Page 2 of 8
BI5.1-9 | Chemistry & Metabolism of Proteins and Immunology — SDL Guide (Part 2)
Plasma Proteins — The Blood's Dissolved Workforce (BI5.4)
Your blood plasma contains 6-8 g/dL of protein. These aren't just floating around — each one has a job. The major plasma proteins, in order of abundance:
1. Albumin (~60% of total plasma protein, 3.5-5.0 g/dL)
- Synthesised in the liver (the liver makes almost all plasma proteins except immunoglobulins)
- Functions:
- Oncotic pressure — albumin is the main protein holding water inside blood vessels. When albumin drops (liver failure, nephrotic syndrome, malnutrition), fluid leaks into tissues → oedema
- Transport — carries bilirubin, fatty acids, drugs (warfarin, diazepam), hormones (thyroid, cortisol), calcium, and metals
- Buffer — contributes to blood pH regulation
2. Globulins (~35% of total plasma protein)
Separated by serum protein electrophoresis (SPE) into:
- Alpha-1 globulins — alpha-1-antitrypsin (protects lungs from neutrophil elastase — deficiency causes emphysema), alpha-fetoprotein (AFP — elevated in hepatocellular carcinoma and neural tube defects)
- Alpha-2 globulins — haptoglobin (binds free haemoglobin — depleted in haemolysis), ceruloplasmin (copper transport — low in Wilson disease)
- Beta globulins — transferrin (iron transport), C-reactive protein (CRP — acute-phase marker), complement proteins, LDL
- Gamma globulins — immunoglobulins (IgG, IgA, IgM, IgD, IgE) — produced by plasma cells, NOT the liver
3. Fibrinogen (~5%)
- The clotting factor that is converted to fibrin during coagulation
- Present in plasma but NOT in serum (serum = plasma minus clotting factors)
Acute-phase proteins — proteins whose levels change dramatically during inflammation:
- Positive (increase): CRP (fastest responder — rises within 6 hours), fibrinogen, haptoglobin, ceruloplasmin, alpha-1-antitrypsin, ferritin
- Negative (decrease): albumin, transferrin, transthyretin (pre-albumin)
Electrophoretic patterns you must recognise:
- Normal: albumin is the tallest peak, followed by smaller alpha-1, alpha-2, beta, and gamma peaks
- Nephrotic syndrome: albumin peak dramatically reduced (lost in urine), alpha-2 and beta increased (liver compensates)
- Cirrhosis: albumin reduced, beta-gamma bridging (polyclonal gammopathy from chronic stimulation)
- Multiple myeloma: a tall, narrow spike in the gamma region (M-spike) — this is the monoclonal protein from malignant plasma cells. This is one of the most important diagnostic patterns in medicine.
Immunoglobulins — Antibodies That Fight for You (BI5.5)
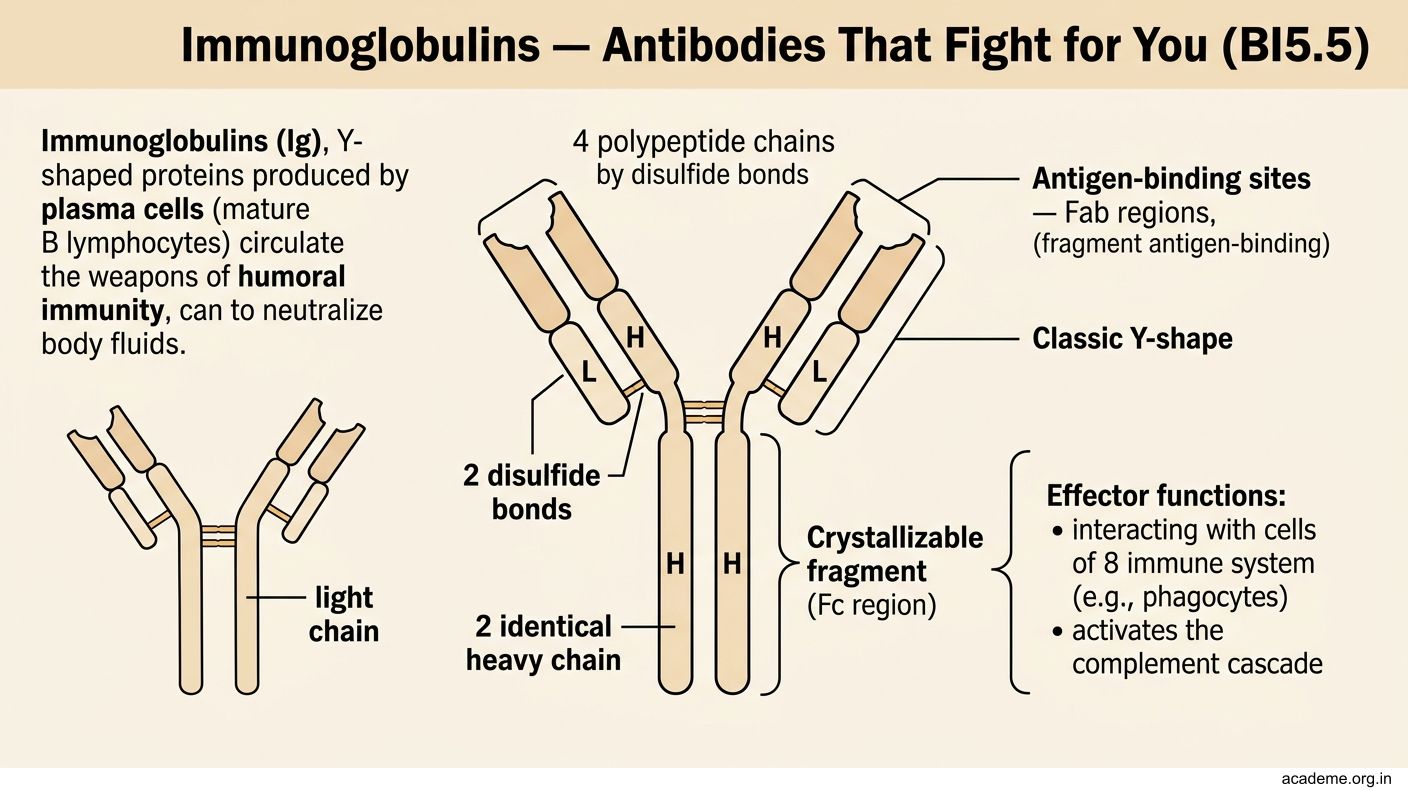
Immunoglobulins (Ig) are Y-shaped proteins produced by plasma cells (mature B lymphocytes). They are the weapons of humoral immunity — circulating in blood and body fluids, ready to neutralise pathogens.

Figure: The five classes of immunoglobulins — GAMED:

Figure: Immunoglobulins — Antibodies That Fight for You (BI5.5)
Basic structure of an antibody:
- 4 polypeptide chains: 2 identical heavy chains (H) + 2 identical light chains (L), held together by disulfide bonds
- The Y-shape has three parts:
- Two Fab regions (Fragment antigen-binding) — the two arms of the Y. Each Fab has a variable region (V) at the tip that recognises a specific antigen. This is where diversity comes from — your body can make antibodies against millions of different antigens.
- One Fc region (Fragment crystallisable) — the stem of the Y. This is the constant region that determines the class of the antibody and mediates effector functions (complement activation, binding to immune cells).
The five classes of immunoglobulins — GAMED:
| Class | Heavy chain | % of serum Ig | Key feature |
|---|---|---|---|
| IgG | Gamma (γ) | 75% | Most abundant. Crosses the placenta (protects the newborn). Only Ig that crosses the placenta. Activates complement. |
| IgA | Alpha (α) | 15% | Secretory antibody — in saliva, tears, breast milk, gut mucosa. Dimer with J-chain + secretory component. First line of mucosal defence. |
| IgM | Mu (μ) | 10% | First antibody produced in a primary immune response. Pentamer (5 units joined by J-chain). Most efficient complement activator. Too large to cross the placenta — if IgM is found in a newborn, it means the baby made it (intrauterine infection). |
| IgE | Epsilon (ε) | Trace | Allergic reactions and parasitic infections. Binds to mast cells via Fc → triggers histamine release on antigen exposure → anaphylaxis, asthma, allergic rhinitis. |
| IgD | Delta (δ) | Trace | Surface receptor on mature B cells. Exact function still debated. |
Humoral vs cellular immunity — the two arms of adaptive immunity:
- Humoral (B cells → plasma cells → antibodies): targets extracellular pathogens (bacteria in blood, toxins, viruses before they enter cells)
- Cellular (T cells): targets intracellular pathogens (viruses inside cells, cancer cells, transplant rejection). CD4+ helper T cells coordinate, CD8+ cytotoxic T cells kill.
Clinical pearl: Bruton's agammaglobulinaemia — an X-linked disorder where B cells fail to mature (defective Bruton tyrosine kinase). No antibodies are produced. These boys get recurrent bacterial infections after 6 months of age (when maternal IgG wanes). Treatment: lifelong IV immunoglobulin (IVIG).
Ammonia Metabolism — Detoxifying a Deadly Waste Product (BI5.6)
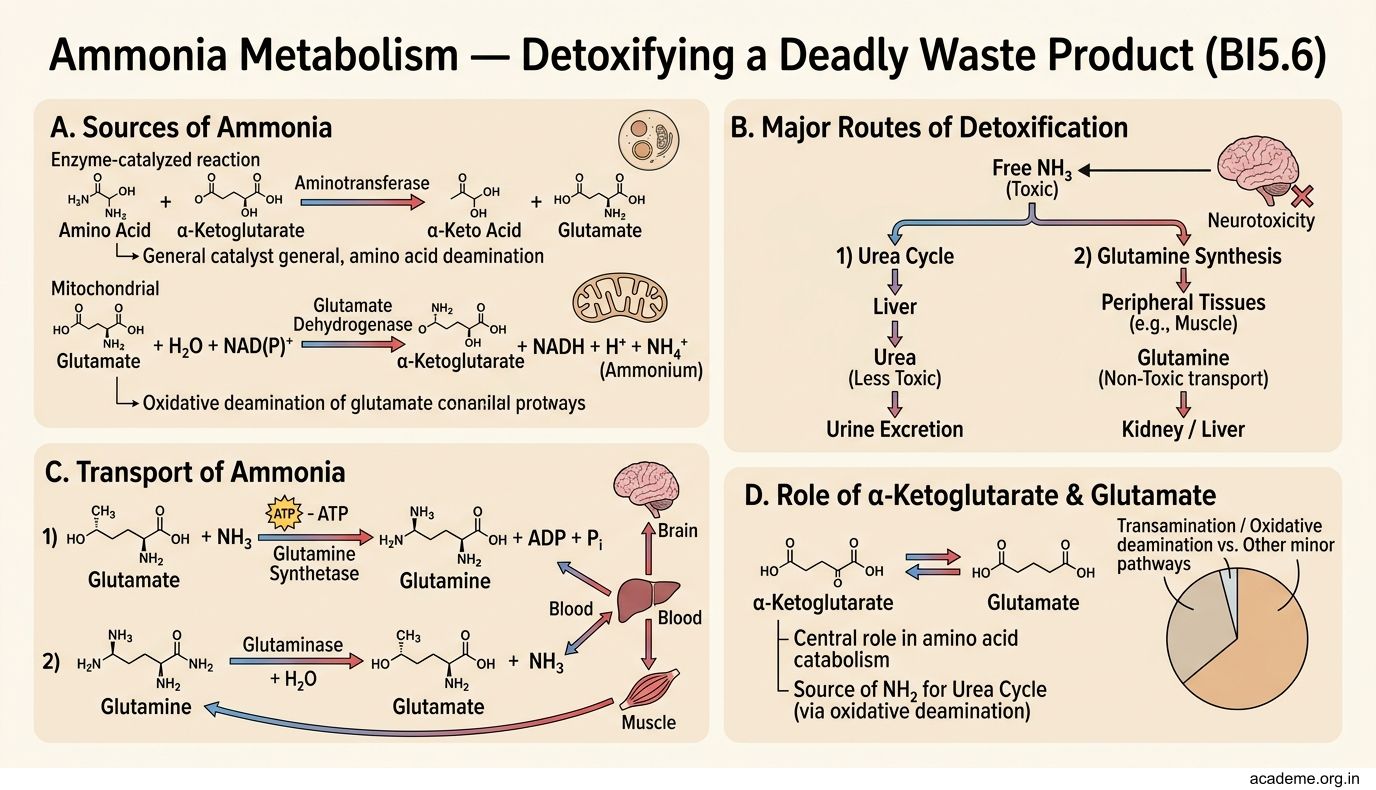
When amino acids are broken down, the amino group (-NH2) is removed — a process called deamination. This releases ammonia (NH3), which is extremely toxic to the brain. Your body must detoxify ammonia constantly, and the urea cycle in the liver is the main route.

Figure: Ammonia Metabolism — Detoxifying a Deadly Waste Product (BI5.6)
Sources of ammonia:
1. Transamination + oxidative deamination — amino acids transfer their amino group to alpha-ketoglutarate (→ glutamate) via transaminases, then glutamate dehydrogenase removes the amino group as free NH3
2. Bacterial action in the gut — intestinal bacteria deaminate amino acids and produce ammonia (this is why liver failure patients are given lactulose — to reduce gut ammonia absorption)
3. Purine/pyrimidine degradation — releases ammonia
4. Amino acid deamination in kidney — glutaminase converts glutamine → glutamate + NH3 (the NH3 is excreted in urine to maintain acid-base balance)
Transport of ammonia:
Free ammonia is toxic, so it travels in the blood safely as:
- Glutamine (glutamate + NH3, catalysed by glutamine synthetase) — the main transport form in blood. Muscle releases glutamine; liver and kidney take it up.
- Alanine (from the glucose-alanine cycle in muscle) — pyruvate picks up the amino group in muscle → alanine → travels to liver → pyruvate regenerated → used for gluconeogenesis, while NH3 enters the urea cycle
The urea cycle (Krebs-Henseleit cycle) — occurs in the liver (partly in mitochondria, partly in cytoplasm):
- Carbamoyl phosphate synthetase I (CPS-I) — combines CO2 + NH3 + 2 ATP → carbamoyl phosphate (mitochondria). This is the rate-limiting step, activated by N-acetylglutamate (NAG).
- Carbamoyl phosphate + ornithine → citrulline (ornithine transcarbamylase, in mitochondria)
- Citrulline + aspartate → argininosuccinate (argininosuccinate synthetase, in cytoplasm — this step brings in the second nitrogen atom)
- Argininosuccinate → arginine + fumarate (argininosuccinate lyase)
- Arginine → urea + ornithine (arginase — ornithine re-enters the cycle)
Net equation: 2 NH3 + CO2 + 3 ATP → urea + water + 2 ADP + AMP
Urea has TWO nitrogen atoms — one from free ammonia (step 1) and one from aspartate (step 3). Urea is non-toxic, water-soluble, and excreted by the kidneys.
Hyperammonaemia — when the system fails:
Causes: liver failure (most common), urea cycle enzyme deficiencies (rare, genetic)
Symptoms: vomiting, lethargy, cerebral oedema, seizures, coma → death if untreated
Mechanism of brain toxicity: excess NH3 + alpha-ketoglutarate → glutamate → glutamine (accumulates in astrocytes, causing osmotic swelling)
Treatment: restrict protein, give lactulose (traps NH3 in gut as NH4+), sodium benzoate/phenylbutyrate (alternative pathways for nitrogen excretion)
SELF-CHECK
A patient with advanced liver cirrhosis develops confusion and lethargy. Blood ammonia levels are markedly elevated. Lactulose is prescribed. How does lactulose reduce blood ammonia?
A. It directly binds ammonia in the blood and converts it to urea
B. It stimulates the urea cycle enzymes in the liver
C. It acidifies the colonic contents, trapping ammonia as NH4+ which is excreted in faeces
D. It increases renal excretion of ammonia by alkalinising the urine
Reveal Answer
Answer: C. It acidifies the colonic contents, trapping ammonia as NH4+ which is excreted in faeces
Lactulose is metabolised by colonic bacteria to organic acids, lowering the pH of the colon. At acidic pH, ammonia (NH3) is protonated to ammonium (NH4+), which is charged and cannot cross the colonic mucosa back into the blood. It is trapped in the gut lumen and excreted in faeces. Lactulose also acts as an osmotic laxative, speeding up faecal elimination.