Page 1 of 8
BI5.1-9 | Chemistry & Metabolism of Proteins and Immunology — SDL Guide
Learning Objectives
- Describe the structure and classification of amino acids based on nutritional and metabolic significance (BI5.1)
- Classify proteins by structure and function, and explain the four levels of structural organisation (BI5.2)
- Describe the digestion and absorption of dietary proteins (BI5.3)
- Describe plasma proteins, their functions, and interpret normal vs abnormal electrophoretic patterns (BI5.4)
- Describe the structure and functions of immunoglobulins and the basics of humoral and cellular immunity (BI5.5)
- Describe ammonia formation, transport, detoxification via the urea cycle, and the clinical significance of ammonia toxicity (BI5.6)
- Describe specialised products from key amino acids and inborn errors of metabolism, including newborn screening (BI5.7)
- Describe the structure and metabolism of haem, with emphasis on jaundice and porphyrias (BI5.8)
- Describe the types, derivatives, and variants of haemoglobin and their clinical relevance (BI5.9)
INSTRUCTIONS
The collagen in your bones, the haemoglobin in your blood, and the antibodies fighting infection RIGHT NOW are all proteins. They make up 50% of the dry weight of your body. This module takes you from the simplest amino acid to the most complex protein machines, and then shows you what happens when the machinery breaks down.
Parallel connections: In Anatomy, you're learning about bones and cartilage — collagen is the protein that makes both of them strong. Type I collagen forms 90% of bone's organic matrix, and Type II collagen is the structural backbone of cartilage. In Physiology, the cell membrane proteins you're studying are the channels and receptors that control everything — every ion channel is a protein, every receptor is a protein, every transporter is a protein.
References
- Harper's Illustrated Biochemistry, 32nd ed., Chapters 3-4 (Amino Acids & Proteins), Chapters 28-29 (Amino Acid Metabolism) (textbook)
- Lehninger Principles of Biochemistry, 8th ed., Chapter 3: Amino Acids, Peptides, and Proteins (textbook)
- Satyanarayana's Biochemistry, 6th ed., Chapters 4-6 (Proteins, Amino Acid Metabolism) (textbook)
- Vasudevan's Textbook of Biochemistry, 9th ed., Section 3: Proteins and Amino Acids (textbook)
Version 2.0 | NMC CBUC 2024, Adapted from Harper's Illustrated Biochemistry 32e
CLINICAL SCENARIO
Your body contains roughly 100,000 different proteins — enzymes, antibodies, receptors, transporters, structural scaffolds — and every single one of them is built from just 20 amino acids. That's like building every word in the English language from 26 letters. The difference between a digestive enzyme and an antibody isn't the building blocks — it's the sequence in which those blocks are assembled. One wrong amino acid in haemoglobin's 574-amino-acid chain causes sickle cell disease. One missing enzyme in the amino acid degradation pathway causes a baby to accumulate phenylalanine until the brain is irreversibly damaged. Proteins are not abstract chemistry — they are the molecular workforce that keeps you alive, and their failures are the diseases you will treat.
WHY THIS MATTERS
As a doctor, proteins will follow you everywhere. In the laboratory, you'll order serum protein electrophoresis to detect multiple myeloma. In the ward, you'll manage a jaundiced newborn whose bilirubin (a haem breakdown product) is dangerously high. In the clinic, you'll screen newborns for phenylketonuria (PKU) — a disorder of amino acid metabolism that causes intellectual disability if missed. In immunology, you'll understand how antibodies work, why some patients lack them (agammaglobulinaemia), and why monoclonal antibodies are revolutionising cancer treatment. And in haematology, you'll differentiate between HbS (sickle cell), HbF (foetal), and HbA1c (diabetes monitoring) — all variants of one protein.
RECALL
From your school-level chemistry, you know that atoms form bonds (covalent, ionic, hydrogen), that pH measures acidity, and that organic molecules contain carbon. You've also heard the word 'protein' in the context of diet. We'll build on that foundation: amino acids are organic molecules with both an amino group and a carboxyl group, and they link together through peptide bonds to form proteins. No new chemistry is needed — just the willingness to see patterns.
Amino Acid Structure — The Universal Building Block (BI5.1)
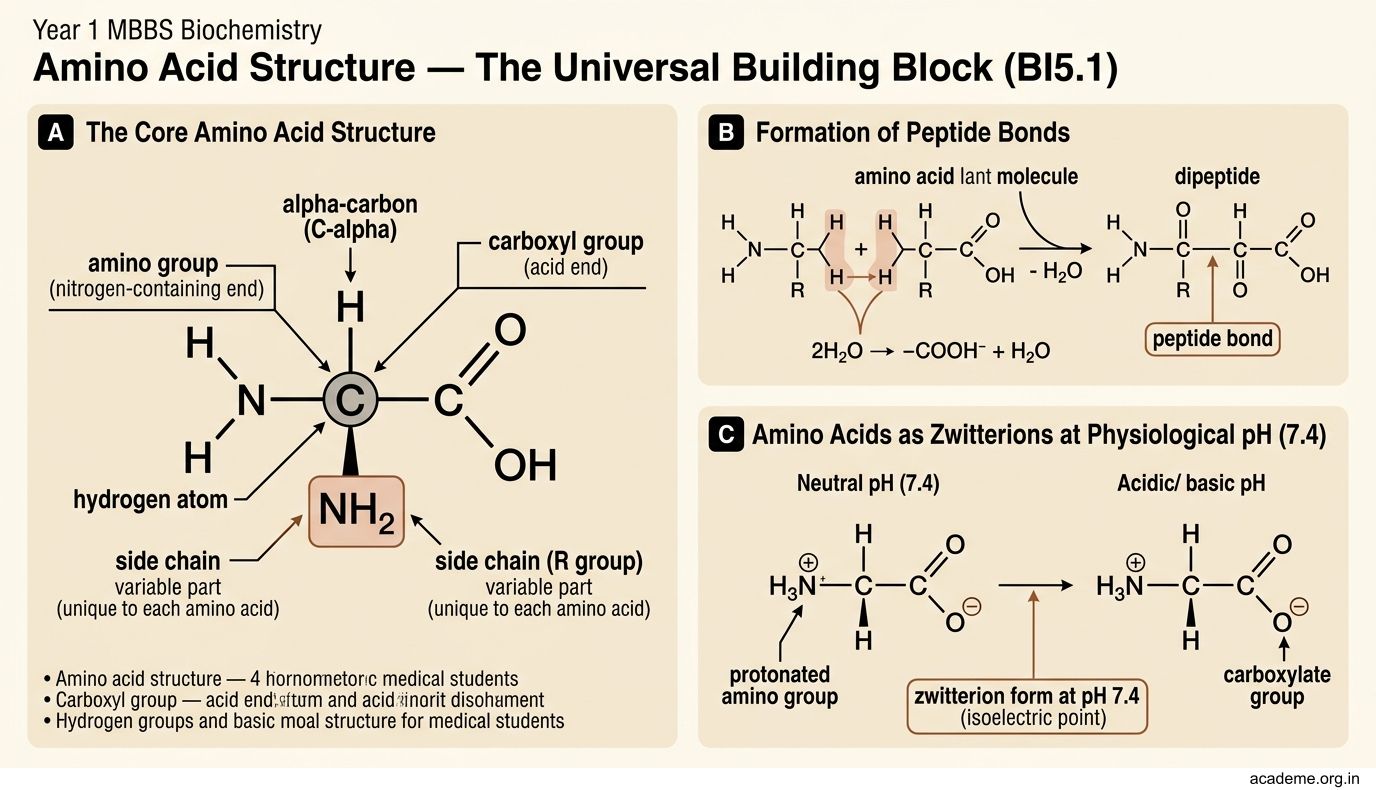
Every amino acid has the same core structure — a central alpha-carbon (C-alpha) bonded to four groups:

Figure: Classification by R-group chemistry:

Figure: Classification by nutritional significance:

Figure: Amino Acid Structure — The Universal Building Block (BI5.1)
- An amino group (-NH2) — the nitrogen-containing end
- A carboxyl group (-COOH) — the acid end
- A hydrogen atom (-H)
- A side chain (R group) — this is the variable part that makes each amino acid unique
At physiological pH (7.4), amino acids exist as zwitterions — the amino group is protonated (-NH3+) and the carboxyl group is deprotonated (-COO-). This means amino acids carry both a positive and negative charge simultaneously.
All amino acids except glycine are optically active — they have a chiral centre at the alpha-carbon. Human proteins use only L-amino acids (the D-form is found in bacterial cell walls — this is why D-amino acids are targets for antibiotics).
Classification by nutritional significance:
- Essential amino acids (9) — your body cannot synthesise them; they must come from diet: PVT TIM HALL (Phe, Val, Trp, Thr, Ile, Met, His, Arg, Leu, Lys). Arg is semi-essential — needed in children for growth.
- Non-essential amino acids (11) — your body can make them from metabolic intermediates.
Classification by R-group chemistry:
- Non-polar/hydrophobic — Gly, Ala, Val, Leu, Ile, Pro, Phe, Trp, Met (these tend to cluster inside proteins, away from water)
- Polar uncharged — Ser, Thr, Cys, Tyr, Asn, Gln (can form hydrogen bonds)
- Positively charged (basic) — Lys, Arg, His (attracted to negative charges)
- Negatively charged (acidic) — Asp, Glu (attracted to positive charges)
Why does classification matter clinically? Because phenylketonuria (PKU) is the inability to convert phenylalanine (essential) to tyrosine (non-essential). If Phe accumulates, it damages the brain. If you understand the classification, you understand why a Phe-restricted diet works — you're removing the amino acid the body can't process while supplementing the one it can't make from it.
Protein Structure — Four Levels of Organisation (BI5.2)
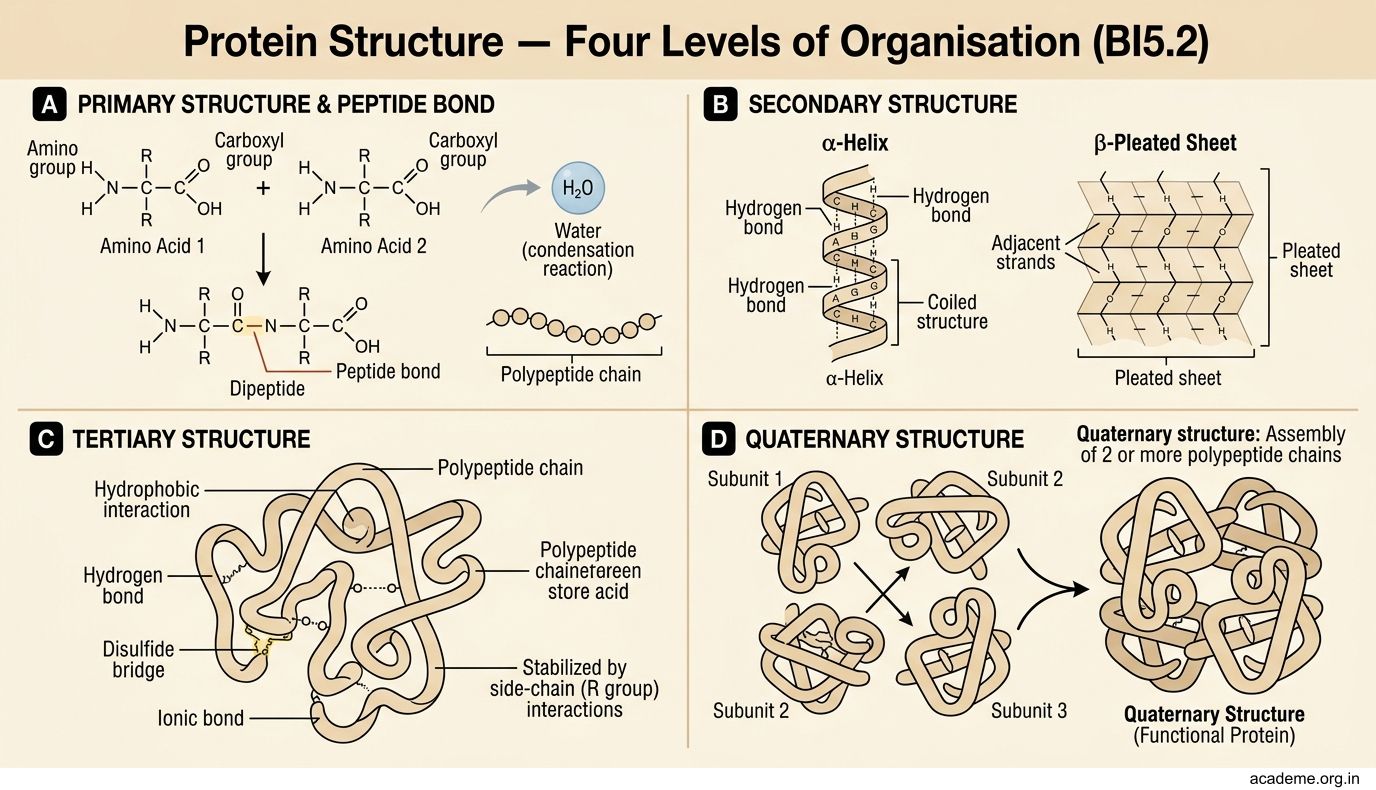
Amino acids join together through peptide bonds — a covalent bond formed between the carboxyl group of one amino acid and the amino group of the next, releasing water (condensation reaction). Two amino acids make a dipeptide, three make a tripeptide, and chains longer than 10 are polypeptides. A protein is one or more polypeptide chains folded into a specific 3D shape.

Figure: Protein Structure — Four Levels of Organisation (BI5.2)
Proteins have four levels of structure, and each level matters clinically:
1. Primary structure — the linear sequence of amino acids, read from the N-terminus (amino end) to the C-terminus (carboxyl end). This sequence is encoded by DNA. A single amino acid change here can cause disease — in sickle cell disease, glutamic acid at position 6 of the beta-globin chain is replaced by valine (Glu→Val). That's one amino acid out of 146, and it transforms the behaviour of the entire molecule.
2. Secondary structure — local folding patterns stabilised by hydrogen bonds between backbone atoms (not R-groups):
- Alpha-helix (α-helix) — the polypeptide coils into a right-handed spiral. Each turn has 3.6 amino acids. Think of it as a spiral staircase. Keratin (hair, nails) is largely alpha-helical.
- Beta-sheet (β-sheet) — the chain folds back and forth in a zigzag, forming flat sheets held together by hydrogen bonds between parallel or antiparallel strands. Silk fibroin is mostly beta-sheet.
3. Tertiary structure — the overall 3D shape of a single polypeptide, determined by interactions between R-groups:
- Hydrophobic interactions (non-polar R-groups cluster inside, away from water)
- Hydrogen bonds (between polar R-groups)
- Ionic bonds (between oppositely charged R-groups)
- Disulfide bonds (covalent S-S links between two cysteine residues — these are the strongest)
This is the level where the protein becomes functional. Myoglobin (an oxygen-carrying protein in muscle) is a single polypeptide with a specific tertiary structure.
4. Quaternary structure — the arrangement of multiple polypeptide subunits into a functional complex. Haemoglobin is the classic example: it has 4 subunits (2 alpha + 2 beta chains). The quaternary structure allows cooperativity — when one subunit binds oxygen, the others change shape and bind oxygen more easily (this is why haemoglobin's oxygen dissociation curve is sigmoidal, not hyperbolic like myoglobin's).
Denaturation — when a protein loses its 3D structure (secondary, tertiary, quaternary) but keeps its primary sequence intact. Causes include heat, extreme pH, organic solvents, and heavy metals. A boiled egg is denatured egg white (albumin) — the proteins unfold irreversibly. Clinically, fever can denature enzymes if body temperature exceeds 41°C, which is why hyperthermia is a medical emergency.
Protein Classification and Functions (BI5.2 continued)
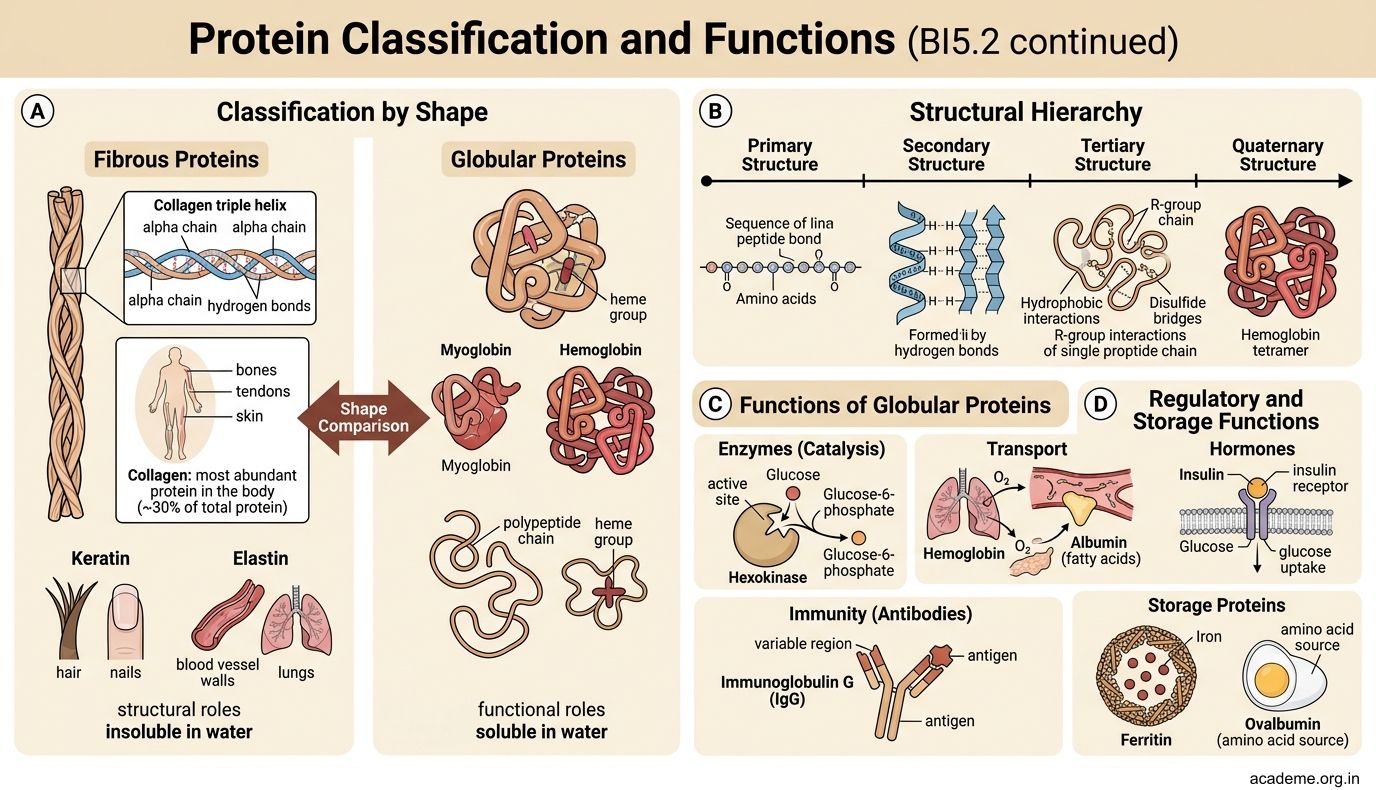
Proteins are classified in several ways:

Figure: Protein Classification and Functions (BI5.2 continued)
By shape:
- Fibrous proteins — long, rope-like, insoluble in water, structural roles. Examples: collagen (bones, tendons, skin — most abundant protein in the body, ~30% of total protein), keratin (hair, nails), elastin (blood vessel walls, lungs).
- Globular proteins — compact, spherical, soluble in water, functional roles. Examples: haemoglobin (oxygen transport), albumin (plasma oncotic pressure), enzymes (catalysis), antibodies (immunity).
By composition:
- Simple proteins — only amino acids. Example: albumin.
- Conjugated proteins — amino acids + a non-protein component (prosthetic group):
- Glycoproteins (+ carbohydrate) — e.g., mucins, antibodies
- Lipoproteins (+ lipid) — e.g., LDL, HDL
- Metalloproteins (+ metal ion) — e.g., ferritin (iron), ceruloplasmin (copper)
- Chromoproteins (+ coloured prosthetic group) — e.g., haemoglobin (haem), cytochromes
- Nucleoproteins (+ nucleic acid) — e.g., histones
- Phosphoproteins (+ phosphate) — e.g., casein (milk)
Collagen — the protein you'll meet in every organ:
Collagen has a unique structure — three polypeptide chains (alpha chains) wound around each other in a triple helix (like a rope). Every third amino acid is glycine (Gly-X-Y repeat, where X is often proline and Y is often hydroxyproline). Vitamin C is essential for the hydroxylation of proline and lysine in collagen — without it, collagen is weak, and you get scurvy (bleeding gums, poor wound healing, loose teeth).
There are at least 28 types of collagen. The clinically important ones:
- Type I — bone, skin, tendon, dentin (90% of body collagen)
- Type II — cartilage, vitreous humour
- Type III — blood vessels, skin, uterus (reticular fibres)
- Type IV — basement membranes (forms a mesh, not fibres)
Spiral forward: In Anatomy, you're learning about bones and cartilage. Type I collagen is why bone is strong in tension (mineral gives compressive strength, collagen gives tensile strength). In Pathology, you'll learn about osteogenesis imperfecta — a genetic defect in Type I collagen that makes bones brittle.
Protein Digestion and Absorption (BI5.3)
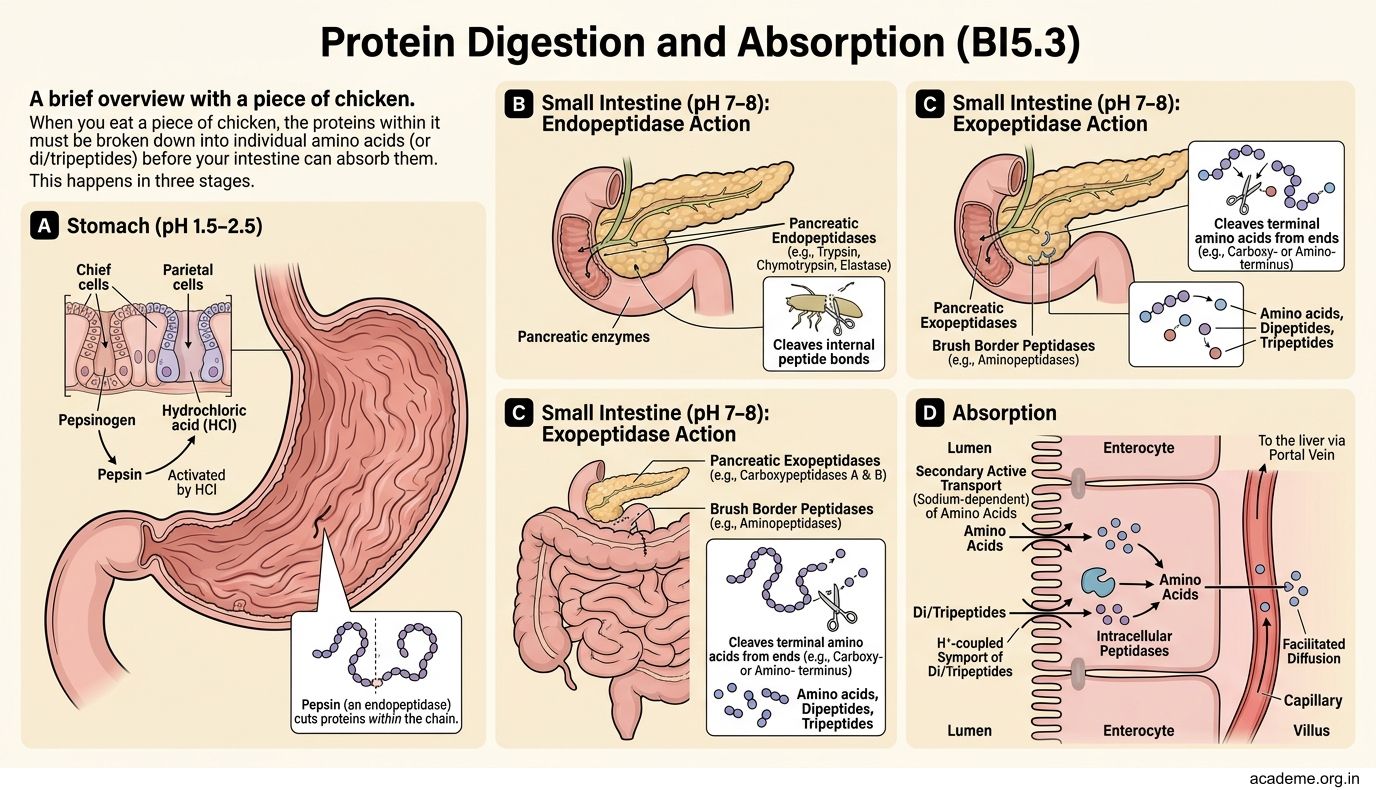
When you eat a piece of chicken, the proteins in it must be broken down into individual amino acids (or di/tripeptides) before your intestine can absorb them. This happens in three stages:

Figure: Protein Digestion and Absorption (BI5.3)
1. Stomach (pH 1.5–2.5):
- Pepsinogen (secreted by chief cells) is activated to pepsin by hydrochloric acid (HCl from parietal cells)
- Pepsin is an endopeptidase — it cuts proteins within the chain, preferring bonds next to aromatic amino acids (Phe, Tyr, Trp)
- The acidic pH also denatures proteins, unfolding them so enzymes can access the peptide bonds
2. Small intestine (pH 7–8):
Pancreatic enzymes take over (all secreted as inactive zymogens to prevent self-digestion):
- Trypsinogen → trypsin (activated by enterokinase from duodenal mucosa) — this is the master activator
- Trypsin then activates chymotrypsinogen → chymotrypsin, proelastase → elastase, and procarboxypeptidase → carboxypeptidase
- Trypsin, chymotrypsin, and elastase are endopeptidases (cut within the chain)
- Carboxypeptidase is an exopeptidase (chops amino acids from the C-terminus)
3. Brush border (intestinal mucosa):
- Aminopeptidases (exopeptidases — chop from the N-terminus) and dipeptidases complete the breakdown
- Final products: free amino acids, dipeptides, and tripeptides
Absorption:
- Free amino acids are absorbed by sodium-dependent active transport (secondary active transport using the Na+ gradient) — similar to glucose absorption
- Di- and tripeptides are absorbed by the PepT1 transporter (H+-dependent) and then hydrolysed inside the enterocyte
- Absorbed amino acids enter the portal blood and travel to the liver — the body's amino acid processing centre
Clinical pearl: Hartnup disease is a defect in the neutral amino acid transporter in the intestine and kidney. Tryptophan (the precursor of niacin) is poorly absorbed, leading to pellagra-like symptoms: dermatitis, diarrhoea, and dementia.
SELF-CHECK
A newborn screening test reveals elevated phenylalanine levels. The baby cannot convert phenylalanine to tyrosine. Phenylalanine is an essential amino acid — what does 'essential' mean in this context?
A. It is the most important amino acid for brain development
B. It cannot be synthesised by the body and must come from the diet
C. It is essential for making all other amino acids
D. It is always the first amino acid in every protein
Reveal Answer
Answer: B. It cannot be synthesised by the body and must come from the diet
An essential amino acid is one the body cannot synthesise — it must be obtained from dietary sources. There are 9 essential amino acids (PVT TIM HALL). In PKU, phenylalanine accumulates because the enzyme phenylalanine hydroxylase is deficient. A Phe-restricted diet reduces accumulation while tyrosine (normally made from Phe) must be supplemented.