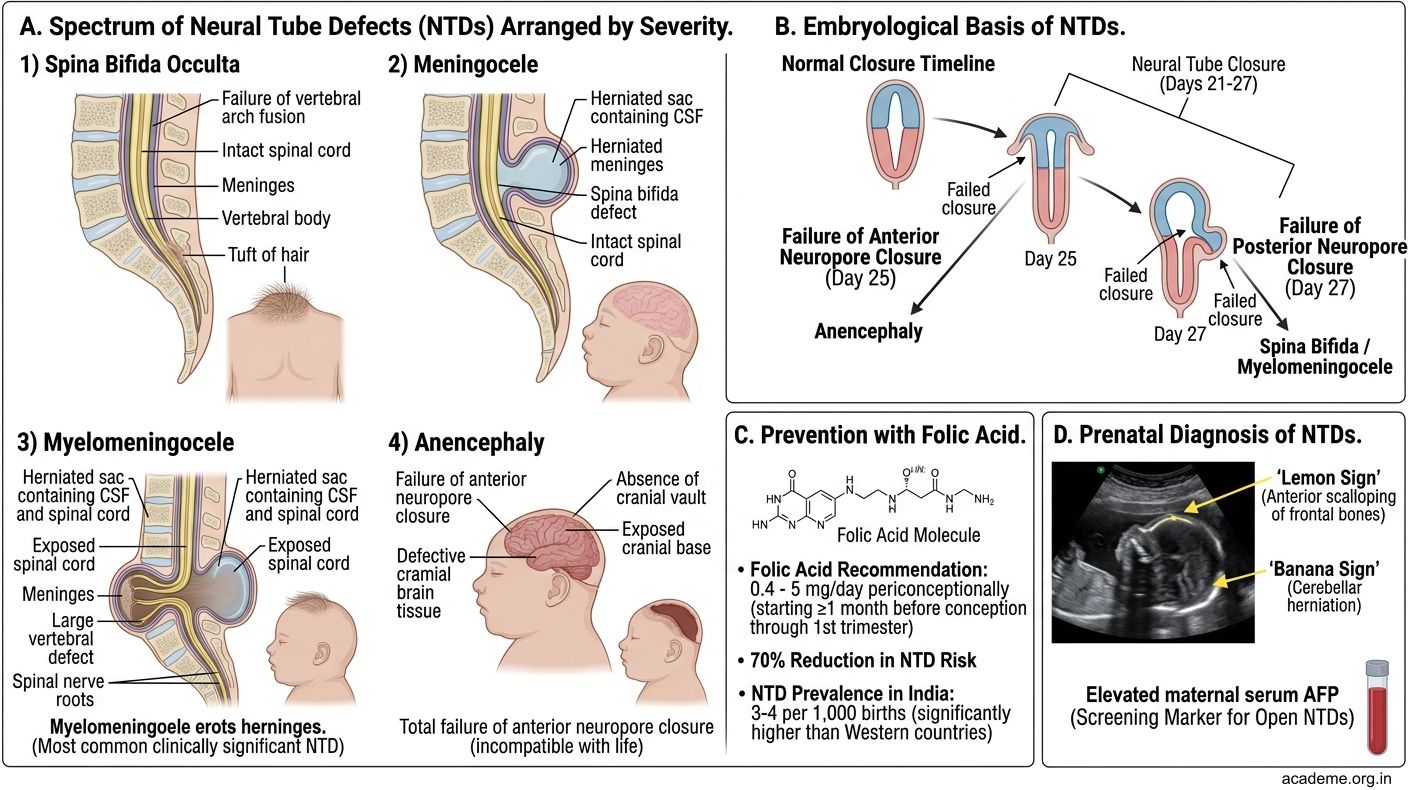
Figure: Neural Tube Defects (NTDs) — Clinical Significance (AN79.5):
Part 4: Somite Development and Intra-Embryonic Coelom (AN79.4)
Somite Formation

Figure: Key Takeaways — 3rd to 8th Week of Development (AN79.1–79.5)

Figure: Congenital Anomalies from 3rd–8th Week — High-Yield Indian Clinical Correlations

Figure: Part 4: Somite Development and Intra-Embryonic Coelom (AN79.4)
Paraxial mesoderm (mesoderm adjacent to the notochord and neural tube) segments into paired blocks called somites starting from the 20th day.
Somite timeline:
• 1st pair: appears at the cranial end on Day 20
• New pairs added caudally at the rate of ~3 per day
• Total: 42–44 pairs (8 occipital, 12 thoracic, 5 lumbar, 5 sacral, 8–10 coccygeal) — number used to estimate embryonic age
• Total somites appears between Days 20–30
Somite Derivatives (3 components):
| Component | Location | Derivatives |
|---|---|---|
| Sclerotome (ventromedial) | Surrounds notochord and neural tube | Vertebral body, vertebral arch, intervertebral disc (annulus fibrosus), ribs |
| Myotome (dorsomedial) | Lateral to sclerotome | Skeletal muscles of trunk (back muscles, intercostals, abdominal wall); each myotome → one spinal segment |
| Dermatome (dorsolateral) | Migrates to surface | Dermis of back skin; each dermatome → sensory supply from one spinal segment |
Note: The word "dermatome" in clinical anatomy (a strip of skin supplied by one spinal nerve) derives directly from the embryological dermatome concept.
Resegmentation:
Each vertebra is formed by fusion of the caudal half of one sclerotome + cranial half of the next sclerotome → this places the myotome (muscle) and its spinal nerve OPPOSITE a vertebral body (not beside it) — allowing free movement of muscles across joints.
Intra-Embryonic Coelom (Body Cavity)
Formation:
• The lateral plate mesoderm (lateral to the somites) splits into two layers:
- Somatic (parietal) mesoderm — adjacent to ectoderm
- Splanchnic (visceral) mesoderm — adjacent to endoderm/yolk sac
• The space between them = intraembryonic coelom (appears around Day 21–28)
Partitioning of the coelom:
| Final Cavity | Location | Lining |
|---|---|---|
| Pericardial cavity | Cranial to septum transversum | Pericardium |
| Pleural cavities (×2) | Between pericardial and peritoneal | Pleura |
| Peritoneal cavity | Caudal | Peritoneum |
Partitioning occurs through: (1) Septum transversum (develops into the central tendon of the diaphragm), (2) Pleuropericardial folds, (3) Pleuroperitoneal folds (close the pleuroperitoneal canals).
Clinical: Congenital Diaphragmatic Hernia (CDH):
• The pleuroperitoneal canal fails to close completely (usually on the LEFT side at the foramen of Bochdalek → abdominal contents (intestines, stomach, spleen) herniate into the left pleural cavity → compress the developing lung → pulmonary hypoplasia
• Presents at birth with respiratory distress; scaphoid abdomen; heart shifted to right on X-ray
• Mortality ~50% due to pulmonary hypoplasia; treated by surgical reduction of hernia + lung support
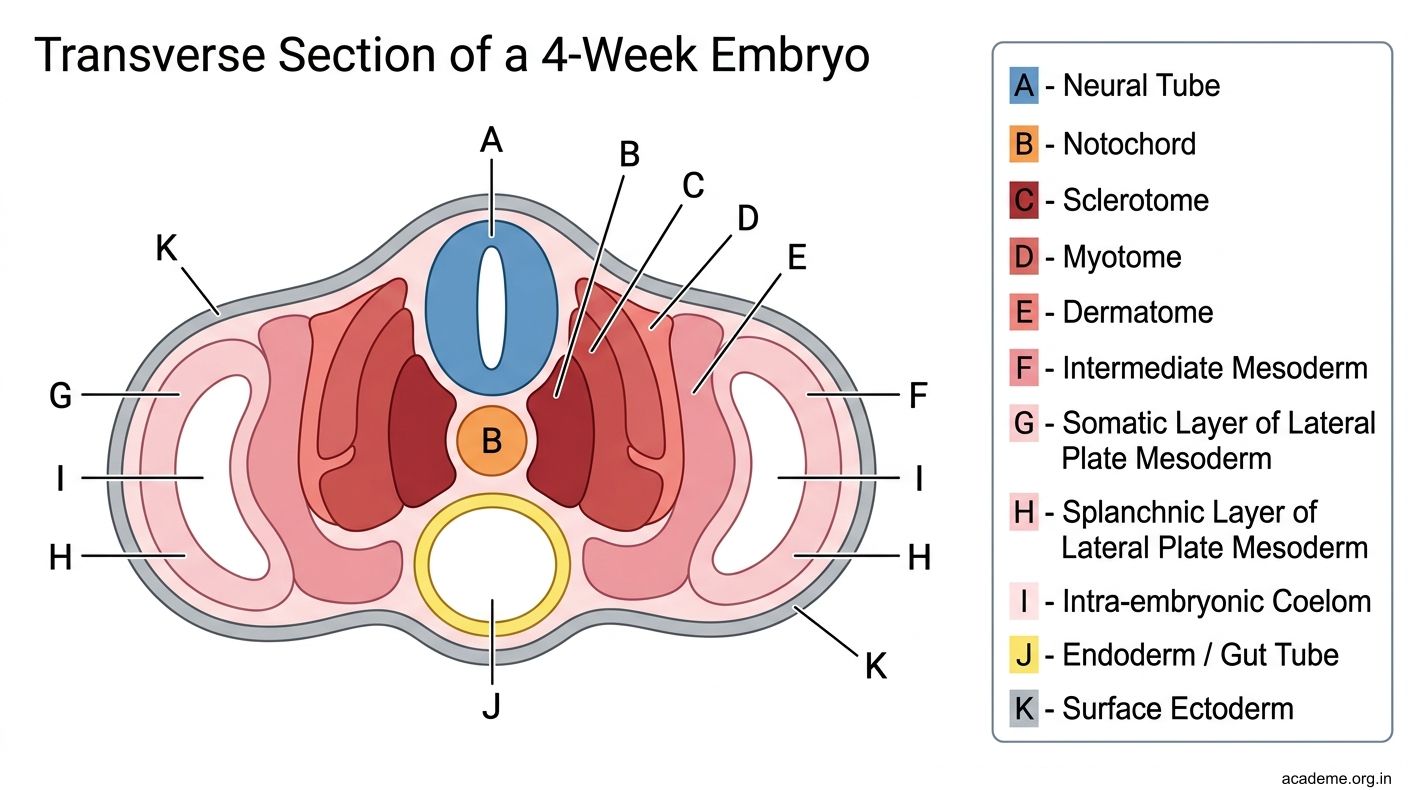
Figure: Part 4: Somite Development and Intra-Embryonic Coelom (AN79.4)

Figure: Somite Derivatives (3 components):
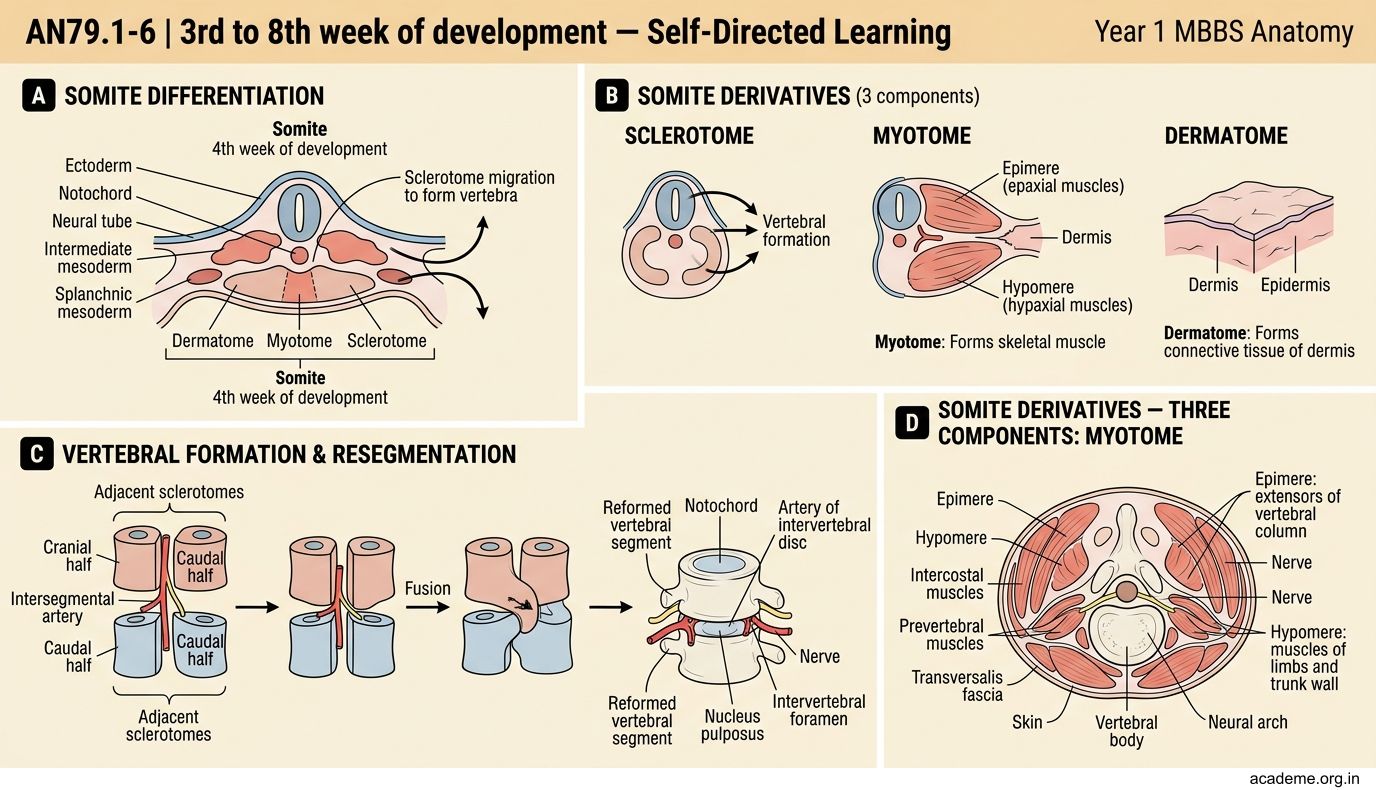
Figure: Somite Derivatives (3 components):
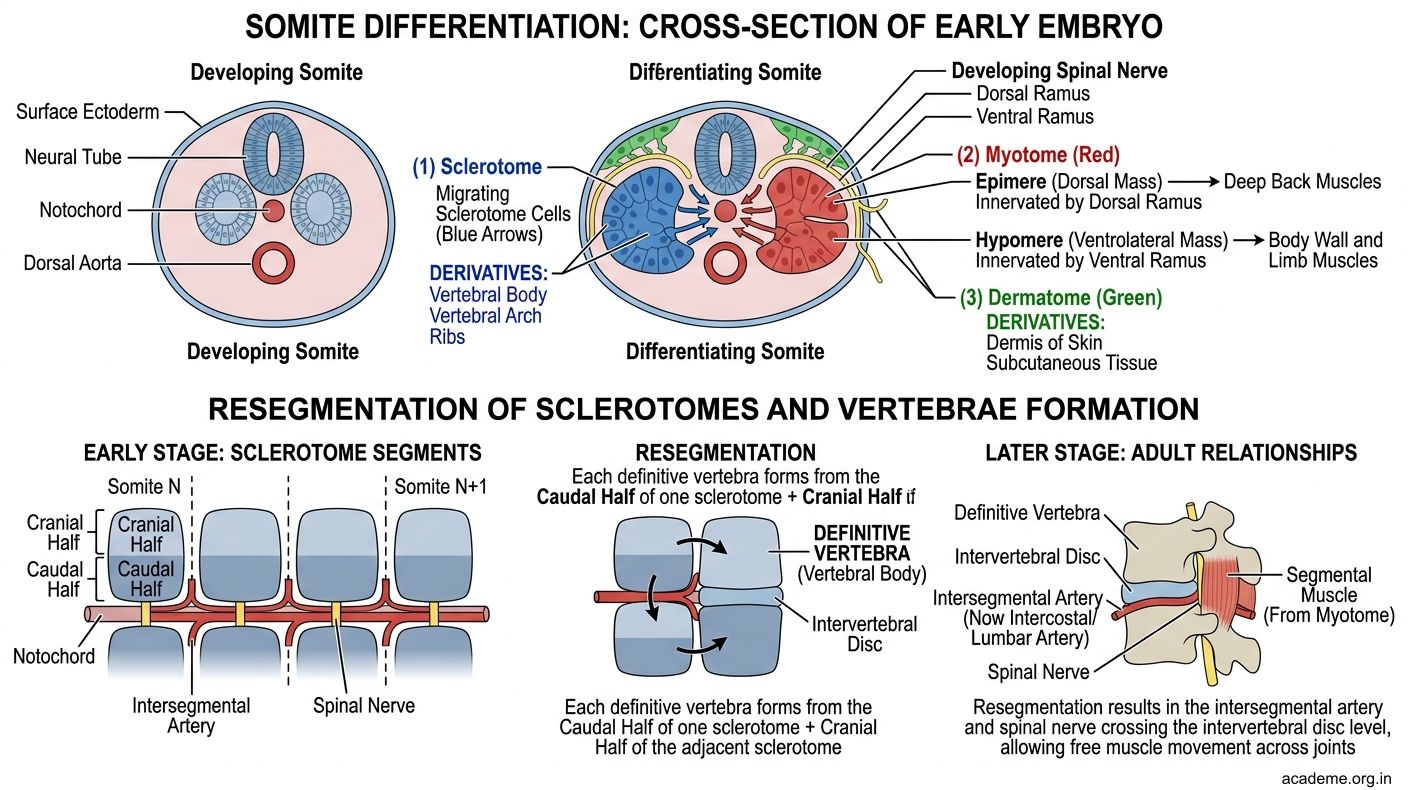
Figure: Somite Derivatives (3 components):

Figure: Intra-Embryonic Coelom (Body Cavity)
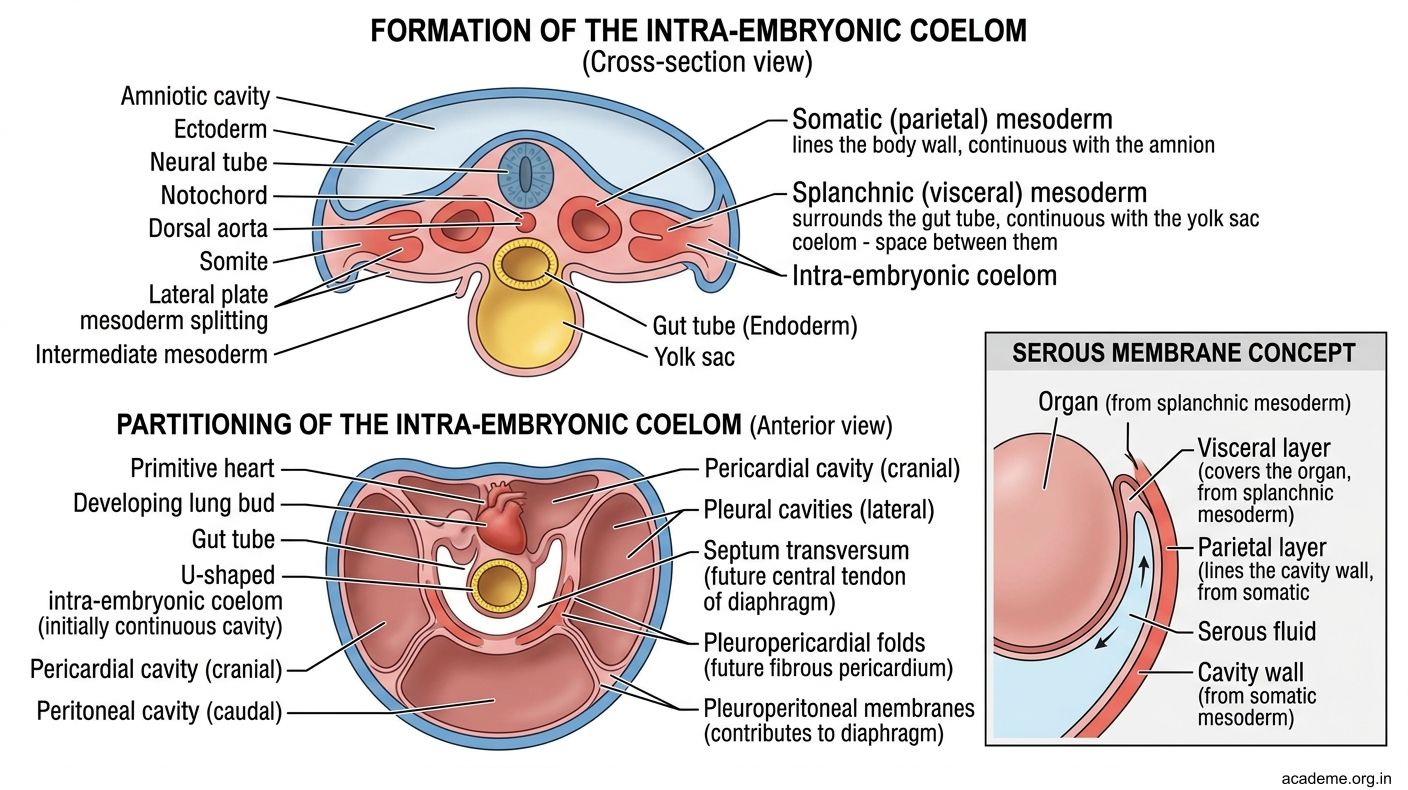
Figure: Intra-Embryonic Coelom (Body Cavity)
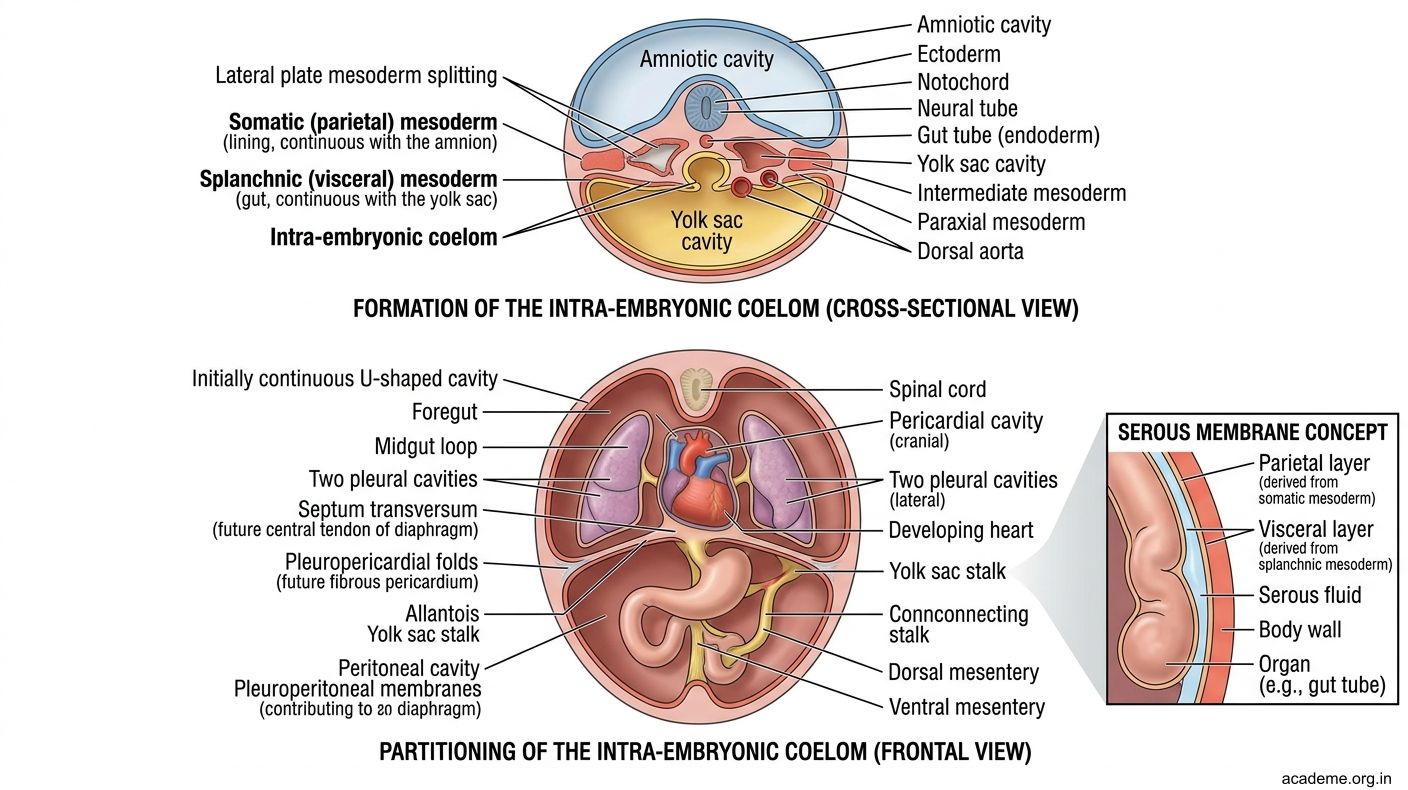
Figure: Intra-Embryonic Coelom (Body Cavity)

Figure: Partitioning of the coelom:
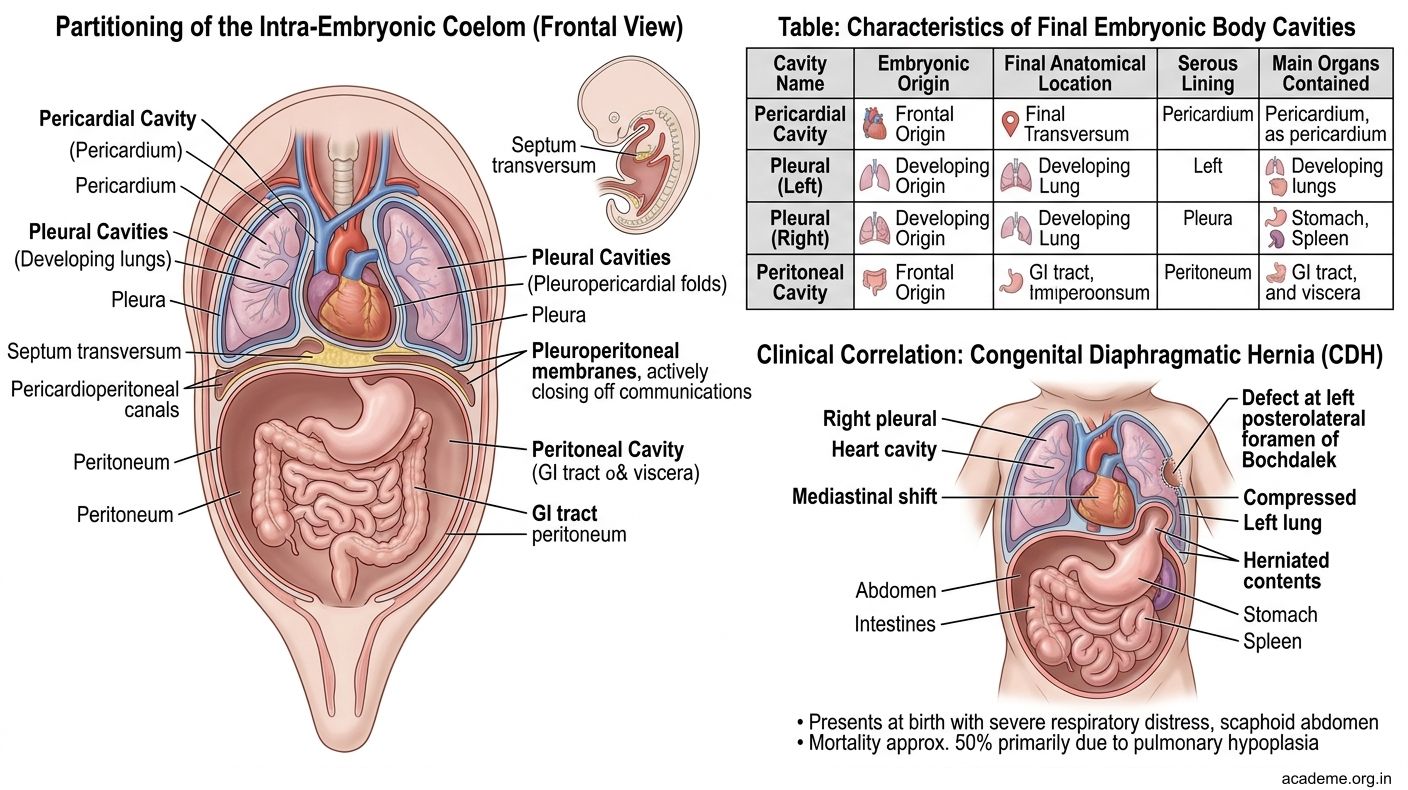
Figure: Partitioning of the coelom:
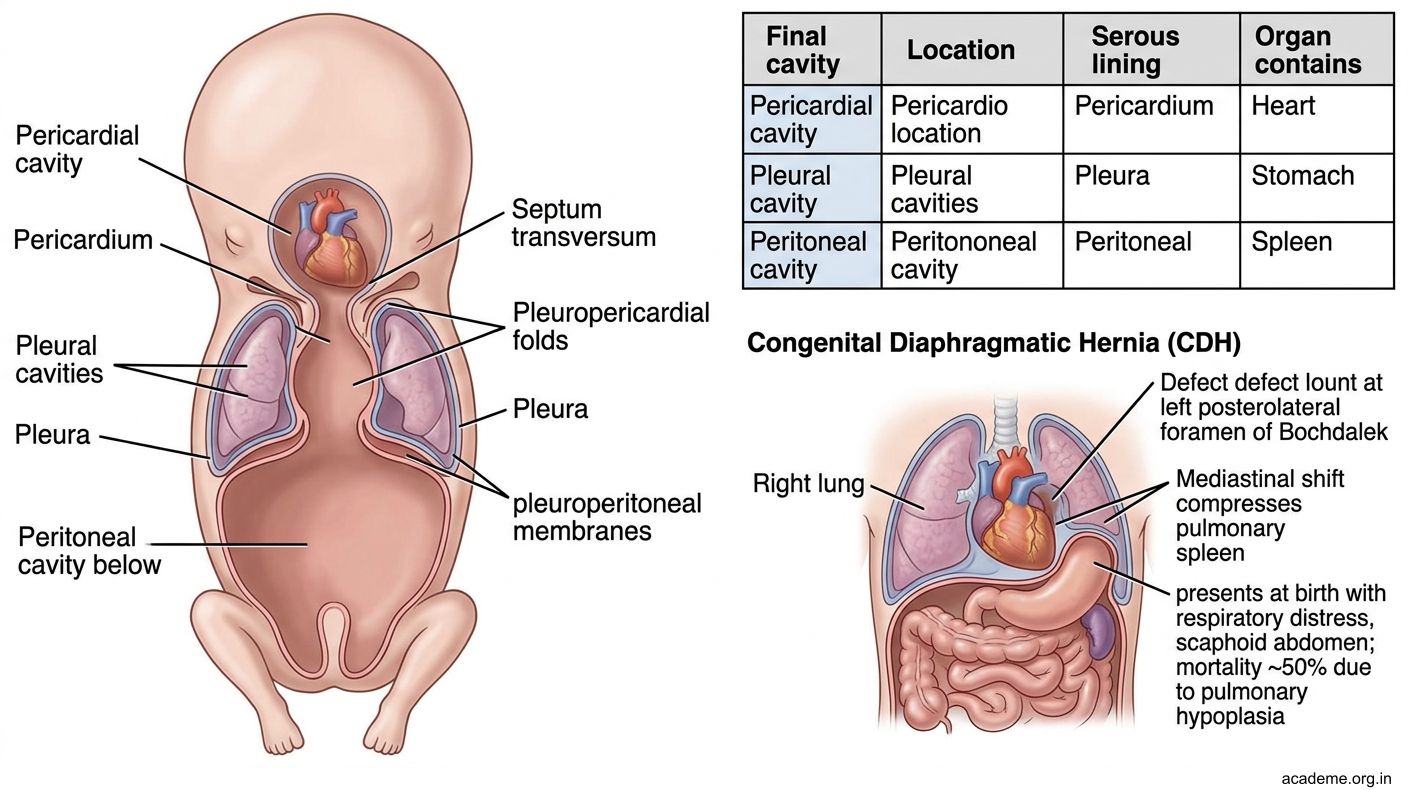
Figure: Partitioning of the coelom:
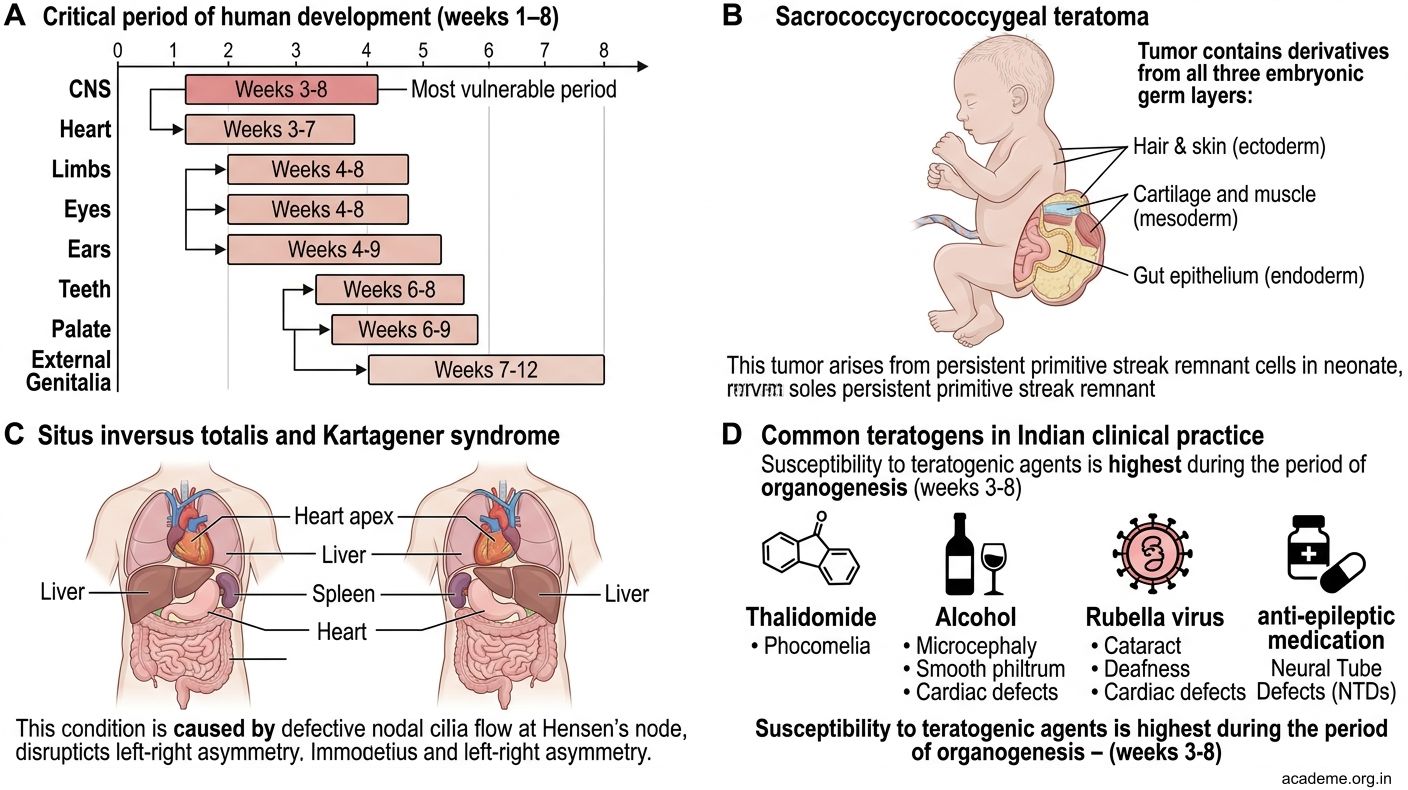
Figure: Congenital Anomalies from 3rd–8th Week — High-Yield Indian Clinical Correlations

Figure: Common teratogens encountered in Indian practice:
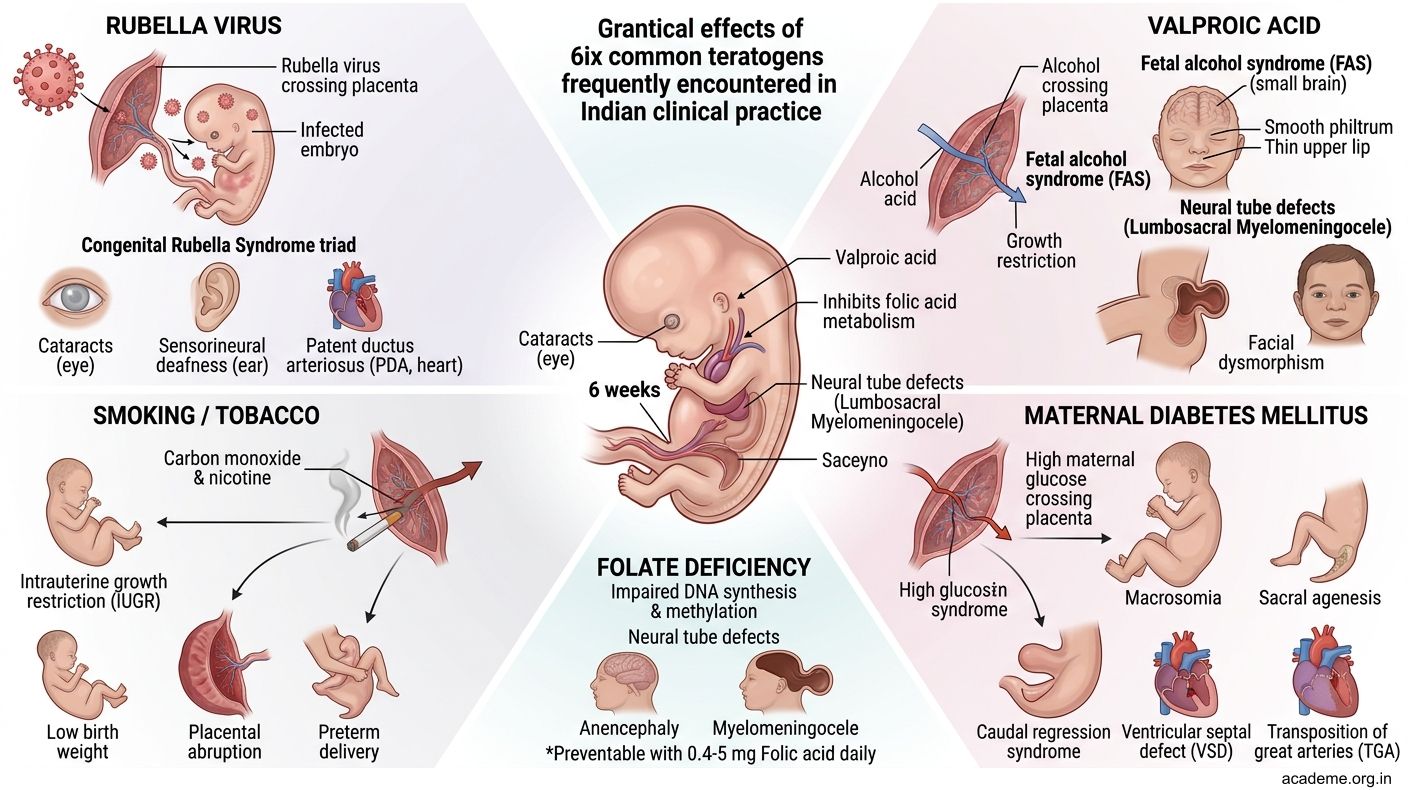
Figure: Common teratogens encountered in Indian practice:
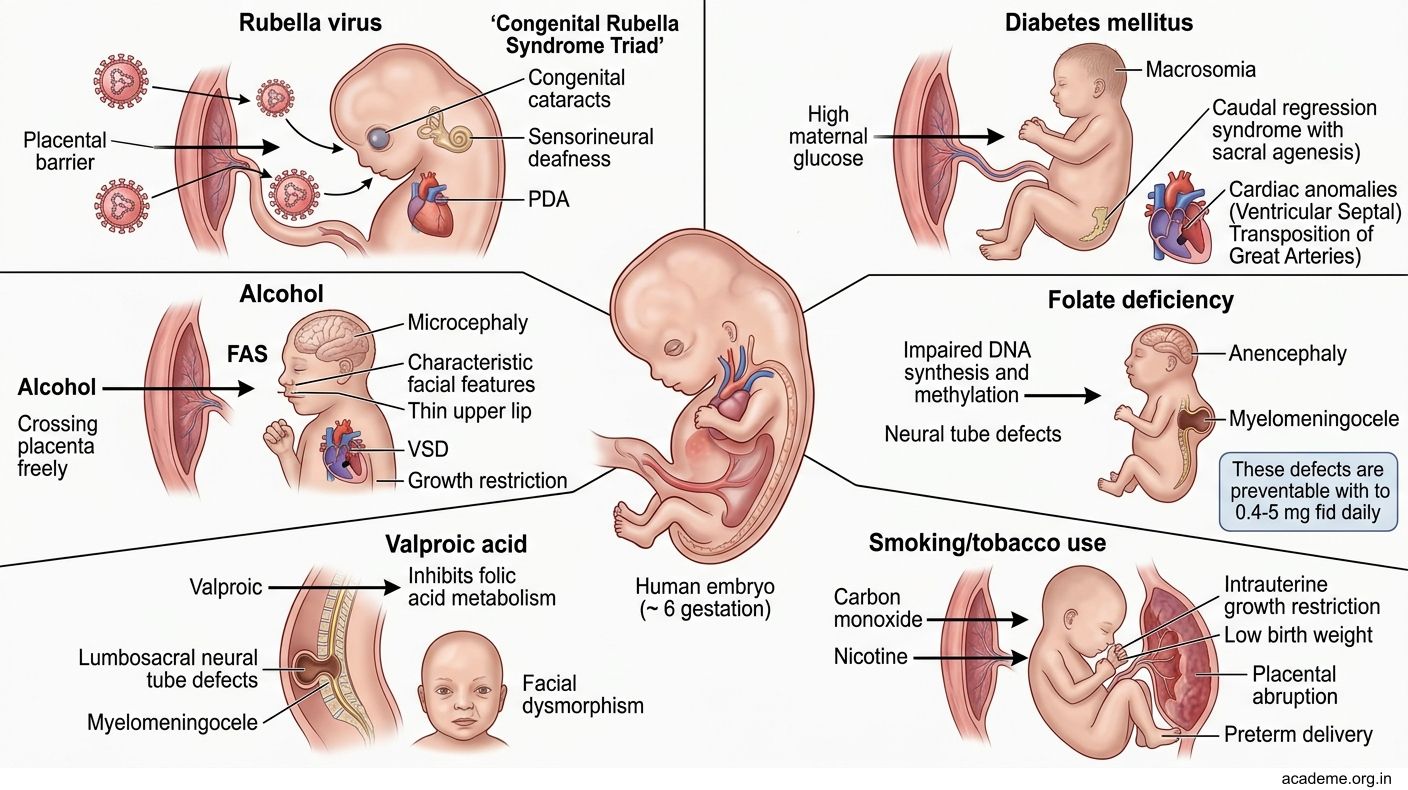
Figure: Common teratogens encountered in Indian practice:
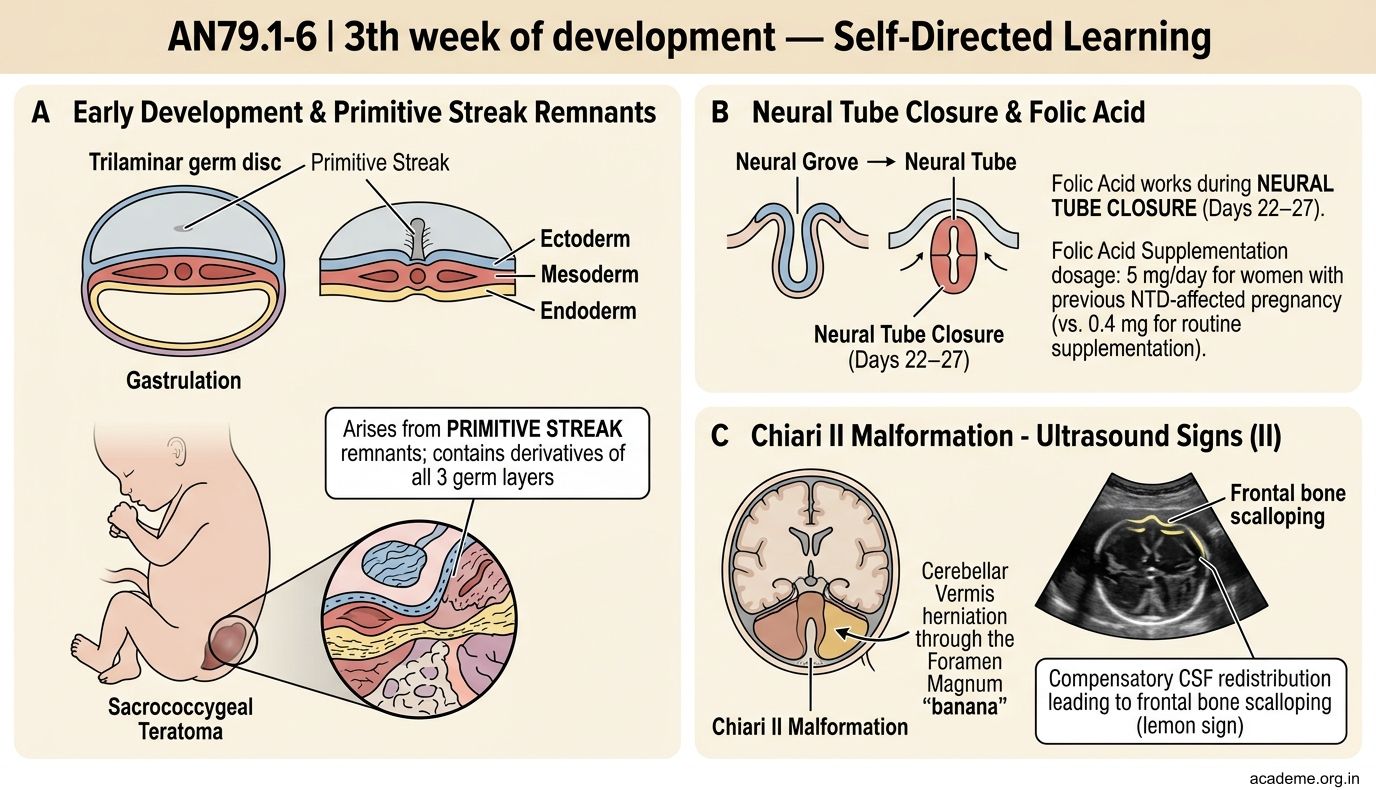
Figure: Key Takeaways — 3rd to 8th Week of Development (AN79.1–79.5)
SELF-CHECK — : 3rd–8th Week Development
Gastrulation converts the bilaminar disc into the trilaminar disc. The intraembryonic mesoderm is formed by cells that originate from which layer and migrate through which structure?
A. Hypoblast cells migrating through the primitive node
B. Epiblast cells migrating through the primitive streak
C. Hypoblast cells migrating through the primitive streak
D. Epiblast cells remaining in place on the surface
Reveal Answer
Answer: B. Epiblast cells migrating through the primitive streak
The nucleus pulposus of an intervertebral disc is a remnant of which embryological structure?
A. Primitive streak
B. Sclerotome
C. Notochord
D. Neural crest
Reveal Answer
Answer: C. Notochord
Neural tube closure begins in the mid-cervical region. The LAST structure to close is:
A. Anterior neuropore (Day 25)
B. Mid-cervical region (Day 22)
C. Brain vesicles
D. Posterior neuropore (Day 27)
Reveal Answer
Answer: D. Posterior neuropore (Day 27)
CLINICAL PEARL
Congenital Anomalies from 3rd–8th Week — High-Yield Indian Clinical Correlations
Teratogen-Sensitive Period:
The 3rd–8th weeks = the critical period of organogenesis. Teratogens cause major structural defects during this window. Exposure BEFORE the 3rd week → all-or-nothing effect (death or survival without defect). Exposure AFTER the 8th week → functional defects (growth, CNS maturation) but not major structural malformations.
Common teratogens encountered in Indian practice:
| Teratogen | Defects Caused |
|---|---|
| Thalidomide (anti-nausea) | Phocomelia (seal-limb deformity); now banned in pregnancy |
| Sodium valproate (epilepsy) | Neural tube defects; commonly used antiepileptic in India |
| Alcohol (FAS) | Fetal Alcohol Syndrome — microcephaly, facial dysmorphism, growth restriction; increasing problem in India |
| Rubella virus (1st trimester) | Cataracts, cardiac defects (PDA, pulmonary stenosis), sensorineural deafness — Gregg's triad |
| CMV (cytomegalovirus) | Sensorineural deafness, periventricular calcifications, mental retardation; most common congenital infection causing NTDs |
| Retinoic acid (acne treatment) | Neural crest cell disruption → craniofacial defects, cardiac defects, CNS malformations |
| Diabetes mellitus (poorly controlled) | Caudal regression syndrome (sacral agenesis), NTDs, cardiac defects |
Folic Acid and NTDs:
Folic acid is essential for the one-carbon transfer reactions needed for DNA synthesis and cell division during neural tube closure. Deficiency → impaired closure at the neuropores → NTDs.
REFLECT
Return to the case of the 26-year-old woman with the myelomeningocele fetus:
- The neural tube defect is at the lumbosacral level. This means the posterior neuropore (which closes on Day 27) failed to close. What would a defect at the ANTERIOR neuropore produce instead?
- The "lemon sign" and "banana sign" on ultrasound indicate Chiari II malformation. Explain the anatomy of Chiari II in terms of neural tube embryology.
- The obstetrician advises folic acid for the next pregnancy. At what specific stage of development does folic acid act to prevent NTDs, and what is the recommended dose for a woman with a previous NTD-affected pregnancy?
- At birth, a neonate has a large sacrococcygeal mass. The paediatric surgeon explains it arose from incomplete regression of a structure. Which structure, and which germ layers are represented in this tumour?
Discussion: (1) Anterior neuropore failure → ANENCEPHALY (absent cranial vault and brain). (2) Chiari II: myelomeningocele causes downward traction on the brainstem and cerebellum → cerebellar tonsils and vermis herniate through the foramen magnum → "banana" sign on US; compensatory CSF redistribution → frontal bone scalloping = "lemon sign". (3) Folic acid works during NEURAL TUBE CLOSURE (Days 22–27); 5 mg/day for women with previous NTD-affected pregnancy (vs. 0.4 mg for routine supplementation). (4) Sacrococcygeal teratoma arises from PRIMITIVE STREAK remnants; contains derivatives of all 3 germ layers.
KEY TAKEAWAYS
Key Takeaways — 3rd to 8th Week of Development (AN79.1–79.5)
Primitive Streak (AN79.1):
• Appears Day 14–15, caudal midline; establishes body axes; gastrulation = bilaminar → trilaminar disc
• Fate: regresses and disappears by end of 4th week
• Remnant → sacrococcygeal teratoma (most common neonatal solid tumour)
Notochord (AN79.2):
• From primitive node; extends cranially in midline; induces neural plate formation
• Fate: incorporated into vertebral bodies (disappears) + persists at disc levels = nucleus pulposus
• Disc prolapse = nucleus pulposus herniation through torn annulus fibrosus
Neurulation (AN79.3):
• Neural plate → neural folds → neural tube; closure starts mid-cervical, spreads both ways
• Anterior neuropore closes Day 25; Posterior neuropore closes Day 27
• NTDs: anencephaly (anterior failure), myelomeningocele (posterior failure)
• Prevention: periconceptional folic acid
Somites and Coelom (AN79.4):
• Somites from paraxial mesoderm; appear Day 20, ~3/day; count = embryonic age
• Sclerotome → vertebrae; myotome → trunk muscles; dermatome → back skin
• Intraembryonic coelom → pericardial + pleural + peritoneal cavities
• CDH = pleuroperitoneal canal fails to close → herniation into pleural cavity
Congenital Anomalies (AN79.5):
• Critical period = 3rd–8th weeks (organogenesis)
• Teratogens: valproate (NTDs), thalidomide (phocomelia), rubella (Gregg's triad), alcohol (FAS)