Page 1 of 13
CM12.1-2 | CM12.1-2 | Geriatric Services and Health Problems — SDL Guide
Learning Objectives
- Define geriatrics and describe the concept of organised geriatric services
- Explain the magnitude of ageing as a demographic and public-health challenge in India
- Describe the major physical, mental, and psychosocial health problems of the aged
- Identify the determinants of health and vulnerability specific to the elderly
- Apply the concept of functional assessment (ADL/IADL, geriatric giants) to community settings
INSTRUCTIONS
India is ageing rapidly — by 2050, one in five Indians will be elderly. Yet most medical graduates encounter older patients as incidentals to another specialty rather than as a distinct population with unique needs. This module establishes why geriatrics deserves its own framework, what diseases and syndromes disproportionately burden older adults, and how organised geriatric services differ from simply 'treating old people.' The competencies here (CM12.1 and CM12.2) form the definitional and epidemiological foundation for the preventive and programme content that follows.
References
- Park K. Park's Textbook of Preventive and Social Medicine, 26th ed. Ch. 12 — Health in Old Age (textbook)
- Longitudinal Ageing Study in India (LASI) Wave 1, 2017-18. International Institute for Population Sciences, Mumbai (survey)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 72-year-old retired schoolteacher presents to the PHC with 'weakness and forgetfulness.' His daughter says he has fallen twice in the last month, stopped cooking for himself, and is 'not the same since his wife died.' His blood pressure today is 158/96 mmHg and his grip strength is markedly reduced. The junior doctor is unsure whether to refer him to medicine, neurology, psychiatry, or none of these — and the PHC has no geriatric specialist. As you read through this case, ask yourself: is this man's problem one disease, or is it something more fundamental about how old age presents?
WHY THIS MATTERS
India entered the 'ageing society' threshold in the 2010s and will reach 'aged society' status by the 2040s. The 2021 census estimates roughly 140 million Indians are elderly (≥60 years) — a number that will reach 300 million by 2050. These older adults carry the highest burden of non-communicable disease, the highest disability-adjusted life-years lost to functional decline, and the greatest unmet need for organised care. Yet medical curricula historically trained graduates for an acute-disease model built around younger patients. Understanding geriatrics — its definition, scope, and the specific health problems that cluster in old age — is no longer a sub-specialty luxury; it is core public-health competency for every graduating doctor who will work in India's community health system.
RECALL
Before exploring geriatric-specific content, bring forward three concepts from earlier learning. First, the epidemiological transition: India has moved from infectious to non-communicable disease dominance, and the elderly population is the leading edge of this shift — they bear the full NCDs burden accumulated over a lifetime. Second, the social determinants of health: poverty, education, housing, and social support affect health outcomes across the life course and are amplified in old age when income stops and social networks shrink. Third, the levels of prevention (Leavell and Clark) — primary, secondary, tertiary — which will reappear when we discuss how geriatric services are organised around these levels. Connect these frameworks as you read.
The Ageing Population: Magnitude and Demographic Shift
Demographic ageing refers to the process by which the proportion of older persons in a population increases relative to younger age groups. It is driven by two parallel forces: falling fertility rates (reducing the young base of the population pyramid) and falling mortality rates at older ages (expanding the elderly apex). India is experiencing both simultaneously, producing a characteristic narrowing at the base and widening at the top of the age pyramid — a shift visible when comparing the 2001 and 2021 censuses.
At the global level, the United Nations projects that by 2050, the world will have more people over 65 than under 15 for the first time in history — a demographic first with profound implications for health systems, pension structures, and caregiving. For India specifically, the elderly population (≥60 years) numbered approximately 77 million in 2001, grew to roughly 104 million by 2011, and is estimated at 140 million in 2021. Projections consistently place this number at 300 million by 2050 — nearly one-fifth of India's expected population.
The old-age dependency ratio — the number of elderly per 100 working-age adults (aged 15–64) — is a policy-critical indicator. As this ratio rises, every working adult must support more older dependents, straining pension systems, health budgets, and informal family caregiving structures. India's dependency ratio is rising but remains lower than East Asian countries (Japan's exceeds 50), giving India a window to build geriatric infrastructure before the peak arrives.
Why does this matter for health? Older adults have a higher burden of multi-morbidity (≥2 chronic conditions simultaneously), higher rates of disability, higher hospitalisation costs per episode, and longer lengths of stay. They are disproportionately under-represented in clinical trial evidence yet over-represented in actual patients. Recognising that ageing is not a crisis to be managed but a transition to be planned for is the starting point of geriatric public health.
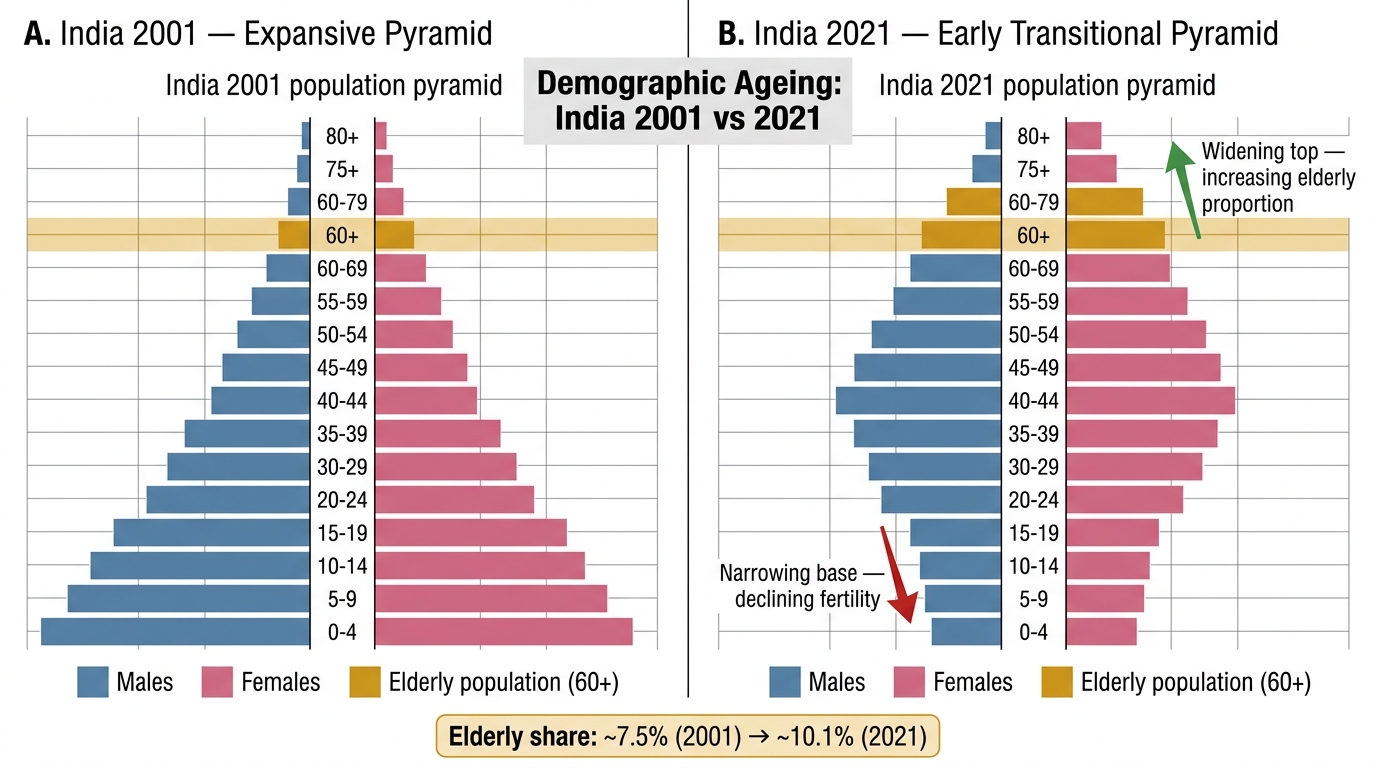
India Population Pyramids 2001 vs 2021: Demographic Ageing Transition
Key facts (Park, 26th ed.): India has the second-largest elderly population globally after China. The sex ratio among the elderly favours women in urban areas; rural areas often see the reverse due to male out-migration. Life expectancy at birth in India reached approximately 70 years in 2022, but healthy life expectancy (disability-free years) remains considerably lower, highlighting the compression-of-morbidity challenge.
Defining Geriatrics and Geriatric Services
Geriatrics is the branch of medicine that deals with the clinical, preventive, rehabilitative, and social aspects of illness in old age. It is distinguished from other medical specialties not simply by patient age but by the complexity of multi-morbidity, polypharmacy, the dominance of functional over diagnostic endpoints, and the critical role of social context in determining outcomes. The term was coined by Ignatz Leo Nascher in 1909 — a deliberate parallel to 'pediatrics,' recognising old age as a physiologically distinct phase deserving its own clinical science.
Geriatric services are the organised systems of health-care delivery designed to meet the needs of the elderly population. The World Health Organization defines geriatric services as those providing: (i) clinical assessment and management, (ii) rehabilitation to maintain or restore function, (iii) long-term or continuing care, and (iv) palliative and end-of-life care — delivered by multidisciplinary teams across different levels of the health system (community, primary, secondary, tertiary).
The cornerstone of geriatric services is the Comprehensive Geriatric Assessment (CGA) — a multidimensional, interdisciplinary diagnostic process used to determine the medical, psychological, and functional capabilities and limitations of an older person. The CGA is not a single test but a structured framework that assesses: (a) medical problems and medications (polypharmacy review), (b) cognitive function (dementia screening), (c) mood and mental health (depression screening), (d) functional status (ADL/IADL), (e) mobility and fall risk, (f) nutritional status, (g) social circumstances and support, and (h) environmental safety. Evidence shows that patients assessed via CGA have better functional outcomes, reduced hospital admissions, and lower mortality compared to usual care.
Geriatric services differ from simply 'treating old patients' in several important ways. First, the goal is functional — maintaining independence and quality of life, not just diagnosing and curing disease. Second, the team is multidisciplinary — physicians, nurses, physiotherapists, occupational therapists, social workers, and pharmacists contribute to the plan. Third, the setting is diverse — geriatric services operate in outpatient clinics, inpatient wards, day hospitals, nursing homes, home visits, and community programmes. Understanding this range is essential to designing an effective geriatric care system at national scale.
Determinants of Health and Vulnerability in the Elderly
Health in old age is not simply the accumulation of disease but the product of a lifetime of biological, social, and environmental exposures interacting with the ageing process itself. Understanding the determinants of vulnerability in the elderly is essential for designing interventions that are targeted rather than generic.
Biological determinants include the physiological changes of normal ageing: reduced organ reserve (diminished cardiac output, reduced renal glomerular filtration rate, decreased lung vital capacity), immunosenescence (reduced immune response increasing infection risk), sarcopenia (progressive loss of skeletal muscle mass and strength), osteoporosis, and the altered pharmacokinetics and pharmacodynamics that make the elderly highly susceptible to drug adverse effects. These changes reduce the elderly person's ability to respond to physiological stress — what geriatricians call reduced homeostenosis. Even a minor insult (a urinary tract infection, a missed dose of antihypertensive medication) can trigger a cascade of functional decline in an older person that would be trivial in a younger adult.
Social determinants that are amplified in old age include: poverty and fixed income (retirement eliminates earning capacity, while healthcare costs rise), social isolation (bereavement, children moving away, reduced mobility), caregiver burden and its reverse — caregiver absence, educational attainment (lower education is associated with higher dementia risk and lower health literacy), and ageism — the systematic devaluation of older people that affects how they access care, how vigorously they are treated, and their own health behaviours. Elder abuse — physical, psychological, financial, or by neglect — is an underreported but prevalent social determinant; Indian studies suggest prevalence of 20–50% depending on the setting.
Environmental determinants include housing safety (stairs, poor lighting, absent grab rails — the home environment contributes to fall risk), access to primary care (transport barriers, long waiting times, providers who lack geriatric training), and the rural-urban divide (rural elderly face additional challenges: longer travel to health facilities, fewer specialist services, greater dependence on overburdened family caregivers). Climate is an emerging determinant — heat waves disproportionately kill the elderly, who have impaired thermoregulation.
The interaction of these determinants produces the concept of frailty — a state of increased vulnerability to stressors resulting from the cumulative decline of multiple physiological systems. Frailty is distinct from chronological age and from specific diseases; it is the best single predictor of adverse outcomes in elderly care.